


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of Action: MVASI (bevacizumab) is a recombinant humanised monoclonal antibody that selectively binds to and neutralises the biologic activity of human vascular endothelial growth factor (VEGF). Bevacizumab contains human framework regions with antigen binding regions of a humanised murine antibody that binds to VEGF. Bevacizumab is a recombinant humanised monoclonal antibody produced by DNA technology in Chinese Hamster Ovary cells. Bevacizumab consists of 214 amino acids and has a molecular weight of approximately 149,000 daltons.
Bevacizumab inhibits the binding of VEGF to its receptors, Flt-1 and KDR, on the surface of endothelial cells. Neutralising the biologic activity of VEGF reduces the vascularisation of tumours, thereby inhibiting tumour growth. Administration of bevacizumab or its parental murine antibody to xenotransplant models of cancer in nude mice resulted in extensive anti-tumour activity in human cancers, including colon, breast, pancreas and prostate. Metastatic disease progression was inhibited and microvascular permeability was reduced.
Clinical/Efficacy Studies: All studies performed in every single indication as approved are referring to the studies conducted by AVASTIN.
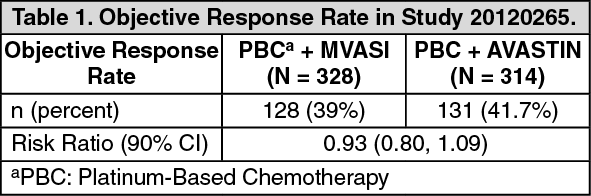
Efficacy data for MVASI: Comparative Study between MVASI and AVASTIN (Study 20120265): Clinical equivalence was demonstrated between MVASI and AVASTIN in Study 20120265. The data as follows (Table 1) reflect exposure to MVASI in 328 patients with non-squamous NSCLC treated at the doses and schedules described as follows for a median of 6 doses of MVASI and 6 doses of AVASTIN, respectively.
Subjects in Study 20120265 were randomized in a 1:1 ratio to treatment consisting of: Arm 1: MVASI at a dose of 15 mg/kg administered as an IV infusion every 3 weeks for 6 cycles, plus carboplatin and paclitaxel chemotherapy every 3 weeks for at least 4 and not more than 6 cycles, or;
Arm 2: AVASTIN at a dose of 15 mg/kg administered as an IV infusion every 3 weeks for 6 cycles, plus carboplatin and paclitaxel chemotherapy every 3 weeks for at least 4 and not more than 6 cycles.
Subjects remained in the treatment phase until 21 days after the last dose of investigational product or study-specified chemotherapy. After completing the end-of-treatment (EOT) visit, subjects were followed for disease progression and overall survival (OS) every 9 weeks until the clinical study ended, consent was withdrawn, or they were lost to follow-up, died, or received prescribed therapy (e.g., commercial bevacizumab, non-study anticancer treatment).
For MVASI and AVASTIN, the median age was 62 and 63 years, respectively, 40.2% and 40.1% were female, 5.8% and 7.6% had recurrent disease, and 94.2% and 92.4% had Stage IV disease.
The primary endpoint was the risk ratio (RR) of the ORR (partial response or complete response as defined by RECIST v1.1). Clinical similarity was demonstrated by comparing the two-sided 90% confidence interval of the ORR risk ratio between MVASI and AVASTIN. There were no clinically meaningful differences in ORR between bevacizumab and MVASI in Study 20120265 as evidenced by the similar ORR observed for MVASI and AVASTIN (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageClinical similarity of MVASI and AVASTIN was further confirmed by duration of response (DOR) as well as PFS analysis in Study 20120265. DOR was defined as time from the first objective response (partial response or complete response) to disease progression. The estimated DOR for subjects in MVASI group was 5.8 months (95% CI: 4.9, 7.7) versus 5.6 months (95% CI: 5.1, 6.3) for subjects in AVASTIN group. Progression-free survival was defined as the time from the randomization date to the date of disease progression or death. The estimated hazard ratio (MVASI relative to AVASTIN) was 1.03 (90% CI: 0.83, 1.29).
Immunogenicity: In Study 20120265 in patients with advanced non-small cell lung cancer, using an immunoassay, the incidence of antibodies to MVASI was found to be similar to AVASTIN. The number of subjects developing binding antibodies during the study were four (1.4%) for those receiving MVASI versus seven (2.5%) for those receiving AVASTIN. Among these subjects, no subject in either treatment group tested positive for neutralizing antibodies. The clinical significance of these anti-product antibody responses to MVASI is unknown.
Immunogenicity assay results are highly dependent on the sensitivity and specificity of the test method and may be influenced by several factors, including sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to MVASI with the incidence of antibodies to other products may be misleading.
As with all therapeutic proteins, there is potential for immunogenicity. Differences in assay methodology for measuring immunogenicity prevent direct comparison of immunogenicity rates between MVASI and AVASTIN or other biologics in different studies. In 20120265, binding anti-drug antibodies (ADA) activity was determined using electrochemiluminescence (ECL)-based bridging immunoassay to detect antibodies capable of binding to MVASI and the neutralizing ADA activity was determined using a non-cell-based target binding assay.
Metastatic Colorectal Cancer (mCRC): The safety and efficacy of the recommended dose of AVASTIN (5 mg/kg of body weight every two weeks) in metastatic carcinoma of the colon or rectum were studied in three randomised, active-controlled clinical trials in combination with fluoropyrimidine-based first-line chemotherapy. AVASTIN was combined with two chemotherapy regimens: AVF2107g: A weekly schedule of irinotecan/bolus 5-fluorouracil/leucovorin (IFL regimen) for a total of 4 weeks of each 6 week cycle.
AVF0780g: In combination with bolus 5-fluorouracil/leucovorin (5-FU/LV) for a total of 6 weeks of each 8 week cycle (Roswell Park regimen).
AVF2192g: In combination with bolus 5-fluorouracil/leucovorin (5-FU/LV) for a total of 6 weeks of each 8 week-cycle (Roswell Park regimen) in patients who were not optimal candidates for first-line irinotecan treatment.
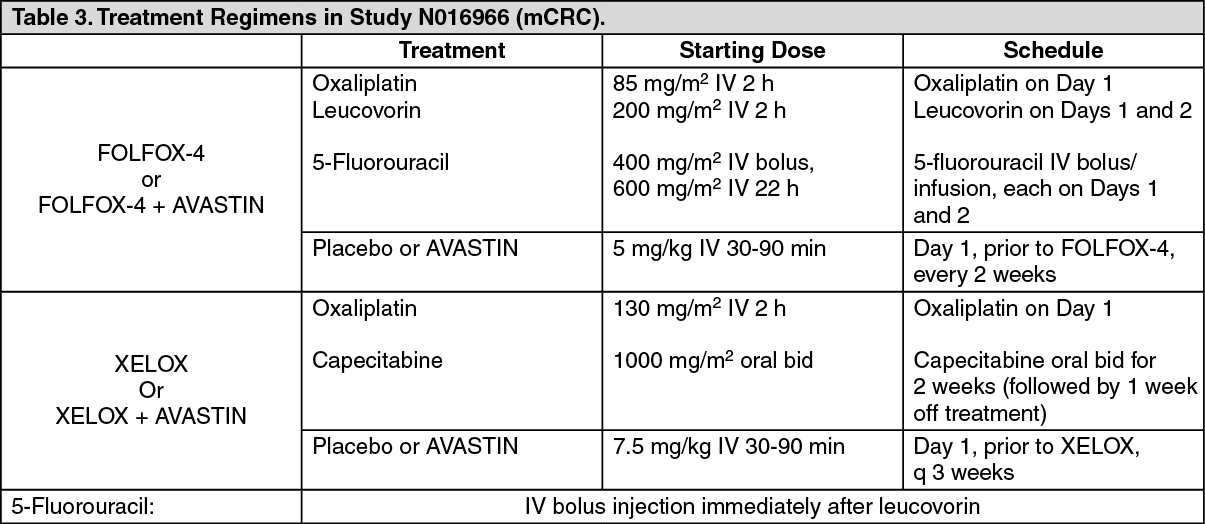
Three additional studies with AVASTIN have been conducted in mCRC patients: first-line (NO16966), second-line with no previous AVASTIN treatment (E3200), and second-line with previous AVASTIN treatment following disease progression in first-line (ML18147). In these studies, AVASTIN was administered at the following dosing regimens, in combination with FOLFOX-4 (5FU/LV/Oxaliplatin), XELOX (Capecitabine/Oxaliplatin) and fluoropyrimidine/irinotecan and fluoropyrimidine/oxaliplatin: NO16966: AVASTIN 7.5 mg/kg of body weight every 3 weeks in combination with oral capecitabine and intravenous oxaliplatin (XELOX) or AVASTIN 5 mg/kg every 2 weeks in combination with leucovorin plus 5-fluorouracil bolus, followed by 5-fluorouracil infusion, with intravenous oxaliplatin (FOLFOX-4).
E3200: AVASTIN 10 mg/kg of body weight every 2 weeks in combination with leucovorin and 5-fluorouracil bolus, followed by 5-fluorouracil infusion, with intravenous oxaliplatin (FOLFOX-4) in AVASTIN naïve patients.
ML18147: AVASTIN 5.0 mg/kg of body weight every 2 weeks or AVASTIN 7.5 mg/kg of body weight every 3 weeks in combination with fluoropyrimidine/irinotecan or fluoropyrimidine/oxaliplatin in patients with disease progression following first-line treatment with AVASTIN. Use of irinotecan- or oxaliplatin-containing regimen was switched depending on first-line usage of either oxaliplatin or irinotecan.
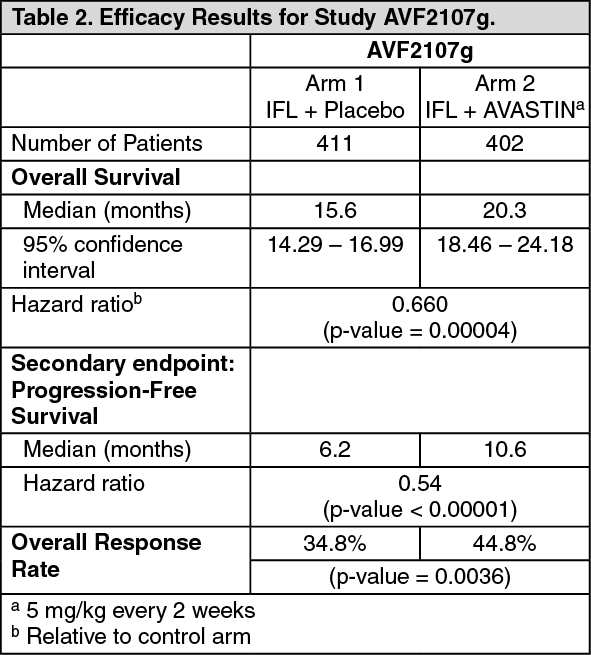
AVF2107g: This was a phase III randomised, double-blind, active-controlled clinical trial evaluating AVASTIN in combination with IFL as first-line treatment for metastatic carcinoma of the colon or rectum. Eight hundred and thirteen patients were randomised to receive IFL + placebo (Arm 1) or IFL + AVASTIN (5 mg/kg every 2 weeks, Arm 2). A third group of 110 patients received bolus 5-FU/LV + AVASTIN (Arm 3). Enrolment in Arm 3 was discontinued, as pre-specified, once safety of AVASTIN with the IFL regimen was established and considered acceptable.
The primary efficacy parameter of the trial was overall survival. The addition of AVASTIN to IFL resulted in a statistically significant increase in overall survival, progression-free survival and overall response rate (see Table 2 for details). The clinical benefit of AVASTIN, as measured by survival, was seen in all pre-specified patient subgroups, including those defined by age, sex, performance status, location of primary tumour, number of organs involved, and duration of metastatic disease. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAmong the 110 patients randomised to Arm 3 (5-FU/LV + AVASTIN) prior to discontinuation of this arm, the median overall survival was 18.3 months, and the median progression free survival was 8.8 months.
AVF2192g: This was a phase II randomised, double-blind, active-controlled clinical trial investigating AVASTIN in combination with 5-FU/leucovorin as first-line treatment for metastatic colorectal cancer in patients who were not optimal candidates for first-line irinotecan treatment. One hundred and five patients were randomised to 5-FU/LV + placebo arm and 104 patients randomised to 5-FU/LV AVASTIN (5 mg/kg every 2 weeks). All treatments were continued until disease progression.
The addition of AVASTIN 5 mg/kg every two weeks to 5-FU/LV resulted in higher objective response rates, significantly longer progression-free survival, and a trend in longer survival as compared with 5-FU/LV chemotherapy alone.
NO16966: This was a phase III randomised, double-blind (for bevacizumab), clinical trial investigating AVASTIN 7.5 mg/kg in combination with oral capecitabine and i.v. oxaliplatin (XELOX), administered on a 3-weekly schedule; or bevacizumab 5 mg/kg in combination with leucovorin with 5-fluorouracil bolus, followed by 5-fluorouracil infusional, with i.v. oxaliplatin (FOLFOX-4), administered on a 2-weekly schedule. The study contained two parts: an initial unblinded 2-arm part (Part I) in which patients were randomised to two different treatment groups (XELOX and FOLFOX-4) and a subsequent 2 x 2 factorial 4-arm part (Part II) in which patients were randomised to four treatments groups (XELOX + placebo, FOLFOX-4 + placebo, XELOX + AVASTIN, FOLFOX-4 + AVASTIN). In Part II, treatment assignment was double-blind with respect to AVASTIN. Approximately 350 patients were randomised into each of the 4 study arms in the Part II of the trial. (See Table 3.)
 Click on icon to see table/diagram/image
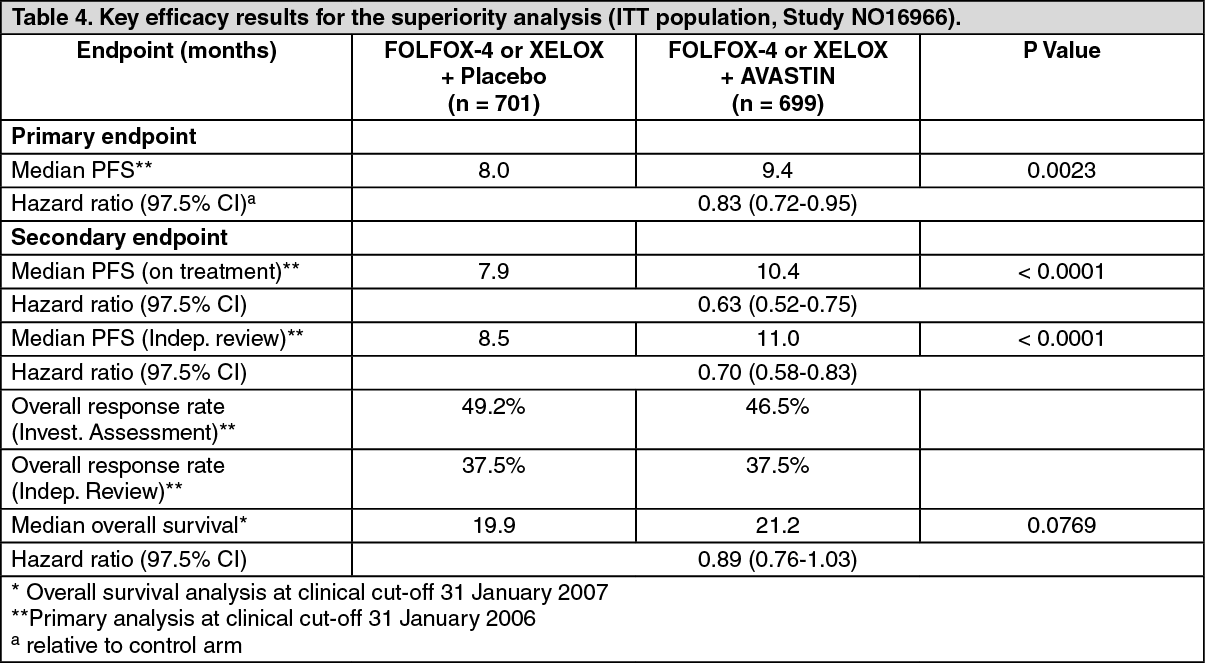
Click on icon to see table/diagram/imageThe primary efficacy parameter of the trial was the duration of progression-free survival. In this study, there were two primary objectives: to show that XELOX was non-inferior to FOLFOX-4 and to show that AVASTIN in combination with FOLFOX-4 or XELOX chemotherapy was superior to chemotherapy alone. Both co-primary objectives were met: i) Non-inferiority of the XELOX-containing arms compared with the FOLFOX-4 containing arms in the overall comparison was demonstrated in terms of progression-free survival and overall survival in the eligible per-protocol population.
ii) Superiority of the AVASTIN-containing arms versus the chemotherapy alone arms in the overall comparison was demonstrated in terms of progression-free survival in the ITT population (Table 4).
Secondary PFS analyses, based on Independent Review Committee (IRC)- and 'on-treatment'-based response assessments, confirmed the significantly superior clinical benefit for patients treated with AVASTIN (subgroup analyses shown in Table 4), consistent with the statistically significant benefit observed in the pooled analysis. (See Table 4.)
 Click on icon to see table/diagram/image
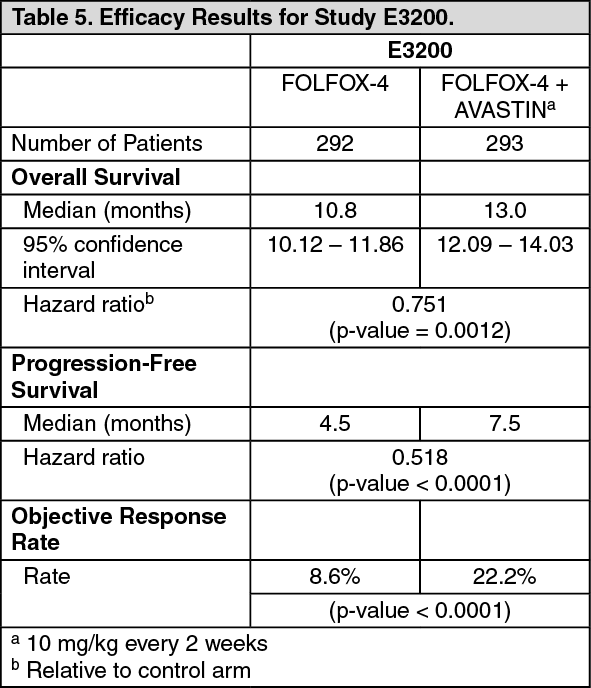
Click on icon to see table/diagram/imageECOG E3200: This was a phase III randomised, active-controlled, open-label study investigating AVASTIN 10 mg/kg in combination with leucovorin 5-fluorouracil bolus and then 5-fluorouracil infusional, with iv oxaliplatin (FOLFOX-4), administered on a 2-weekly schedule in previously-treated patients (second line) with advanced colorectal cancer. In the chemotherapy arms, the FOLFOX-4 regimen used the same doses and schedule as shown in Table 3 for Study NO16966.
The primary efficacy parameter of the trial was overall survival, defined as the time from randomisation to death from any cause. Eight hundred and twenty-nine patients were randomised (292 FOLFOX-4, 293 bevacizumab + FOLFOX-4 and 244 AVASTIN monotherapy). The addition of AVASTIN to FOLFOX-4 resulted in a statistically significant prolongation of survival. Statistically significant improvements in progression-free survival and objective response rate were also observed (see Table 5).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNo significant difference was observed in the duration of overall survival between patients who received AVASTIN monotherapy compared to patients treated with FOLFOX-4. Progression-free survival and objective response rate were inferior in the AVASTIN monotherapy arm compared to the FOLFOX-4 arm.
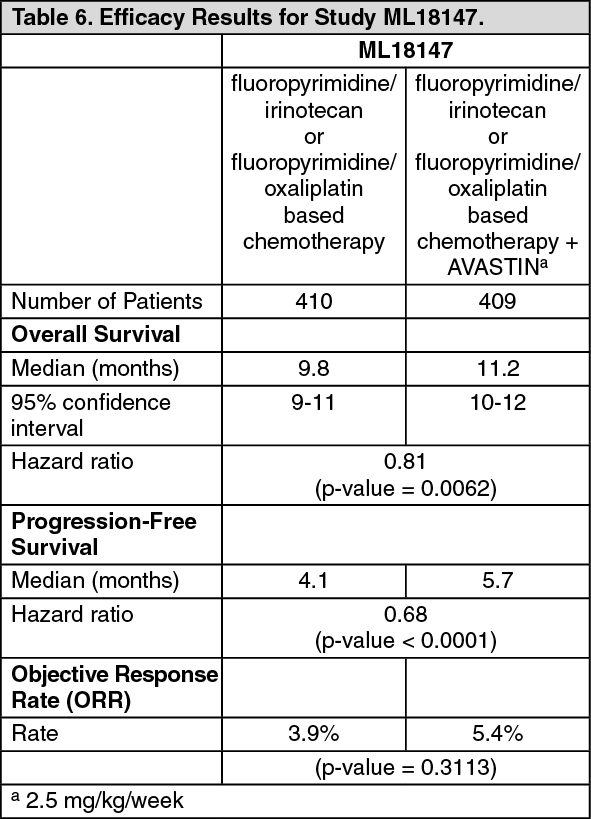
ML18147: This was a Phase III randomised, controlled, open-label trial investigating AVASTIN 5.0 mg/kg every 2 weeks or 7.5 mg/kg every 3 weeks in combination with fluoropyrimidine-based chemotherapy versus fluoropyrimidine-based chemotherapy alone in patients with metastatic colorectal cancer who have progressed on a first-line AVASTIN-containing regimen.
Patients with histologically confirmed mCRC and disease progression were randomised 1:1 within 3 months after discontinuation of AVASTIN first-line therapy to receive fluoropyrimidine/oxaliplatin or fluoropyrimidine/irinotecan-based chemotherapy (chemotherapy switched depending on first-line chemotherapy) with or without AVASTIN. Treatment was given until progressive disease or unacceptable toxicity. The primary outcome measure was overall survival (OS) defined as the time from randomisation until death from any cause.
A total of 820 patients were randomised. The addition of AVASTIN to fluoropyrimidine-based chemotherapy resulted in a statistically significant prolongation of survival in patients with metastatic colorectal cancer who have progressed on a first-line AVASTIN-containing regimen (ITT = 819) (see Table 6).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageStatistically significant improvements in progression-free survival were also observed. Objective response rate was low in both treatment arms and did not meet statistical significance.
Adjuvant Colon Cancer (aCC): BO17920: This was a phase III randomised open-label, 3-arm study evaluating the efficacy and safety of AVASTIN administered at a dose equivalent to 2.5 mg/kg/week on either a 2-weekly schedule in combination with FOLFOX-4, or on a 3-weekly schedule in combination with XELOX versus FOLFOX-4 alone as adjuvant chemotherapy in 3451 patients with high-risk stage II and stage III colon carcinoma.
More relapses and deaths due to disease progression were observed in both bevacizumab arms compared to the control arm. The primary objective of prolonging disease free survival (DFS) in patients with stage III colon cancer (n = 2867) by adding AVASTIN to either chemotherapy regimen was not met. The hazard ratios for DFS were 1.17 (95% CI: 0.98-1.39) for the FOLFOX-4 + AVASTIN arm and 1.07 (95% CI: 0.91-1.28) for the XELOX + AVASTIN arm.
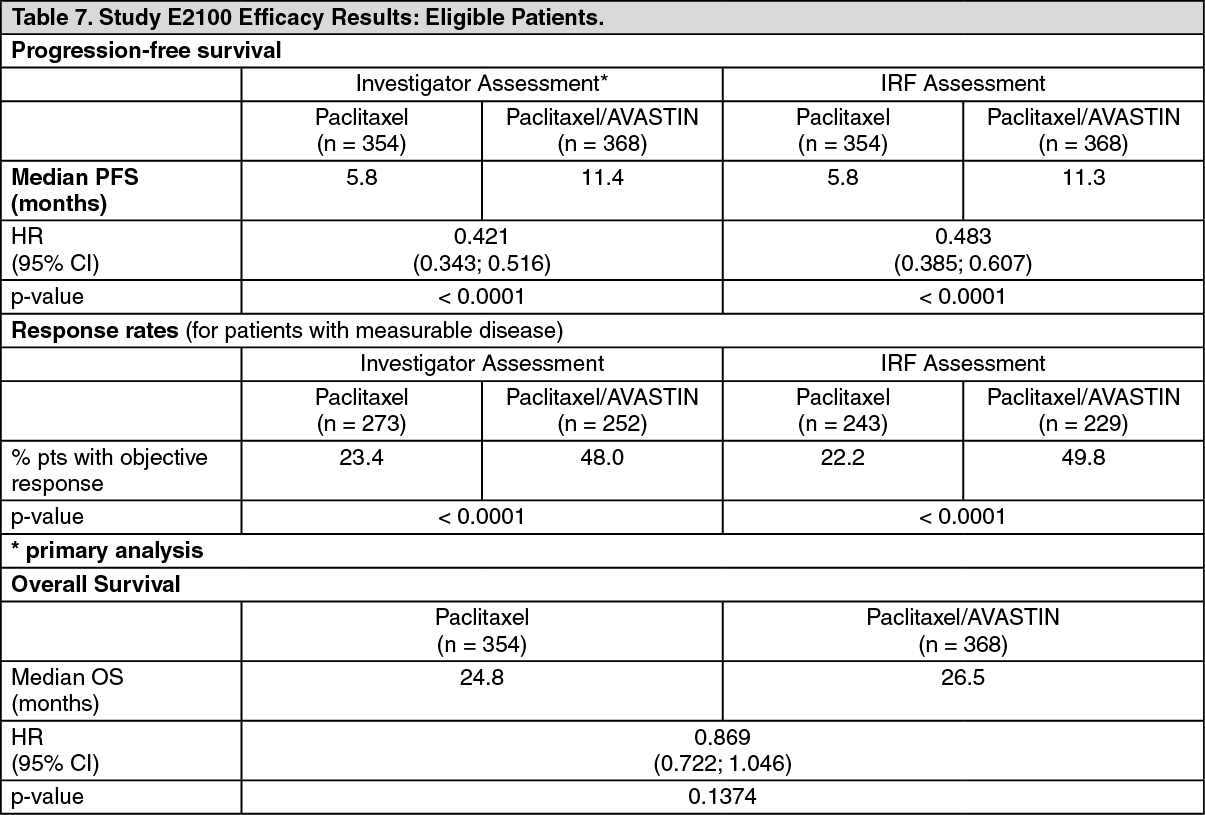
Metastatic Breast Cancer (mBC): ECOG E2100: E2100 was an open-label, randomised, active controlled, multicentre clinical trial evaluating AVASTIN in combination with paclitaxel for locally recurrent or metastatic breast cancer in patients who had not previously received chemotherapy for locally recurrent and metastatic disease. Prior hormonal therapy for the treatment of metastatic disease was allowed. Adjuvant taxane therapy was allowed only if it was completed at least 12 months prior to study entry. Patients were randomised to paclitaxel alone (90 mg/m2 IV over 1 hour once weekly for three out of four weeks) or in combination with AVASTIN (10 mg/kg IV infusion every two weeks). Patients were to continue assigned study treatment until disease progression. In cases where patients discontinued chemotherapy prematurely, treatment with AVASTIN as a single agent was continued until disease progression. The primary endpoint was progression free survival (PFS), as assessed by investigators. In addition, an independent review of the primary endpoint was also conducted.
Of the 722 patients in the study, the majority of patients (90%) had HER2-negative disease. A small number of patients had HER-2 receptor status that was either unknown (8%) or positive (2%). Patients who were HER-2 positive had either received previous treatment with trastuzumab or were considered unsuitable for trastuzumab. The majority (65%) of patients had received adjuvant chemotherapy including 19% who had prior taxanes and 49% who had prior anthracyclines. The patient characteristics were similar between the study arms.
The results of this study are presented in Table 7. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdvanced, metastatic or recurrent Non-Small Cell Lung Cancer (NSCLC): The safety and efficacy of AVASTIN in the first-line treatment of patients with non-small cell lung cancer (NSCLC) other than predominantly squamous cell histology, was studied in addition to platinum-based chemotherapy in studies E4599 and BO17704.
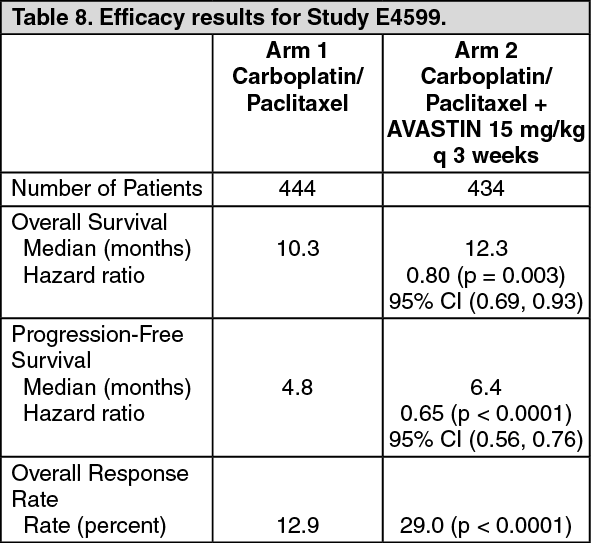
E4599: E4599 was an open-label, randomised, active-controlled, multicentre clinical trial evaluating AVASTIN as first-line treatment of patients with locally advanced, metastatic or recurrent NSCLC other than predominantly squamous cell histology.
Patients were randomised to platinum-based chemotherapy (paclitaxel 200 mg/m2 and carboplatin AUC = 6.0, both by IV infusion) (PC) on day 1 every 3-week cycle for up to 6 cycles or PC in combination with AVASTIN at a dose of 15 mg/kg IV infusion day 1 of every 3-week cycle. After completion of six cycles of carboplatin-paclitaxel chemotherapy or upon premature discontinuation of chemotherapy, patients on the AVASTIN + carboplatin-paclitaxel arm continued to receive AVASTIN as a single agent every 3 weeks until disease progression. 878 patients were randomised to the two arms.
During the study, of the patients who received trial treatment, 32.2% (136/422) of patients received 7-12 administrations of AVASTIN and 21.1% (89/422) of patients received 13 or more administrations of AVASTIN. The primary endpoint was duration of survival. Results are presented in Table 8. (See Table 8.)
 Click on icon to see table/diagram/image
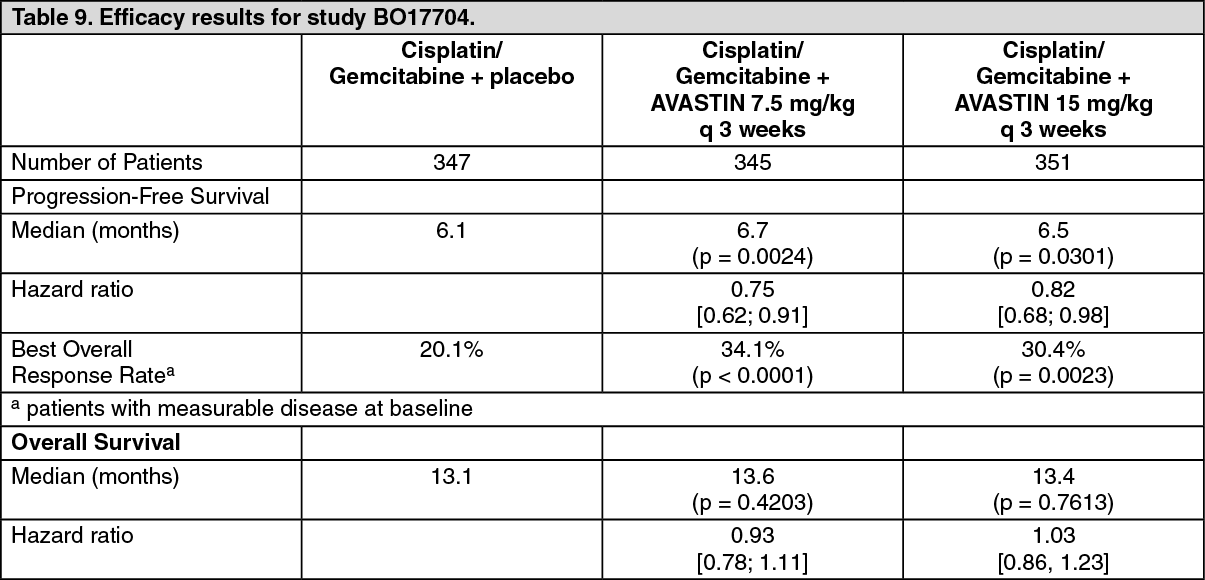
Click on icon to see table/diagram/imageBO17704: Study BO17704 was a randomised, double-blind phase III study of AVASTIN in addition to cisplatin and gemcitabine versus placebo, cisplatin and gemcitabine in patients with locally advanced, metastatic or recurrent non-squamous NSCLC, who had not received prior chemotherapy. The primary endpoint was progression-free survival, secondary endpoints for the study included the duration of overall survival.
Patients were randomised to platinum-based chemotherapy, cisplatin 80 mg/m2 i.v. infusion on day 1 and gemcitabine 1250 mg/m2 i.v. infusion on days 1 and 8 of every 3-week cycle for up to 6 cycles (CG) with placebo or CG with AVASTIN at a dose of 7.5 or 15 mg/kg IV infusion day 1 of every 3-week cycle. In the AVASTIN-containing arms, patients could receive AVASTIN as a single-agent every 3 weeks until disease progression or unacceptable toxicity. Study results show that 94% (277/296) of eligible patients went on to receive single agent AVASTIN at cycle 7. A high proportion of patients (approximately 62%) went on to receive a variety of non-protocol specified anti-cancer therapies, which may have impacted the analysis of overall survival.
The efficacy results are presented in Table 9. (See Table 9.)
 Click on icon to see table/diagram/image
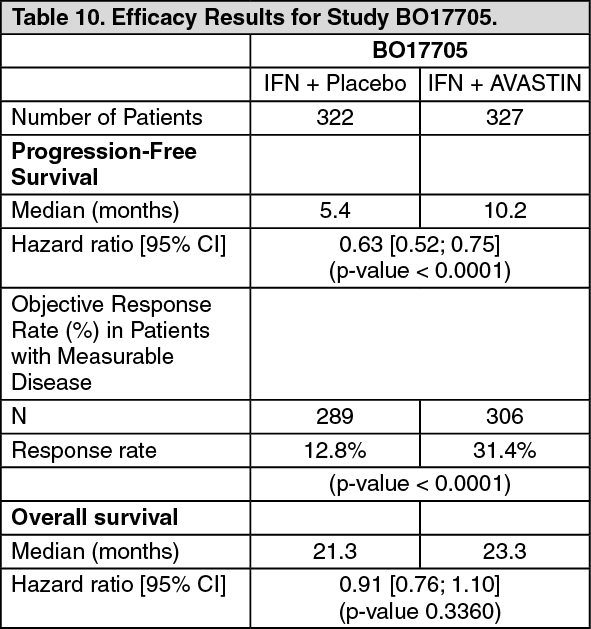
Click on icon to see table/diagram/imageAdvanced and/or metastatic Renal Cell Cancer (mRCC): BO17705: Study BO17705 was a multicenter randomised, double-blind phase III trial conducted to evaluate the efficacy and safety of AVASTIN in combination with interferon (IFN)-alfa-2a versus IFN-alfa-2a alone as first-line treatment in mRCC. The 649 randomised patients (641 treated) had clear cell mRCC, Karnofsky Performance Status (KPS) of ≥ 70%, no CNS metastases and adequate organ function. IFN-alfa-2a (x3/week at a recommended dose of 9 MIU) plus AVASTIN (10 mg/kg q2w) or placebo was given until disease progression. Patients were stratified according to country and Motzer score and the treatment arms were shown to be well balanced for the prognostic factors.
The primary endpoint was overall survival, with secondary endpoints for the study including progression-free survival. The addition of AVASTIN to IFN-alfa-2a significantly increased PFS and objective tumour response rate. These results have been confirmed through an independent radiological review. However, the increase in the primary endpoint of overall survival by 2 months was not significant (HR = 0.91). A high proportion of patients (approximately 63% IFN/placebo; 55% bevacizumab/IFN) received a variety of non-specified, post-protocol anti-cancer therapies, including antineoplastic agents, which may have impacted the analysis of overall survival.
The efficacy results are presented in Table 10. (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAn exploratory multivariate Cox regression model using backward selection indicated, that the following baseline prognostic factors were strongly associated with survival independent of treatment: gender, white blood cell count, platelets, body weight loss in the 6 months prior to study entry, number of metastatic sites, sum of longest diameter of target lesions, Motzer score. Adjustment for these baseline factors resulted in a treatment hazard ratio of 0.78 (95% CI [0.63; 0.96], p = 0.0219), indicating a 22% reduction in the risk of death for patients in the AVASTIN + IFN alfa-2a arm compared to IFN alfa-2a arm.
Ninety seven (97) patients in the IFN alfa-2a arm and 131 patients in the AVASTIN arm reduced the dose of IFN alfa-2a from 9 MIU to either 6 or 3 MIU, three times a week as pre-specified in the protocol. Dose-reduction of IFN alfa-2a did not appear to affect the efficacy of the combination of AVASTIN and IFN alfa-2a, based on PFS event free rates over time, as shown by a sub-group analysis. The 131 patients in the AVASTIN + IFN alfa-2a arm who reduced and maintained the IFN alfa-2a dose at 6 or 3 MIU during the study, exhibited at 6, 12 and 18 months, PFS event free rates of 73, 52 and 21% respectively, as compared to 61, 43 and 17% in the total population of patients receiving AVASTIN + IFN alfa-2a.
AVF2938: This was a randomised, double-blind, phase II clinical study investigating AVASTIN 10 mg/kg in a 2 weekly schedule with the same dose of AVASTIN in combination with 150 mg daily erlotinib, in patients with metastatic clear cell RCC. A total of 104 patients were randomised to treatment in this study, 53 to AVASTIN 10 mg/kg q2w plus placebo and 51 to AVASTIN 10 mg/kg q2w plus erlotinib 150 mg daily. The analysis of the primary endpoint showed no difference between the AVASTIN + PI arm and the AVASTIN + Erl arm (median PFS 8.5 versus 9.9 months). Seven patients in each arm had an objective response.
Glioblastoma: AVF3708g: The efficacy and safety of AVASTIN as treatment for patients with glioblastoma was studied in an open-label, multicenter, randomised, non-comparative study (study AVF3708g).
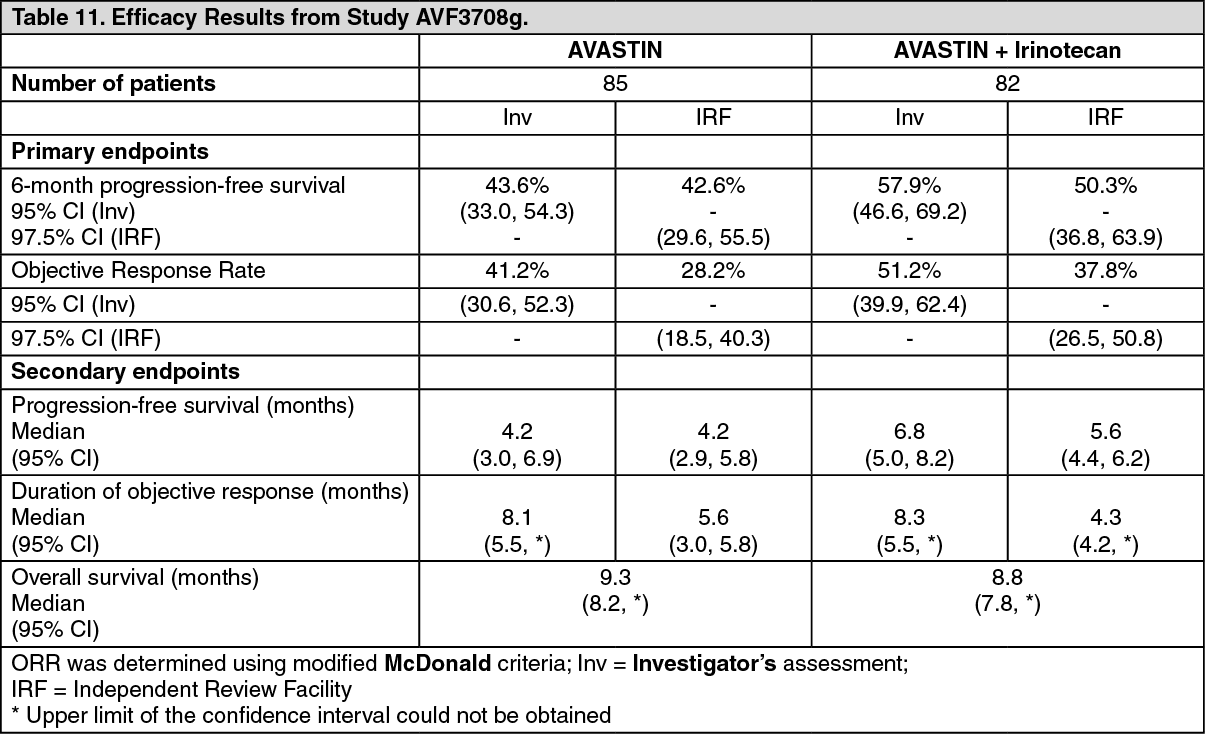
Glioblastoma patients in first or second relapse after prior radiotherapy (completed at least 8 weeks prior to receiving AVASTIN) and temozolomide, were randomised (1:1) to receive AVASTIN (10 mg/kg IV infusion every 2 weeks) or AVASTIN plus irinotecan (125 mg/m2 IV or 340 mg/m2 IV for patients on enzyme-inducing anti-epileptic drugs every 2 weeks) until disease progression or until unacceptable toxicity. The primary endpoints of the study were 6-month progression-free survival (PFS) and objective response rate (ORR) as assessed by an independent review facility (IRF). Other outcome measures were duration of PFS, duration of response and overall survival.
Results of the study are summarised in Table 11. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn study AVF3708g, six-month PFS based on IRF assessments was significantly higher (p < 0.0001) compared with historical controls for both treatment arms: 42.6% in the AVASTIN arm and 50.3% in the AVASTIN plus irinotecan arm (investigator assessment: 43.6% in the AVASTIN arm and 57.9% in the AVASTIN plus irinotecan arm). Objective response rates were also significantly higher (p < 0.0001) compared with historical controls for both treatment arms: 28.2% in the AVASTIN arm and 37.8% in the AVASTIN plus irinotecan arm (investigator assessment: 41.2% in the AVASTIN arm and 51.2% in the AVASTIN plus irinotecan arm).
The majority of patients who were receiving steroids at baseline, including responders and non-responders, were able to reduce their steroid utilisation over time while receiving AVASTIN treatment. The majority of patients experiencing an objective response or prolonged PFS (at week 24) were able to maintain or improve their neurocognitive functions while on study treatment compared to baseline. The majority of patients that remained in the study were progression-free at 24 weeks, had a Karnofsky performance status (KPS) that remained stable.
Epithelial Ovarian, Fallopian Tube and Primary Peritoneal Cancer: Front-line Ovarian Cancer: The safety and efficacy of AVASTIN in the front-line treatment of patients with epithelial ovarian, fallopian tube or primary peritoneal cancer were studied in two phase III trials (GOG-0218 and BO17707) that compared the effect of the addition of AVASTIN to carboplatin and paclitaxel compared to the chemotherapy regimen alone.
GOG-0218: The GOG-0218 study was a phase III multicenter, randomised, double-blind, placebo-controlled, three arm study evaluating the effect of adding AVASTIN to an approved chemotherapy regimen (carboplatin and paclitaxel) in patients with optimally or sub-optimally debulked Stage III or Stage IV epithelial ovarian, fallopian tube or primary peritoneal cancer.
A total of 1873 patients were randomised in equal proportions to the following three arms: CPP arm: Placebo in combination with carboplatin (AUC 6) and paclitaxel (175 mg/m2) for 6 cycles followed by placebo alone, for a total of up to 15 months of therapy;
CPB15 arm: Five cycles of AVASTIN (15 mg/kg q3w) in combination with carboplatin (AUC 6) and paclitaxel (175 mg/m2) for 6 cycles (AVASTIN commenced at cycle 2 of chemotherapy) followed by placebo alone, for a total of up to 15 months of therapy;
CPB15+ arm: Five cycles of AVASTIN (15 mg/kg q3w) in combination with carboplatin (AUC 6) and paclitaxel (175 mg/m2) for 6 cycles (AVASTIN commenced at cycle 2 of chemotherapy) followed by continued use of AVASTIN (15 mg/kg q3w) as single agent for a total of up to 15 months of therapy.
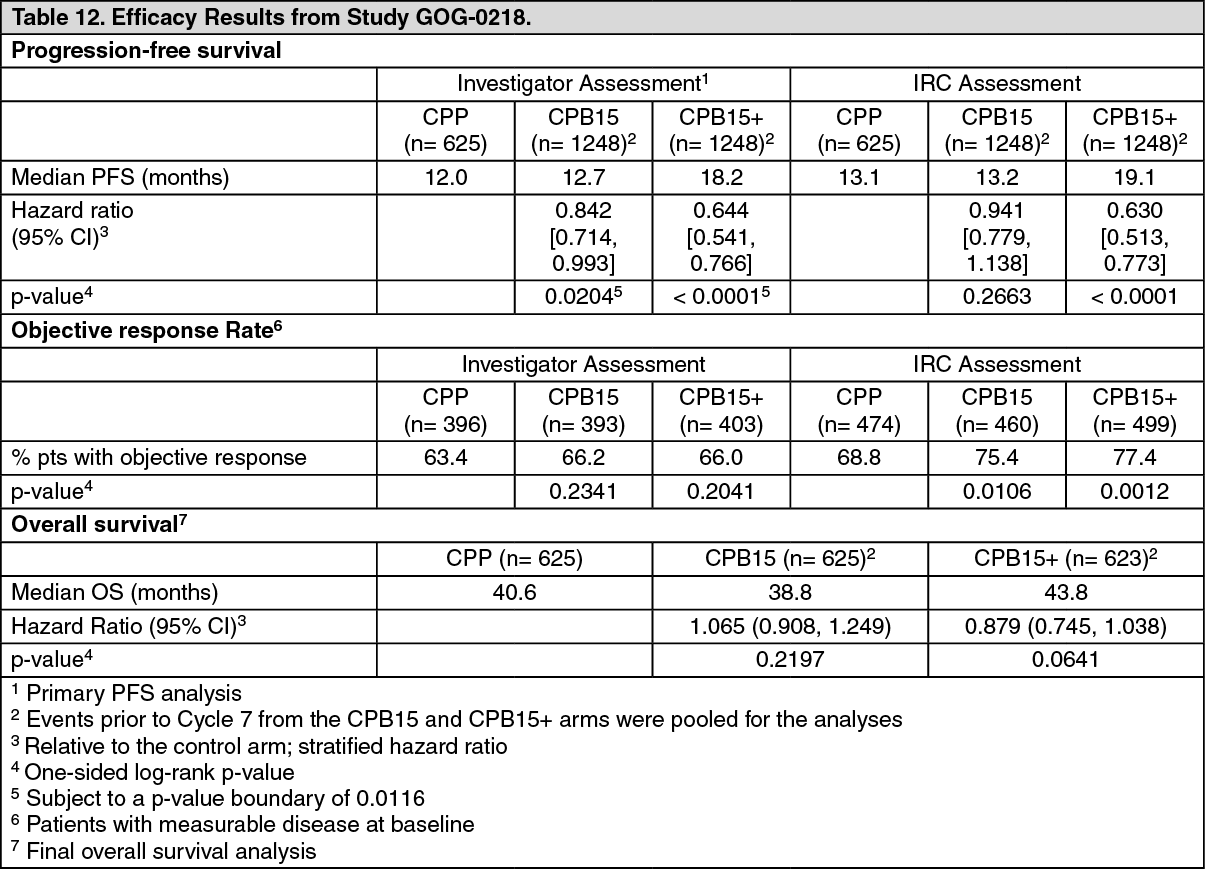
The primary endpoint was Progression-Free Survival (PFS) based on investigator's assessment of radiological scans. In addition, an independent review of the primary endpoint was also conducted.
The results of this study are summarised in Table 12. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe trial met its primary objective of PFS improvement. Compared to patients treated with chemotherapy (carboplatin and paclitaxel) alone, patients who received front-line AVASTIN at a dose of 15 mg/kg q3w in combination with chemotherapy and continued to receive AVASTIN alone, had a clinically meaningful and statistically significant improvement in PFS.
Although there was an improvement in PFS for patients who received front-line AVASTIN in combination with chemotherapy and did not continue to receive AVASTIN alone, the improvement was neither clinically meaningful nor statistically significant compared to patients who received chemotherapy alone.
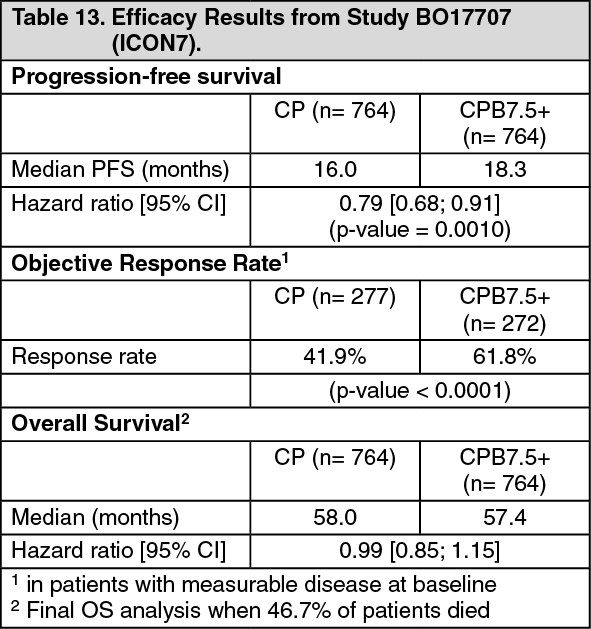
BO17707 (ICON7): BO17707 was a Phase III, two arm, multicenter, randomised, controlled, open-label study comparing the effects of adding bevacizumab to carboplatin plus paclitaxel in patients with FIGO Stage I or IIA (Grade 3 or clear cell histology only), or FIGO Stage IIB - IV (all grades and all histological types) epithelial ovarian, fallopian tube or primary peritoneal cancer following surgery, and in whom no further surgery was planned before progression. A total of 1528 patients were randomised in equal proportions to the following two arms: CP arm: Carboplatin (AUC 6) and paclitaxel (175 mg/m2) for 6 cycles;
CPB7.5+ arm: Carboplatin (AUC 6) and paclitaxel (175 mg/m2) for 6 cycles plus AVASTIN (7.5 mg/kg q3w) for up to 18 cycles.
The primary endpoint was Progression-Free Survival (PFS) as assessed by the investigator.
The results of this study are summarised in Table 13. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe trial met its primary objective of PFS improvement. Compared to patients treated with chemotherapy (carboplatin and paclitaxel) alone, patients who received AVASTIN at a dose of 7.5 mg/kg q3w in combination with chemotherapy and continued to receive AVASTIN for up to 18 cycles had a statistically significant improvement in PFS.
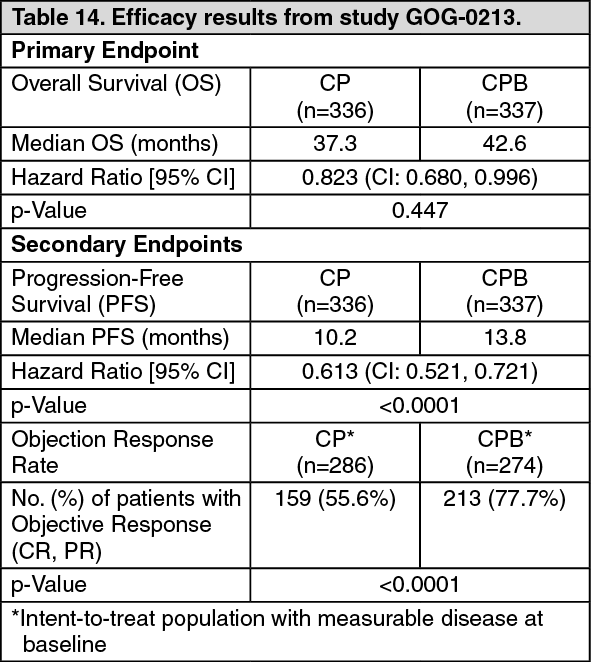
Recurrent Ovarian Cancer: GOG-0213: GOG-0213 was a phase III randomized controlled trial studying the safety and efficacy of Avastin in the treatment of patients with platinum-sensitive, recurrent epithelial ovarian, fallopian tube or primary peritoneal cancer, who have not received prior chemotherapy in the recurrent setting. There was no exclusion criterion for prior anti-angiogenic therapy. The study evaluated the effect of adding AVASTIN to carboplatin+paclitaxel and continuing Avastin as a single agent compared to carboplatin+paclitaxel alone.
A total of 673 patients were randomized in equal proportions to the following two treatment arms: CP arm: Carboplatin (AUC5) and paclitaxel (175 mg/m2 IV over 3 hours) every 3 weeks for 6 and up to 8 cycles;
CPB arm: Carboplatin (AUC5) and paclitaxel (175 mg/m2 IV over 3 hours) and concurrent AVASTIN (15 mg/kg) every 3 weeks for 6 and up to 8 cycles followed by AVASTIN (15 mg/kg every 3 weeks) alone until disease progression or unacceptable toxicity.
The primary efficacy endpoint was overall survival (OS). The main secondary efficacy endpoint was progression-free survival (PFS). Objective response rates (ORR) were also examined. Results are presented in Table 14. (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment with AVASTIN at 15 mg/kg every 3 weeks in combination with chemotherapy (carboplatin and paclitaxel) for 6 and up to 8 cycles then followed by AVASTIN as a single agent resulted in a clinically meaningful and statistically significant improvement in OS compared to treatment with carboplatin and paclitaxel alone.
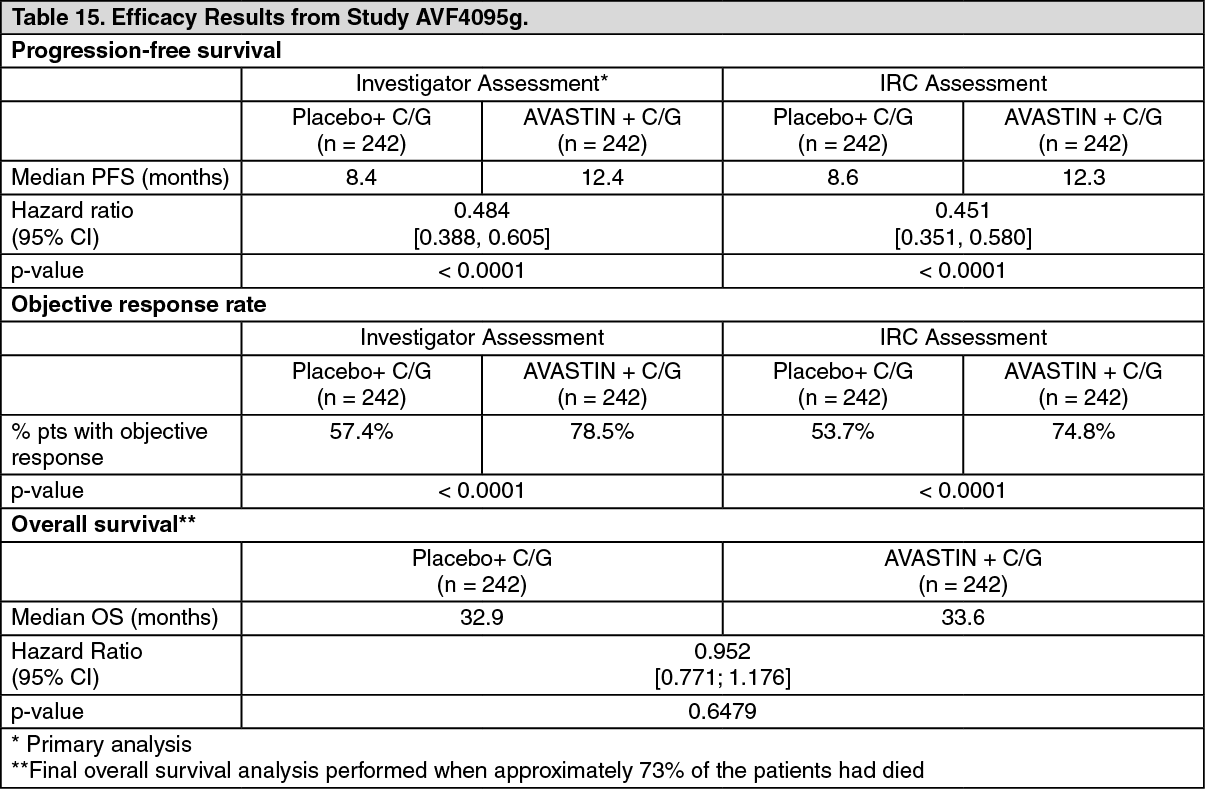
AVF4095g: The safety and efficacy of AVASTIN in the treatment of patients with platinum-sensitive, recurrent epithelial ovarian, fallopian tube or primary peritoneal cancer, who have not received prior chemotherapy in the recurrent setting or prior AVASTIN treatment, was studied in a phase III trial randomised, double-blind, placebo-controlled trial (AVF4095g). The study compared the effect of adding AVASTIN to carboplatin and gemcitabine chemotherapy and continuing AVASTIN as a single agent to progression to carboplatin and gemcitabine alone.
A total of 484 patients with measurable disease were randomised in equal portions to either: Carboplatin (AUC4, Day 1) and gemcitabine (1000 mg/m2 on Days 1 and 8) and concurrent placebo every 3 weeks for 6 and up to 10 cycles followed by placebo alone until disease progression or unacceptable toxicity.
Carboplatin (AUC4, Day 1) and gemcitabine (1000 mg/m2 on Days 1 and 8) and concurrent AVASTIN (15 mg/kg Day 1) every 3 weeks for 6 and up to 10 cycles followed by AVASTIN (15 mg/kg every 3 weeks) alone until disease progression or unacceptable toxicity.
The primary endpoint was progression-free survival based on investigator assessment using RECIST criteria. Additional endpoints included objective response, duration of response, safety and overall survival. An independent review of the primary endpoint was also conducted.
The results of this study are summarised in Table 15. (See Table 15.)
 Click on icon to see table/diagram/image
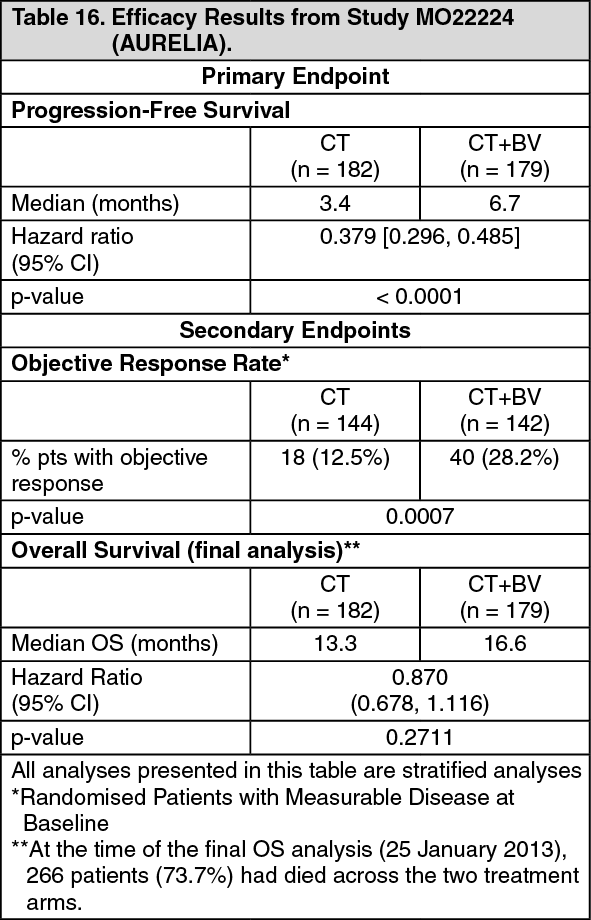
Click on icon to see table/diagram/imageMO22224 (AURELIA): Study MO22224 evaluated the efficacy and safety of AVASTIN in combination with chemotherapy for platinum-resistant recurrent ovarian cancer. This study was designed as an open-label, randomised, two-arm phase III evaluation of AVASTIN plus chemotherapy (CT+BV) versus chemotherapy alone (CT). A total of 361 patients were enrolled into this study and administered either chemotherapy (paclitaxel, topotecan, or PLD) alone or in combination with AVASTIN: CT Arm (chemotherapy alone): Paclitaxel 80 mg/m2 as a 1-hour IV infusion on Days 1, 8, 15, and 22 every 4 weeks.
Topotecan 4 mg/m2 as a 30 minute IV infusion on Days 1, 8, and 15 every 4 weeks. Alternatively, a 1.25 mg/m2 dose could be administered over 30 minutes on Days 1-5 every 3 weeks.
PLD 40 mg/m2 as a 1 mg/min IV infusion on Day 1 only every 4 weeks. After Cycle 1, the drug could be delivered as a 1 hour infusion.
CT+BV Arm (chemotherapy plus AVASTIN): The chosen chemotherapy was combined with AVASTIN 10 mg/kg IV every 2 weeks (or AVASTIN 15 mg/kg every 3 weeks if used in combination with topotecan 1.25 mg/m2 on Days 1-5 on a every 3 weeks schedule).
Eligible patients had ovarian cancer that progressed within 6 months of previous platinum therapy. If a patient had been previously included in a blinded trial with an anti-angiogenic agent, the patient was enrolled in the same stratum as those patients who were known to have previously received an anti-angiogenic agent.
The primary endpoint was progression-free survival, with secondary endpoints including objective response rate and overall survival. Results are presented in Table 16. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCervical Cancer: GOG-0240: The efficacy and safety of AVASTIN in combination with chemotherapy (paclitaxel and cisplatin or paclitaxel and topotecan) as a treatment for patients with persistent, recurrent, or metastatic carcinoma of the cervix was evaluated in study GOG-0240, a randomised, four-arm, multicentre phase III trial.
A total of 452 patients were randomised to receive either: Paclitaxel 135 mg/m2 IV over 24 hours on Day 1 and cisplatin 50 mg/m2 IV on Day 2, every 3 weeks (q3w); or paclitaxel 175 mg/m2 IV over 3 hours on Day 1 and cisplatin 50 mg/m2 IV on Day 2 (q3w); or paclitaxel 175 mg/m2 IV over 3 hours on Day 1 and cisplatin 50 mg/m2 IV on Day 1 (q3w).
Paclitaxel 135 mg/m2 IV over 24 hours on Day 1 and cisplatin 50 mg/m2 IV on Day 2 plus AVASTIN 15 mg/kg IV on Day 2 (q3w); paclitaxel 175 mg/m2 IV over 3 hours on Day 1 and cisplatin 50 mg/m2 IV on Day 2 plus AVASTIN 15 mg/kg IV on Day 2 (q3w); or paclitaxel 175 mg/m2 IV over 3 hours on Day 1 and cisplatin 50 mg/m2 IV on Day 1 and AVASTIN 15 mg/kg IV on day 1 (q3w).
Paclitaxel 175 mg/m2 over 3 hours on Day 1 and topotecan 0.75 mg/m2 over 30 minutes on Days 1-3 (q3w).
Paclitaxel 175 mg/m2 over 3 hours on Day 1 and topotecan 0.75 mg/m2 over 30 minutes on Days 1-3 plus AVASTIN 15 mg/kg IV on Day 1 (q3w).
Eligible patients had persistent, recurrent, or metastatic squamous cell carcinoma, adenosquamous carcinoma, or adenocarcinoma of the cervix which was not amenable to curative treatment with surgery and/or radiation therapy.
The primary efficacy endpoint was overall survival (OS). Secondary efficacy endpoints included progression-free survival (PFS) and objective response rate (ORR). Results are presented in Table 17. (See Table 17.)
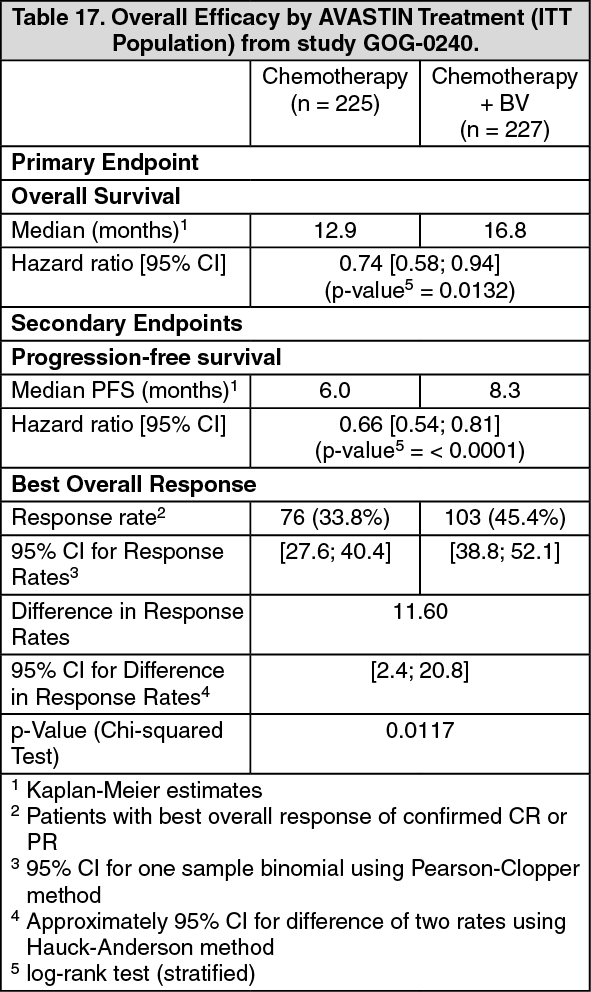 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmunogenicity: No robust assessment of anti-drug antibodies has been done in Avastin clinical trials.
For MVASI, see Clinical/Efficacy Studies: Efficacy data for MVASI and Immunogenicity as previously mentioned.
Pharmacokinetics: The pharmacokinetics of MVASI is similar to AVASTIN.
The pharmacokinetics of bevacizumab were characterised in patients with various types of solid tumours. The doses tested were 0.1-10 mg/kg weekly in phase I; 3-20 mg/kg every two weeks (q2w) or every three weeks (q3w) in phase II; 5 mg/kg (q2w) or 15 mg/kg q3w in phase III. In all clinical trials, bevacizumab was administered as an IV infusion.
As observed with other antibodies, the pharmacokinetics of bevacizumab are well described by a two-compartment model. Overall, in all clinical trials, bevacizumab disposition was characterised by a low clearance, a limited volume of the central compartment (Vc), and a long elimination half-life. This enables target therapeutic bevacizumab serum levels to be maintained with a range of administration schedules (such as one administration every 2 or 3 weeks).
In the population pharmacokinetics analysis there was no significant difference in the pharmacokinetics of bevacizumab in relation to age (no correlation between bevacizumab clearance and patient age [the median age was 59 year with 5th and 95th percentiles of 37 and 76 year]).
Low albumin and high tumour burden are generally indicative of disease severity. Bevacizumab clearance was approximately 30% faster in patients with low levels of serum albumin and 7% faster in subjects with higher tumour burden when compared with a typical patient with median values of albumin and tumour burden.
Absorption: No information available.
Distribution: The typical value for central volume (Vc) was 2.73 L and 3.28 L for female and male subjects respectively, which is in the range that has been described for IgGs and other monoclonal antibodies. The typical value for peripheral volume (Vp) was 1.69 L and 2.35 L for female and male patients respectively, when bevacizumab is coadministered with anti-neoplastic agents. After correcting for body weight, male subjects had a larger Vc (+20%) than females.
Metabolism: Assessment of bevacizumab metabolism in rabbits following a single i.v. dose of 125 I-bevacizumab indicated that its metabolic profile was similar to that expected for a native IgG molecule which does not bind VEGF. The metabolism and elimination of bevacizumab is similar to endogenous IgG i.e. primarily via proteolytic catabolism throughout the body, including endothelial cells, and does not rely primarily on elimination through the kidneys and liver. Binding of the IgG to the FcRn receptor result in protection from cellular metabolism and the long terminal half-life.
Elimination: The pharmacokinetics of bevacizumab are linear at doses ranging from 1.5 to 10 mg/kg/wk. The value for clearance is, on average, equal to 0.188 and 0.220 L/day for female and male patients respectively. After correcting for body weight, male patients had a higher bevacizumab clearance (+17%) than females. According to the two-compartmental model, the elimination half-life is 18 days for a typical female patient and 20 days for a typical male patient.
Pharmacokinetics in Special Populations: The population pharmacokinetics were analysed to evaluate the effects of demographic characteristics. The results showed no significant difference in the pharmacokinetics of bevacizumab in relation to age.
Pediatric population: The pharmacokinetics of bevacizumab have been studied in a limited number of paediatric patients. The resulting pharmacokinetic data suggest that the volume of distribution and clearance of bevacizumab were comparable to that in adults with solid tumours.
Renal impairment: No studies have been conducted to investigate the pharmacokinetics of bevacizumab in renally impaired patients since the kidneys are not a major organ for bevacizumab metabolism or excretion.
Hepatic impairment: No studies have been conducted to investigate the pharmacokinetics of bevacizumab in patients with hepatic impairment since the liver is not a major organ for bevacizumab metabolism or excretion.
Toxicology: Nonclinical Safety: Carcinogenicity: Studies have not been performed to evaluate the carcinogenic potential of bevacizumab.
Genotoxicity: Studies have not been performed to evaluate the mutagenic potential of bevacizumab.
Impairment of Fertility: No specific studies in animals have been performed to evaluate the effect of bevacizumab on fertility. No adverse effect on male reproductive organs was observed in repeat dose toxicity studies in cynomolgus monkeys. Inhibition of ovarian function was characterised by decreases in ovarian and/or uterine weight and the number of corpora lutea, a reduction in endometrial proliferation and an inhibition of follicular maturation in cynomolgus monkeys treated with bevacizumab for 13 or 26 weeks. The doses associated with this effect were ≥4 times the human therapeutic dose or ≥2-fold above the expected human exposure based on average serum concentrations in female monkeys. In rabbits, administration of 50 mg/kg of bevacizumab resulted in a significant decrease in ovarian weight and number of corpora lutea. The results in both monkeys and rabbits were reversible upon cessation of treatment. The inhibition of angiogenesis following administration of bevacizumab is likely to result in an adverse effect on female fertility.
Reproductive Toxicity: Bevacizumab has been shown to be embryotoxic and teratogenic when administered to rabbits. Observed effects included decreases in maternal and foetal body weights, an increased number of foetal resorptions and an increased incidence of specific gross and skeletal foetal alterations. Adverse foetal outcomes were observed at all tested doses of 10-100 mg/kg. Information on foetal malformations observed in the post-marketing setting are provided in Use in Pregnancy & Lactation and Postmarketing Experience under Adverse Reactions.
Other: Physeal development: In studies of up to 26 weeks duration in cynomolgus monkeys, bevacizumab was associated with physeal dysplasia. Physeal dysplasia was characterised primarily by thickened growth plate cartilage, subchondral bony plate formation and inhibition of vascular invasion of the growth plate. This effect occurred at doses ≥ 0.8 times the human therapeutic dose and exposure levels slightly below the expected human clinical exposure, based on average serum concentrations. It should be noted, however, that physeal dysplasia occurred only in actively growing animals with open growth plates.
Wound healing: In rabbits, the effects of bevacizumab on circular wound healing were studied. Wound re-epithelialisation was delayed in rabbits following five doses of bevacizumab, ranging from 2-50 mg/kg, over a 2-week period. A trend toward a dose-dependent relationship was observed. The magnitude of effect on wound healing was similar to that observed with corticosteroid administration. Upon treatment cessation with either 2 or 10 mg/kg bevacizumab, the wounds closed completely. The lower dose of 2 mg/kg was approximately equivalent to the proposed clinical dose. A more sensitive linear wound healing model was also studied in rabbits. Three doses of bevacizumab ranging from 0.5-2 mg/kg dose-dependently and significantly decreased the tensile strength of the wounds, consistently with delayed wound healing. The low dose of 0.5 mg/kg was 5-fold below the proposed clinical dose.
As effects on wound healing were observed in rabbits at doses below the proposed clinical dose, the capacity for bevacizumab to adversely impact wound healing in human should be considered.
In cynomolgus monkeys, the effects of bevacizumab on the healing of a linear incision were highly variable and no dose-response relationship was evident.
Renal function: In normal cynomolgus monkeys, bevacizumab had no measurable effect on renal function treated once or twice weekly for up to 26 weeks, and did not accumulate in the kidney of rabbits following two doses up to 100 mg/kg (approximately 80-folds the proposed clinical dose).
Investigative toxicity studies in rabbits, using the models of renal dysfunction, showed that bevacizumab did not exacerbate renal glomerular injury induced by bovine serum albumin or renal tubular damage induced by cisplatin.
Albumin: In male cynomolgus monkeys, bevacizumab administered at doses of 10 mg/kg twice weekly or 50 mg/kg once weekly for 26 weeks was associated with a statistically significant decrease in albumin and albumin to globulin ratio and increase in globulin. These effects were reversible upon cessation of exposure. As the parameters remained within the normal reference range of values for these endpoints, these changes were not considered as clinically significant.
Hypertension: At doses up to 50 mg/kg twice weekly in cynomolgus monkeys, bevacizumab showed no effects on blood pressure.
Haemostasis: Non-clinical toxicology studies of up to 26 weeks duration in cynomolgus monkeys did not find changes in haematology or coagulation parameters including platelet counts, prothrombin and activated partial thromboplastin time. A model of haemostasis in rabbits, used to investigate the effect of bevacizumab on thrombus formation, did not show alteration in the rate of clot formation or any other haematological parameters compared to treatment with bevacizumab vehicle.