


 Sign Out
Sign Out

The most serious adverse events were: Gastrointestinal perforations (see General under Precautions);
Haemorrhage including pulmonary haemorrhage/haemoptysis, which is more common in NSCLC patients (see General under Precautions);
Arterial thromboembolism (see General under Precautions);
Analyses of the clinical safety data suggest that the occurrence of hypertension and proteinuria with bevacizumab therapy are likely to be dose-dependent.
The most frequently observed adverse drug reactions across clinical trials in patients receiving bevacizumab were hypertension, fatigue or asthenia, diarrhoea and abdominal pain.
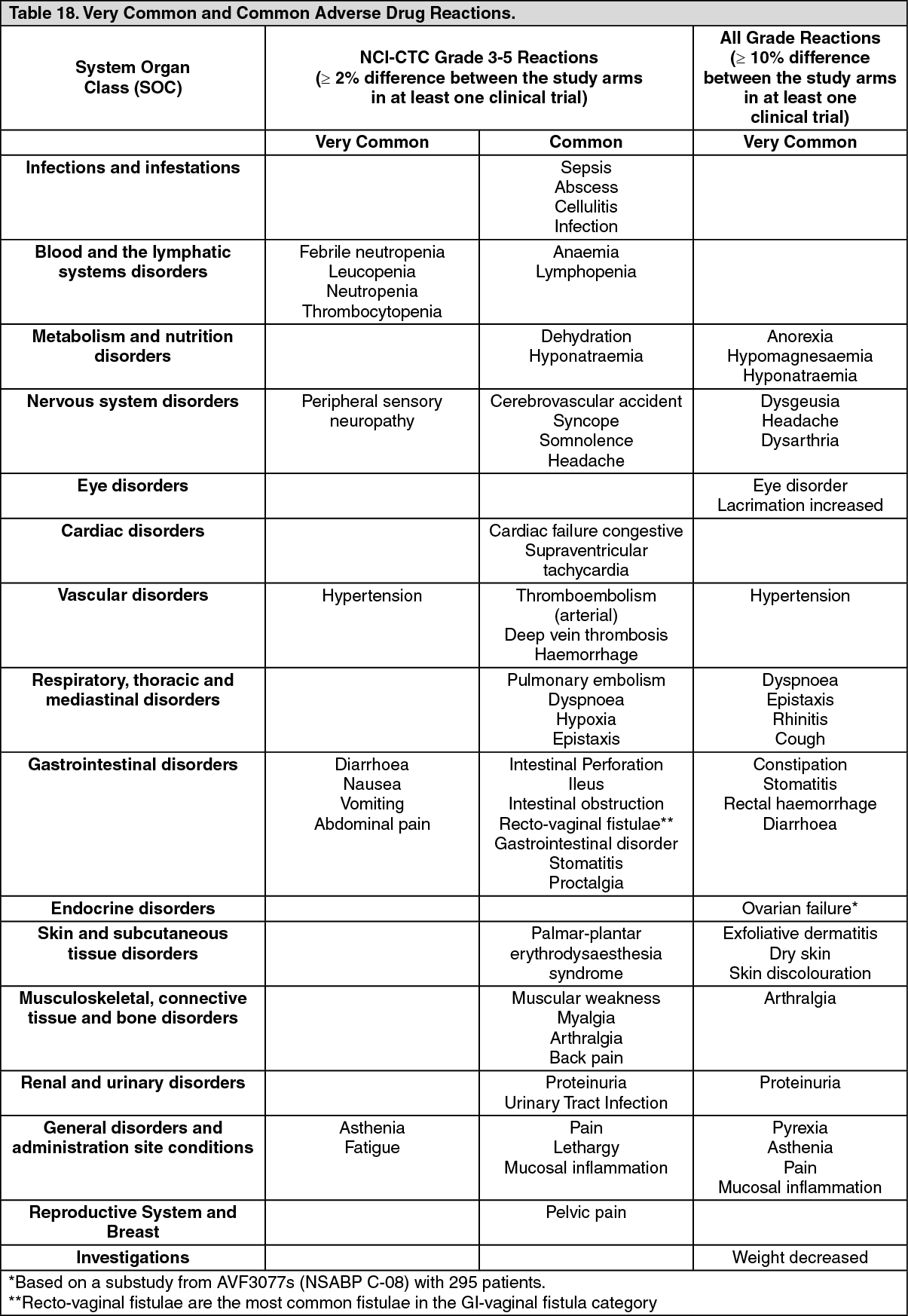
Tabulated summary of adverse drug reactions from clinical trials: Table 18 lists adverse drug reactions associated with the use of bevacizumab in combination with different chemotherapy regimens in multiple indications, by MedDRA system organ class. The corresponding frequency category for each adverse drug reaction is based on the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). These reactions had occurred either with at least a 2% difference compared to the control arm (NCI-CTC [common toxicity criteria] Grade 3-5 reactions) or with at least a 10% difference compared to the control arm (NCI-CTC Grade 1-5 reactions), in at least one of the major clinical trials. Adverse drug reactions are added to the appropriate category in the table as follows according to the highest incidence seen in any of the major clinical trials. Within each frequency grouping adverse drug reactions are presented in order of decreasing seriousness. Some of the adverse reactions are reactions commonly seen with chemotherapy, however, bevacizumab may exacerbate these reactions when combined with chemotherapeutic agents. Examples include palmar-plantar erythrodysaesthesia syndrome with pegylated liposomal doxorubicin or capecitabine, peripheral sensory neuropathy with paclitaxel or oxaliplatin, and nail disorders or alopecia with paclitaxel. (See Table 18.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse drug reactions from clinical trials: The following adverse drug reactions, reported using NCI-CTC for assessment of toxicity have been observed in patients treated with bevacizumab: Gastrointestinal perforation and Fistulae (see General under Precautions): Bevacizumab has been associated with serious cases of gastrointestinal perforation.
Gastrointestinal perforations have been reported in clinical trials with an incidence of less than 1% in patients with metastatic breast cancer or non-squamous non-small cell lung cancer, up to 2% in patients with metastatic renal cell cancer, or in patients with ovarian cancer receiving front-line treatment, and up to 2.7% (including gastrointestinal fistula and abscess) in patients with metastatic colorectal cancer. Cases of GI perforations have also been observed in patients with relapses glioblastoma.
From a clinical trial in patients with persistent, recurrent, or metastatic cervical cancer (study GOG-0240), GI perforations, (all grade) were reported in 3.2% of patients, all of whom had a history of prior pelvic radiation. The occurrence of those events varied in type and severity, ranging from free air seen on the plain abdominal X-ray, which resolved without treatment, to intestinal perforation with abdominal abscess and fatal outcome. In some cases underlying intra-abdominal inflammation was present, either from gastric ulcer disease, tumour necrosis, diverticulitis or chemotherapy-associated colitis. A casual association of intra-abdominal inflammatory process and gastrointestinal perforation to bevacizumab has not been established. Fatal outcome was reported in approximately a third of serious cases of gastrointestinal perforations, which represents between 0.2% - 1% of all bevacizumab treated patients.
In bevacizumab clinical trials, gastrointestinal fistulae (all grade) have been reported with an incidence of up to 2% in patients with metastatic colorectal cancer and ovarian cancer, but were also reported less commonly in patients with other types of cancer.
In a trial of patients with persistent, recurrent or metastatic cervical cancer, the incidence of GI-vaginal fistulae was 8.3% in bevacizumab-treated patients and 0.9% in control patients, all of whom had a history of prior pelvic radiation. Patients who develop GI-vaginal fistulae may also have bowel obstructions and require surgical intervention as well as diverting ostomies.
Non-GI Fistulae (see General under Precautions): Bevacizumab use has been associated with serious cases of fistulae including events resulting in death.
From a clinical trial in patients with persistent, recurrent, or metastatic cervical cancer (GOG-240), 1.8% of bevacizumab treated patients and 1.4% of control patients were reported to have had non-gastrointestinal vaginal, vesical, or female genital tract fistulae.
Uncommon (≥ 0.1% to < 1%) reports of other types of fistulae that involve areas of the body other than the gastrointestinal tract (e.g. bronchopleural, biliary fistulae) were observed across various indications.
Fistulae have also been reported in post-marketing experience.
Events were reported at various time points during treatment ranging from one week to greater than 1 year from initiation of bevacizumab, with most events occurring within the first 6 months of therapy.
Haemorrhage: In clinical trials across all indications the overall incidence of NCI-CTC Grade 3-5 bleeding events ranged from 0.4% to 6.9% in bevacizumab-treated patients, compared to 0 to 4.5% of patients in the chemotherapy control group. The haemorrhagic events that have been observed in bevacizumab clinical studies were predominantly tumour-associated haemorrhage (see as follows) and minor mucocutaneous haemorrhage (e.g. epistaxis).
Tumour-associated haemorrhage: Major or massive pulmonary haemorrhage/haemoptysis has been observed primarily in studies in patients with non-small cell lung cancer (NSCLC). Possible risk factors include squamous cell histology, treatment with antirheumatic/anti-inflammatory drugs, treatment with anticoagulants, prior radiotherapy, bevacizumab therapy, previous medical history of atherosclerosis, central tumour location and cavitation of tumours prior to or during therapy. The only variables that showed statistically significant correlations with bleeding were bevacizumab therapy and squamous cell histology. Patients with NSCLC of known squamous cell histology or mixed cell type with predominant squamous cell histology were excluded from subsequent studies, while patients with unknown tumour histology were included.
In patients with NSCLC excluding predominant squamous histology, all grade events were seen with a frequency of up to 9.3% when treated with bevacizumab plus chemotherapy compared with 5% in the patients treated with chemotherapy alone. Grade 3-5 events have been observed in up to 2.3% of patients treated with bevacizumab plus chemotherapy as compared with < 1% with chemotherapy alone. Major or massive pulmonary haemorrhage/haemoptysis can occur suddenly and up to two thirds of the serious pulmonary haemorrhages resulted in a fatal outcome (see General under Precautions).
Gastrointestinal haemorrhages, including rectal bleeding and melaena have been reported in colorectal patients, and have been assessed as tumour-associated haemorrhages.
Tumour-associated haemorrhages were also seen rarely in other tumour types and locations and included cases of central nervous system (CNS) bleeding in patients with CNS metastases and in patients with glioblastoma. The incidence of CNS bleeding in patients with untreated CNS metastases receiving bevacizumab has not been prospectively evaluated in randomised in clinical studies. In an exploratory retrospective analysis of data from 13 completed randomised trials in patients with various tumour types, 3 patients out of 91 (3.3%) with brain metastases experienced CNS bleeding (all Grade 4) when treated with bevacizumab, compared to 1 case (Grade 5) out of 96 patients (1%) that were not exposed to bevacizumab. In two subsequent studies in patients with treated brain metastases (which included around 800 patients), one case of Grade 2 CNS haemorrhage was reported. Intracranial haemorrhage can occur in patients with relapsed glioblastoma. In study AVF3708g, CNS haemorrhage was reported in 2.4% (2/84) of patients in the bevacizumab alone arm (Grade 1); and in 3.8% (3/79) of patients treated with bevacizumab and irinotecan (Grades 1, 2 and 4).
Across all bevacizumab clinical trials, mucocutaneous haemorrhage were seen in up to 50% of patients treated with bevacizumab. These were most commonly NCI-CTC Grade 1 epistaxis that lasted less than 5 minutes, resolved without medical intervention and did not require any change in the bevacizumab treatment regimen. Clinical safety data suggest that the incidence of minor mucocutaneous haemorrhage (e.g. epistaxis) may be dose dependent. There have also been less common events of minor mucocutaneous haemorrhage in other locations, such as gingival bleeding or vaginal bleeding.
Hypertension (see General under Precautions): An increased incidence of hypertension (all grades) of up to 42.1% has been observed in patients treated with bevacizumab compared with up to 14% in all the comparator arm. In clinical trials across all indications the overall incidence of NCI-CTC Grade 3 and 4 hypertension in patients receiving bevacizumab ranged from 0.4% to 17.9%. Grade 4 hypertension (hypertensive crisis) occurred in up to 1.0% of patients treated with bevacizumab compared to up to 0.2% patients treated with the same chemotherapy alone. Hypertension was generally adequately controlled with oral anti-hypertensives such as angiotensin-converting enzyme inhibitors, diuretics and calcium-channel blockers. It rarely resulted in discontinuation of bevacizumab treatment or hospitalisation.
Very rare cases of hypertensive encephalopathy have been reported, some of which were fatal (see also General under Precautions). The risk of bevacizumab associated hypertension did not correlate with the patients' baseline characteristics, underlying disease or concomitant therapy.
Posterior Reversible Encephalopathy Syndrome (see General under Precautions): Two confirmed cases (0.8%) of PRES have been reported in one clinical study. Symptoms usually resolve or improve within days, although some patients have experienced neurologic sequelae.
Thromboembolism: Arterial thromboembolism: An increased incidence of arterial thromboembolic events was observed in patients treated with bevacizumab across indications including cerebrovascular accidents, myocardial infarction, transient ischemic attacks, and other arterial thromboembolic events.
In clinical trials, the overall incidence ranged up to 5.90% in the bevacizumab containing arms compared up to 1.7% in the chemotherapy control arms. Fatal outcome was reported in 0.8% of patients receiving bevacizumab in combination with chemotherapy compared to 0.5% of patients receiving chemotherapy alone. Cerebrovascular accidents (including transient ischemic attacks) were reported in up to 2.7% of bevacizumab treated patients versus 0.5% of patients in the control group: myocardial infarction was reported in 1.4% of bevacizumab treated versus 0.7% of patients in the observed control group.
In one clinical trial, AVF2192g, patients with metastatic colorectal cancer who were not candidates for treatment with irinotecan were included. In this trial arterial thromboembolic events were observed in 11% (11/100) of bevacizumab patients compared to 5.8% (6/104) in the chemotherapy control group. In an uncontrolled clinical trial, AVF3708g, in patients with relapsed glioblastoma, arterial thromboembolic events were observed in 6.3% (5/79) of patients who received bevacizumab in combination with irinotecan compared to 4.8% (4/84) of patients who received bevacizumab alone.
Venous thromboembolism (see General under Precautions): In clinical trials across indications, the overall incidence of venous thromboembolic events ranged from 2.8% to 17.3% in the bevacizumab containing arms compared to 3.2% to 15.6% in the chemotherapy control arms. Venous thromboembolic events include deep venous thrombosis and pulmonary embolism.
Grade 3-5 venous thromboembolic events have been reported in up to 7.8% of patients treated with chemotherapy plus bevacizumab compared with up to 4.9% in patients with chemotherapy alone. Patients who have experienced a venous thromboembolic event may be at higher risk for a recurrence if they receive bevacizumab in combination with chemotherapy versus chemotherapy alone.
From a clinical trial in patients with persistent, recurrent, or metastatic cervical cancer (study GOG-0240), grade 3-5 venous thromboembolic events have been reported in up to 10.6% of patients treated with chemotherapy and bevacizumab compared with up to 5.4% in patients with chemotherapy alone.
Congestive heart failure: In clinical trials with bevacizumab, congestive heart failure (CHF) was observed in all cancer indications studied to date, but occurred predominantly in patients with metastatic breast cancer. In phase III studies (AVF2119g and E2100) in patients with metastatic breast cancer an increase of CHF Grade 3 or more with bevacizumab was seen. CHF was reported in up to 3.5% of patients treated with bevacizumab compared with up to 0.9% in the control arms. Most of these patients who developed CHF during mBC trials showed improved symptoms and/or left ventricular function following appropriate medical therapy.
In most clinical trials of bevacizumab, patients with pre-existing CHF of NYHA II - IV were excluded, therefore, no information is available on the risk of CHF in this population.
Prior anthracyclines exposure and/or prior radiation to the chest wall may be possible risk factors for the development of CHF (see General under Precautions). An increased incidence of CHF has been observed in a clinical trial of patients with diffuse large B-cell lymphoma when receiving bevacizumab with a cumulative doxorubicin dose greater than 300 mg/m2. This phase III clinical trial compared rituximab/cyclophosphamide/doxorubicin/vincristine/prednisone (R-CHOP) plus bevacizumab to R-CHOP without bevacizumab. While the incidence of CHF was, in both arms, above that previously observed for doxorubicin therapy, the rate was higher in the R-CHOP plus bevacizumab arm.
Wound healing (see General under Precautions): As bevacizumab may adversely impact wound healing, patients who had major surgery within the last 28 days prior to starting bevacizumab treatment were excluded from participation in phase III trials.
Across mCRC clinical trials there was no increased risk of post-operative bleeding or wound healing complications observed in patients who underwent major surgery between 28-60 days prior to starting bevacizumab therapy. An increased incidence of post-operative bleeding or wound healing complications occurring within 60 days of major surgery was observed if the patient was being treated with bevacizumab at the time of surgery. The incidence varied between 10% (4/40) and 20% (3/15).
Cases of serious wound healing complications have been reported during bevacizumab use, some of which had a fatal outcome (see General under Precautions).
In locally recurrent and metastatic breast cancer trials, Grade 3-5 wound healing complications were observed in up to 1.1% of patients receiving bevacizumab compared with up to 0.9% of patients in the control arms.
In a study of patients with relapsed glioblastoma (study AVF3708g), the incidence of post-operative wound healing complications (including craniotomy site wound dehiscence and cerebrospinal fluid leak) was 3.6% in patients treated with single-agent bevacizumab and 1.3% in patients treated with bevacizumab plus irinotecan. In clinical trials of ovarian cancer, Grade 3-5 wound healing complications were observed in up to 1.2% of patients in the bevacizumab arm versus 0.1% in the control arm.
Proteinuria (see General under Precautions): In clinical trials, proteinuria has been reported within the range of 0.7% to 54.7% of patients receiving bevacizumab. Proteinuria ranged in severity from clinically asymptomatic, transient, trace proteinuria to nephrotic syndrome. Grade 3 proteinuria was reported in up to 8.1% of treated patients. Grade 4 proteinuria (nephrotic syndrome) was seen in up to 1.4% of treated patients.
Patients with a history of hypertension may be at increased risk for the development of proteinuria when treated with bevacizumab. There is evidence suggesting that Grade 1 proteinuria may be related to bevacizumab dose. Testing for proteinuria is recommended prior to start of bevacizumab therapy. In most clinical studies urine protein levels of ≥ 2g/24 hrs led to the holding of bevacizumab until recovery to < 2g/24 hrs.
Hypersensitivity, infusion reactions (see General under Precautions and Postmarketing Experience under Adverse Reactions): In some clinical trials anaphylactic and anaphylactoid-type reactions were reported more frequently in patients receiving bevacizumab in combination with chemotherapies than with chemotherapy alone. The incidence of these reactions in some clinical trials of bevacizumab is common (up to 5% in bevacizumab-treated patients).
Ovarian Failure/Fertility (see General under Precautions and Females and Males of Reproductive Potential under Use in Pregnancy & Lactation): The incidence of new cases of ovarian failure, defined as amenorrhea lasting 3 or more months, FSH level ≥ 30 mIU/mL and a negative serum β-HCG pregnancy test has been evaluated. New cases of ovarian failure were reported more frequently in patients receiving bevacizumab. After discontinuation of bevacizumab treatment, ovarian function recovered in majority of women. Long term effects of the treatment with bevacizumab on fertility are unknown.
Elderly patients: In randomised clinical trials, age > 65 years was associated with an increased risk of developing arterial thromboembolic events including cerebrovascular accidents, transient ischemic attacks and myocardial infarction as compared to those aged ≤ 65 years when treated with bevacizumab (see General under Precautions and Clinical Trials for AVASTIN: Thromboembolism as previously mentioned). Other reactions with a higher frequency seen in patients over 65 were grade 3-4 leucopenia, thrombocytopenia; and all Grade neutropenia, diarrhoea, nausea, headache and fatigue.
From a clinical trial in patients with metastatic colorectal cancer (study AVF2107), no increase in the incidence of other reactions, including gastrointestinal perforation, wound healing complications, congestive heart failure and haemorrhage, was observed in elderly patients (> 65 years) receiving bevacizumab as compared to those aged ≤ 65 years treated with bevacizumab.
Laboratory Abnormalities: Decreased neutrophil count, decreased white blood cell count and presence of urine protein may be associated with bevacizumab treatment.
Across clinical trials, the following Grade 3 and 4 laboratory abnormalities were seen with an increased (≥ 2%) incidence in patients treated with bevacizumab compared to those in the control groups: hyperglycaemia, decreased haemoglobin, hypokalaemia, hyponatraemia, decreased white blood cell count, increased PT (prothrombin time), normalised ratio. Clinical trials have shown that transient increases in serum creatinine (ranging between 1.5-1.9 times baseline level), both with and without proteinuria, are associated with the use of bevacizumab. The observed increase in serum creatinine was not associated with a higher incidence of clinical manifestations of renal impairment in patients treated with bevacizumab.
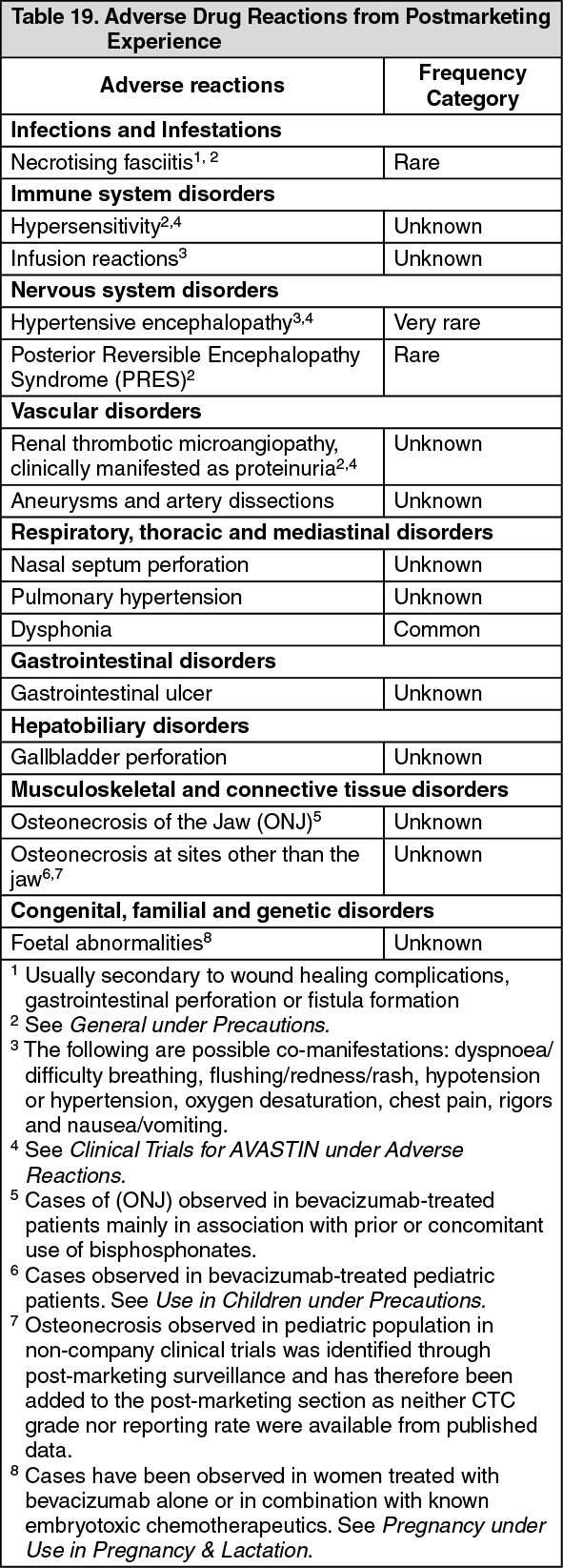
Postmarketing Experience: The following adverse drug reactions have been identified from postmarketing experience with bevacizumab (Table 19) based on spontaneous case reports and literature cases. Adverse drug reactions are listed according to system organ classes in MedDRA and the corresponding frequency category estimation for each adverse drug reaction is based on the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). (See Table 19.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse drug reactions from postmarketing experience: Eye disorders (reported from unapproved intravitreal use): Infectious endophthalmitis (frequency not known; some cases leading to permanent blindness; one case reported extraocular extension of infection resulting in meningoencephalitis); Intraocular inflammation (some cases leading to permanent blindness; including a cluster of serious eye inflammation leading to blindness after compounding an anticancer chemotherapy product for intravenous administration) such as sterile endophthalmitis, uveitis, and vitritis; Retinal detachment (frequency not known); Retinal pigment epithelial tear (frequency not known); Intraocular pressure increased (frequency not known); Intraocular hemorrhage such as vitreous hemorrhage or retinal hemorrhage (frequency not known); Conjunctival hemorrhage (frequency not known). Following variable and non-validated methods in compounding, storage, and handling of bevacizumab, serious ocular adverse events (including infectious endophthalmitis and other ocular inflammatory conditions) affecting multiple patients have been reported.
Systemic Events (reported from unapproved intravitreal use): Increased risk for haemorrhagic stroke; Increased risk for overall mortality. Increased risk of serious systemic adverse events for bevacizumab, most of which resulted in hospitalization (adjusted risk ratio 1.29; 95% CI: 1.01, 1.66) (Incidence 24.1%; comparator 19.0%).
View ADR Monitoring Form