


 Sign Out
Sign Out


Pharmacodynamics: Lurasidone is an antagonist with high affinity binding at the dopamine D2 receptors (Ki of 1 nM) and the serotonin 5-HT2A (Ki of 0.5 nM) and 5-HT7 (Ki of 0.5 nM) receptors. It also binds with moderate affinity to the human α2C adrenergic receptors (Ki of 11 nM), is a partial agonist at serotonin 5-HT1A (Ki of 6.4 nM) receptors, and is an antagonist at the α2A adrenergic receptors (Ki of 41 nM). Lurasidone exhibits little or no affinity for histamine H1 and muscarinic M1 receptors (IC50 > 1,000 nM).
ECG Changes: The effects of LATUDA on the QTc interval were evaluated in a randomized, double-blind, multiple-dose, parallel-dedicated thorough QT study in 43 patients with schizophrenia or schizoaffective disorder, who were treated with LATUDA doses of 120 mg daily, 600 mg daily and completed the study. The maximum mean (upper 1-sided, 95% CI) increase in baseline-adjusted QTc intervals based on individual correction method (QTcI) was 7.5 (11.7) ms and 4.6 (9.5) ms, for the 120 mg and 600 mg dose groups respectively, observed at 2 to 4 hours after dosing. In this study, there was no apparent dose (exposure)-response relationship.
In short-term, placebo-controlled studies in schizophrenia and bipolar depression, no post-baseline QT prolongations exceeding 500 msec were reported in patients treated with LATUDA or placebo.
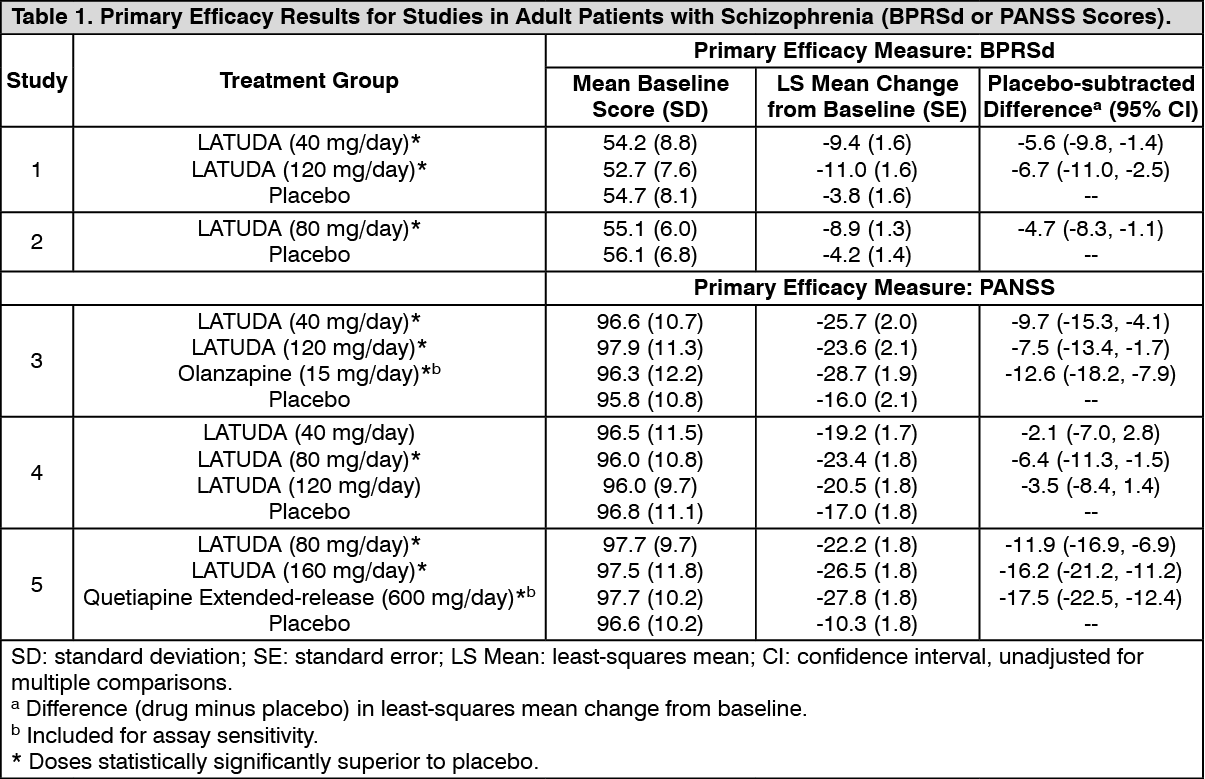
CLINICAL STUDIES: Schizophrenia: Adults: The efficacy of LATUDA for the treatment of schizophrenia was established in five short-term (6-week), placebo-controlled studies in adult patients (mean age of 38.4 years, range 18-72) who met DSM-IV criteria for schizophrenia. An active-control arm (olanzapine or quetiapine extended-release) was included in two studies to assess assay sensitivity.
Several instruments were used for assessing psychiatric signs and symptoms in these studies: 1. Positive and Negative Syndrome Scale (PANSS), is a multi-item inventory of general psychopathology used to evaluate the effects of drug treatment in schizophrenia. PANSS total scores may range from 30 to 210.
2. Brief Psychiatric Rating Scale derived (BPRSd), derived from the PANSS, is a multi-item inventory primarily focusing on positive symptoms of schizophrenia, whereas the PANSS includes a wider range of positive, negative and other symptoms of schizophrenia. The BPRSd consists of 18 items rated on a scale of 1 (not present) to 7 (severe). BPRSd scores may range from 18 to 126.
3. The Clinical Global Impression severity scale (CGI-S) is a clinician-rated scale that measures the subject's current illness state on a 1- to 7-point scale.
The endpoint associated with each instrument is change from baseline in the total score to the end of week 6. These changes are then compared to placebo changes for the drug and control groups.
The results of the studies follow: 1. Study 1: In a 6-week, placebo-controlled trial (N=145) involving two fixed doses of LATUDA (40 or 120 mg/day), both doses of LATUDA at Endpoint were superior to placebo on the BPRSd total score, and the CGI-S.
2. Study 2: In a 6-week, placebo-controlled trial (N=180) involving a fixed dose of LATUDA (80 mg/day), LATUDA at Endpoint was superior to placebo on the BPRSd total score, and the CGI-S.
3. Study 3: In a 6-week, placebo- and active-controlled trial (N=473) involving two fixed doses of LATUDA (40 or 120 mg/day) and an active control (olanzapine), both LATUDA doses and the active control at Endpoint were superior to placebo on the PANSS total score, and the CGI-S.
4. Study 4: In a 6-week, placebo-controlled trial (N=489) involving three fixed doses of LATUDA (40, 80 or 120 mg/day), only the 80 mg/day dose of LATUDA at Endpoint was superior to placebo on the PANSS total score, and the CGI-S.
5. Study 5: In a 6-week, placebo- and active-controlled trial (N=482) involving two fixed doses of LATUDA (80 or 160 mg/day) and an active control (quetiapine extended-release), both LATUDA doses and the active control at Endpoint were superior to placebo on the PANSS total score, and the CGI-S.
Thus, the efficacy of LATUDA at doses of 40, 80, 120 and 160 mg/day has been established (Table 1). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageExamination of population subgroups based on age (there were few patients over 65), gender and race did not reveal any clear evidence of differential responsiveness.
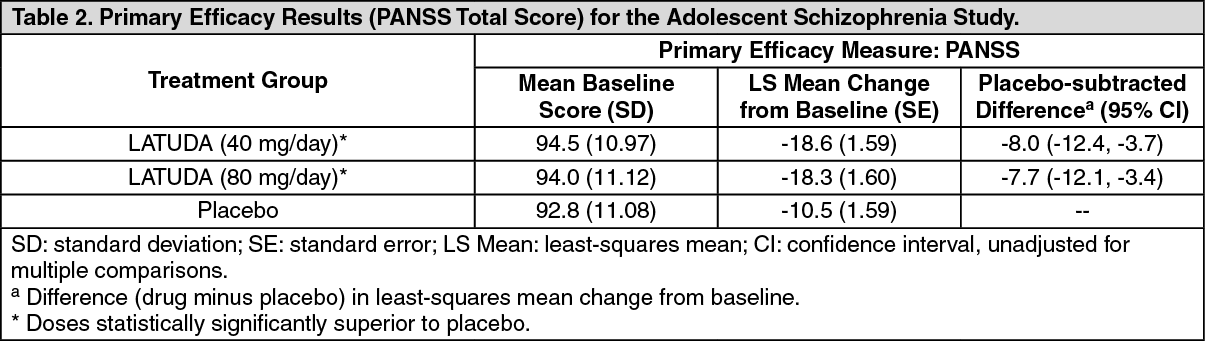
Adolescents (13-17 years): The efficacy of LATUDA, was established in a 6-week, multicenter, randomized, double-blind, placebo-controlled study of adolescents (13 to 17 years) who met DSM-IV-TR criteria for schizophrenia (N=326). Patients were randomized to one of two fixed-doses of LATUDA (40 or 80 mg/day) or placebo.
The primary rating instrument used to assess psychiatric signs and symptoms was the PANSS. The key secondary instrument was the CGI-S.
For both dose groups, LATUDA was superior to placebo in reduction of PANSS and CGI-S scores at Week 6. On average, the 80 mg/day dose did not provide additional benefit compared to the 40 mg/day dose.
The primary efficacy results are provided in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDepressive Episodes Associated with Bipolar I Disorder: Adults: Monotherapy: The efficacy of LATUDA, as monotherapy, was established in a 6-week, multicenter, randomized, double-blind, placebo-controlled study of adult patients (mean age of 41.5 years, range 18 to 74) who met DSM-IV-TR criteria for major depressive episodes associated with bipolar I disorder, with or without rapid cycling, and without psychotic features (N=485). Patients were randomized to one of two flexible-dose ranges of LATUDA (20 to 60 mg/day, or 80 to 120 mg/day) or placebo.
The primary rating instrument used to assess depressive symptoms in this study was the Montgomery-Asberg Depression Rating Scale (MADRS), a 10-item clinician-rated scale with total scores ranging from 0 (no depressive features) to 60 (maximum score). The primary endpoint was the change from baseline in MADRS score at Week 6. The key secondary instrument was the Clinical Global Impression-Bipolar-Severity of Illness scale (CGI-BP-S), a clinician-rated scale that measures the subject's current illness state on a 7-point scale, where a higher score is associated with greater illness severity.
For both dose groups, LATUDA was superior to placebo in reduction of MADRS and CGI-BP-S scores at Week 6. The primary efficacy results are provided in Table 3. The high dose range (80 to 120 mg per day) did not provide additional efficacy on average, compared to the low dose range (20 to 60 mg per day).
Adjunctive Therapy with Lithium or Valproate: The efficacy of LATUDA, as an adjunctive therapy with lithium or valproate, was established in a 6-week, multicenter, randomized, double-blind, placebo-controlled study of adult patients (mean age of 41.7 years, range 18 to 72) who met DSM-IV-TR criteria for major depressive episodes associated with bipolar I disorder, with or without rapid cycling, and without psychotic features (N=340). Patients who remained symptomatic after treatment with lithium or valproate were randomized to flexibly dosed LATUDA 20 to 120 mg/day or placebo.
The primary rating instrument used to assess depressive symptoms in this study was the MADRS. The primary endpoint was the change from baseline in MADRS score at Week 6. The key secondary instrument was the CGI-BP-S scale.
LATUDA was superior to placebo in reduction of MADRS and CGI-BP-S scores at Week 6, as an adjunctive therapy with lithium or valproate (Table 3). (See Table 3.)
 Click on icon to see table/diagram/image
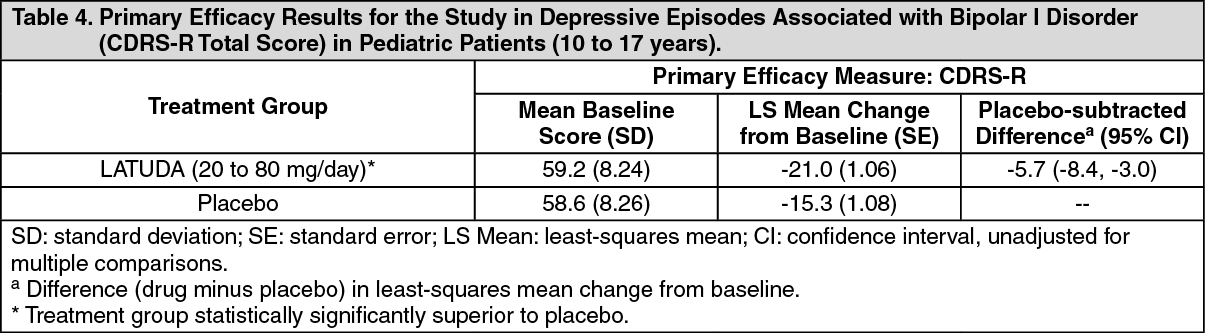
Click on icon to see table/diagram/imagePediatric Patients (10 to 17 years): The efficacy of LATUDA was established in a 6-week, multicenter, randomized, double-blind, placebo-controlled study of pediatric patients (10 to 17 years) who met DSM-5 criteria for a major depressive episode associated with bipolar I disorder, with or without rapid cycling, and without psychotic features (N=343). Patients were randomized to flexibly dosed LATUDA 20 to 80 mg/day or placebo. At the end of the clinical study, most patients (67%) received 20 mg/day or 40 mg/day.
The primary rating scale used to assess depressive symptoms in this study was the Children's Depression Rating Scale, Revised (CDRS-R) total score. The CDRS-R is a 17-item clinician-rated scale with total scores ranging from 17 to 113. The primary endpoint was the change from baseline in CDRS-R score at Week 6. The key secondary endpoint was the change from baseline in CGI-BP-S depression score.
LATUDA was superior to placebo in reduction of CDRS-R total score and CGI-BP-S depression score at Week 6. The primary efficacy results are provided in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Adults: The activity of LATUDA is primarily due to the parent drug. The pharmacokinetics of LATUDA is dose-proportional within a total daily dose range of 20 mg to 160 mg. Steady-state concentrations of LATUDA are reached within 7 days of starting LATUDA.
Following administration of 40 mg of LATUDA, the mean (%CV) elimination half-life was 18 (7) hours.
Absorption and Distribution: LATUDA is absorbed and reaches peak serum concentrations in approximately 1-3 hours. It is estimated that 9-19% of an administered dose is absorbed. Following administration of 40 mg of LATUDA, the mean (%CV) apparent volume of distribution was 6173 (17.2) L. LATUDA is highly bound (~99%) to serum proteins.
In a food effect study, LATUDA mean Cmax and AUC were about 3-times and 2-times, respectively, when administered with food compared to the levels observed under fasting conditions. LATUDA exposure was not affected as meal size was increased from 350 to 1000 calories and was independent of meal fat content [see Dosage & Administration].
In clinical studies, establishing the safety and efficacy of LATUDA, patients were instructed to take their daily dose with food [see Dosage & Administration].
Metabolism and Elimination: LATUDA is metabolized mainly via CYP3A4. The major biotransformation pathways are oxidative N-dealkylation, hydroxylation of norbornane ring, and S-oxidation. LATUDA is metabolized into two active metabolites (ID-14283 and ID-14326) and two major non-active metabolites (ID-20219 and ID-20220). Based on in vitro studies, LATUDA is not a substrate of CYP1A1, CYP1A2, CYP2A6, CYP4A11, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6 or CYP2E1 enzymes. Because LATUDA is not a substrate for CYP1A2, smoking is not expected to have an effect on the pharmacokinetics of LATUDA.
Transporter proteins: In vitro studies suggest LATUDA is not a substrate of OATP1B1 or OATP1B3, however, is probably a substrate of P-gp and BCRP. In vitro studies indicate that LATUDA is not expected to inhibit transporters OATP1B1, OATP1B3, OCT1, OCT2, OAT1, OAT3, MATE1, MATE2-K and BSEP at clinically relevant concentrations. LATUDA is not a clinically significant inhibitor of P-gp. However, it may inhibit BCRP.
Total excretion of radioactivity in urine and feces combined was approximately 89%, with about 80% recovered in feces and 9% recovered in urine, after a single dose of [14C]-labeled LATUDA.
Following administration of 40 mg of LATUDA, the mean (%CV) apparent clearance was 3902 (18.0) mL/min.
Drug Interaction Studies: Effects of other drugs on the exposure of lurasidone are summarized in Figure 1. A population PK analyses concluded that coadministration of lithium 300-2400 mg/day or valproate 300-2000 mg/day with lurasidone for up to 6 weeks has minimal effect on lurasidone exposure.
And the effects of LATUDA on the exposures of other drugs are summarized in Figure 2. A population PK analyses concluded that coadministration of lurasidone has minimal effect on lithium and valproate exposure when it is co-administered with lithium 300-2400 mg/day or valproate 300-2000 mg/day. (See Figures 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image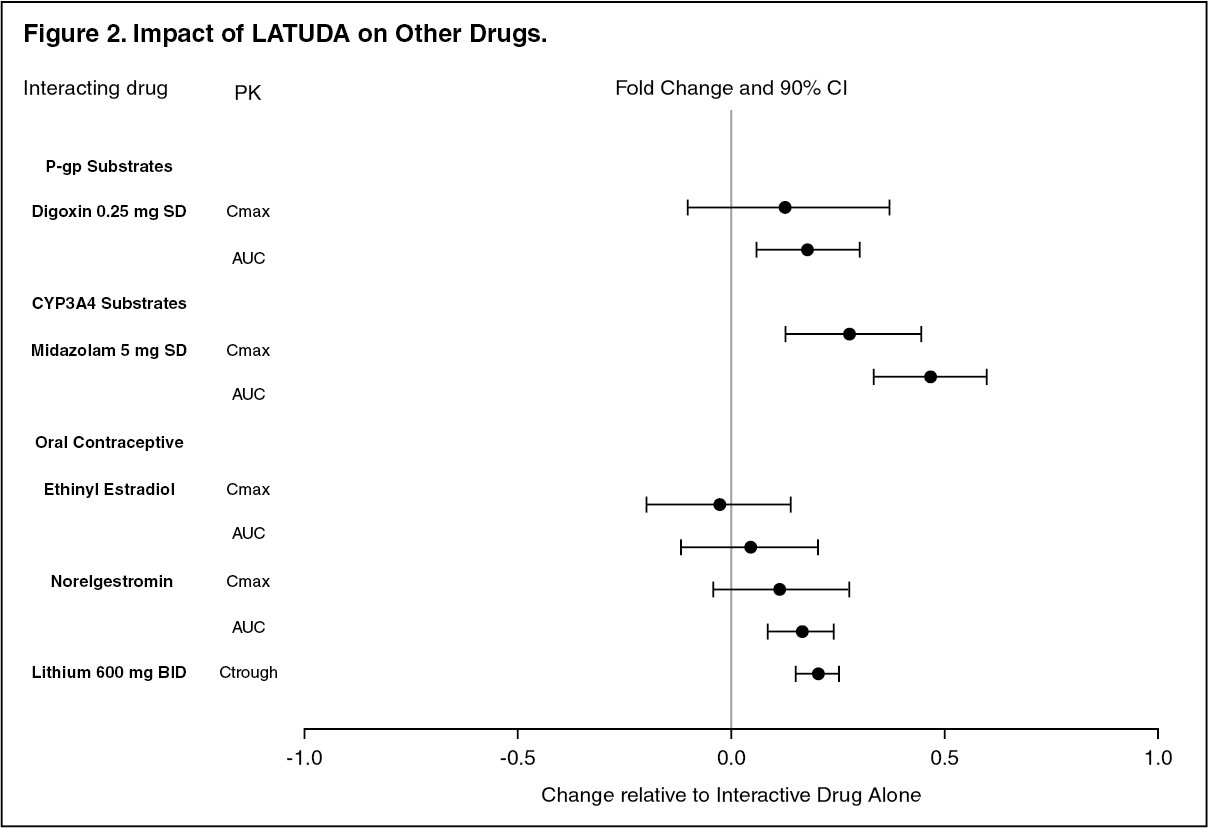 Click on icon to see table/diagram/image
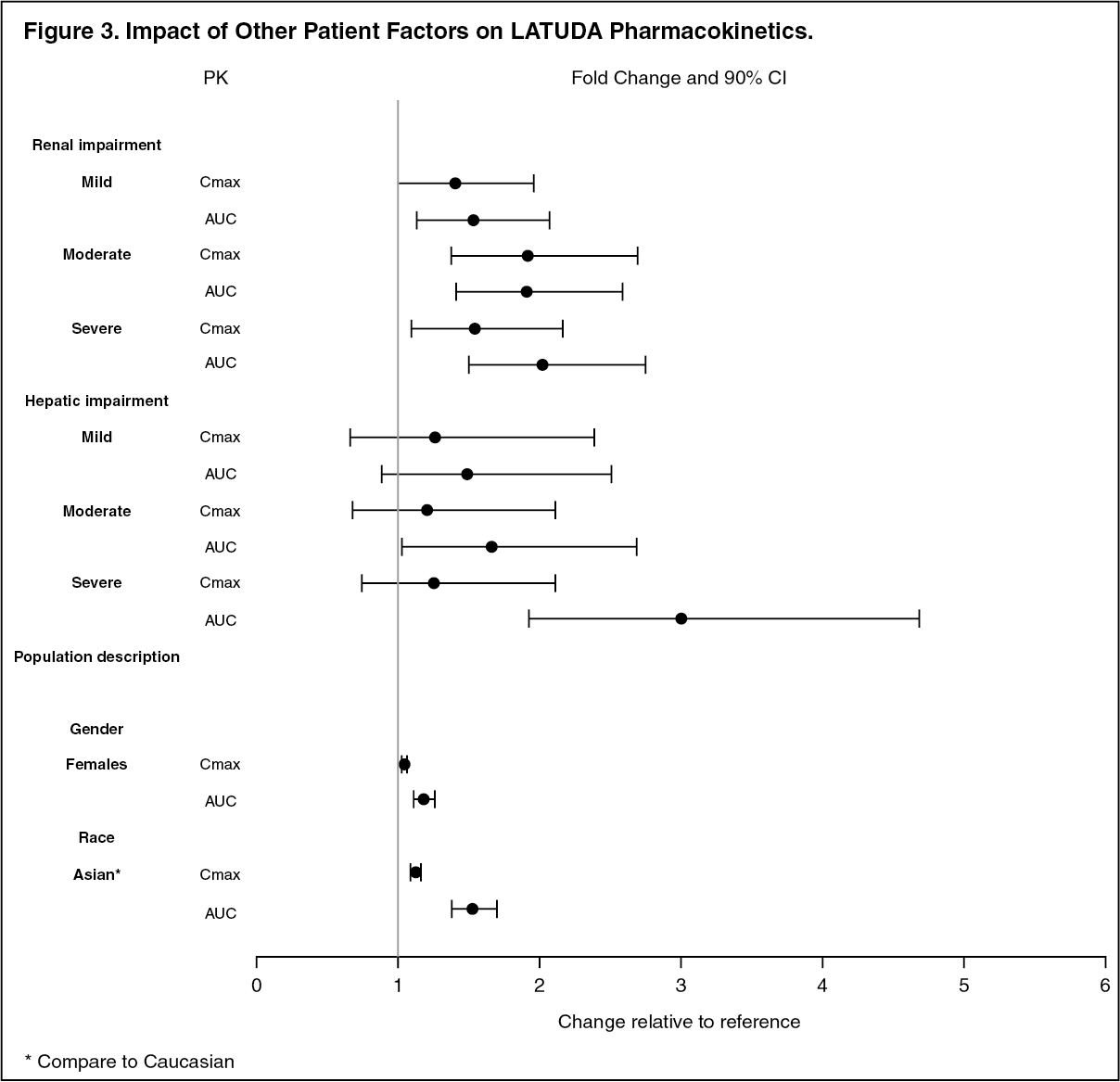
Click on icon to see table/diagram/imageStudies in Specific Populations: The effect of intrinsic patient factors on the pharmacokinetics of LATUDA is presented in Figure 3.
Pediatric Patients: LATUDA exposure (i.e., steady-state Cmax and AUC) in children and adolescent patients (10 to 17 years of age) was generally similar to that in adults across the dose range from 40 to 160 mg, without adjusting for body weight. (See Figure 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageToxicology: Preclinical safety data: Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenesis: Lurasidone increased incidences of malignant mammary gland tumors and pituitary gland adenomas in female mice orally dosed with 30, 100, 300, or 650 mg/kg/day. The lowest dose produced plasma levels (AUC) approximately equal to those in humans receiving the MRHD of 160 mg/day. No increases in tumors were seen in male mice up to the highest dose tested, which produced plasma levels (AUC) 14 times those in humans receiving the MRHD.
Lurasidone increased the incidence of mammary gland carcinomas in female rats orally dosed at 12 and 36 mg/kg/day: the lowest dose; 3 mg/kg/day is the no-effect dose which produced plasma levels (AUC) 0.4 times those in humans receiving the MRHD. No increases in tumors were seen in male rats up to the highest dose tested, which produced plasma levels (AUC) 6 times those in humans receiving the MRHD.
Proliferative and/or neoplastic changes in the mammary and pituitary glands of rodents have been observed following chronic administration of antipsychotic drugs and are considered to be prolactin-mediated [see Precautions].
Mutagenesis: Lurasidone did not cause mutation or chromosomal aberration when tested in vitro and in vivo test battery. Lurasidone was negative in the Ames gene mutation test, the Chinese Hamster Lung (CHL) cells, and in the in vivo mouse bone marrow micronucleus test up to 2000 mg/kg which is 61 times the MRHD of 160 mg/day based on mg/m2 body surface area.
Impairment of Fertility: Estrus cycle irregularities were seen in rats orally administered lurasidone at 1.5, 15 and 150 mg/kg/day for 15 consecutive days prior to mating, during the mating period, and through gestation day 7. No effect was seen at the lowest dose of 0.1 mg/kg which is approximately 0.006 times the MRHD of 160 mg/day based on mg/m2. Fertility was reduced only at the highest dose, which was reversible after a 14 day drug-free period. The no-effect dose for reduced fertility was approximately equal to the MRHD based on mg/m2.
Lurasidone had no effect on fertility in male rats treated orally for 64 consecutive days prior to mating and during the mating period at doses up to 9 times the MRHD based on mg/m2.