Adult: Doses are expressed in terms of lurasidone hydrochloride; approx 37 mg lurasidone base is equivalent to 40 mg lurasidone hydrochloride. For treatment of depressive episodes associated with bipolar I disorder, as monotherapy or in combination with lithium or valproate: Initially, 20 mg once daily. Dose may be increased based on clinical response and tolerability. Max: 120 mg daily. Child: 10-17 years For treatment of depressive episodes associated with bipolar I disorder, as monotherapy: Initially, 20 mg once daily. May increase dose after 1 week based on clinical response and tolerability. Max: 80 mg daily. Treatment recommendations may vary among countries (refer to specific product guidelines).
Oral Schizophrenia
Adult: Doses are expressed in terms of lurasidone hydrochloride; approx 37 mg lurasidone base is equivalent to 40 mg lurasidone hydrochloride. Initially, 40 mg once daily. Dose may be increased based on clinical response and tolerability. Max: 160 mg daily. Child: 13-17 years Initially, 40 mg once daily. Dose may be increased based on clinical response and tolerability. Max: 80 mg daily.
Special Patient Group
Patients receiving moderate CYP3A4 inhibitors (e.g. diltiazem, atazanavir, erythromycin, fluconazole, verapamil): If moderate CYP3A4 inhibitor is added to treatment in patients receiving lurasidone, reduce lurasidone dose to half of the original dose. If lurasidone is added to treatment in patients receiving moderate CYP3A4 inhibitor, initiate lurasidone dose at 20 mg daily, Max of 80 mg daily.
Patients receiving moderate CYP3A4 inducers (e.g. efavirenz): Dose of lurasidone may need to be increased after chronic treatment (7 days or more) with the CYP3A4 inducer.
Renal Impairment
CrCl (mL/min)
Dosage
<50
Initially, 20 mg daily. Max: 80 mg daily.
Hepatic Impairment
Moderate (Child-Pugh class B): Initially, 20 mg daily. Max: 80 mg daily. Severe (Child-Pugh class C): Initially, 20 mg daily. Max: 40 mg daily.
Administration
tab: Should be taken with food.
Contraindications
Concomitant use with strong CYP3A4 inhibitors (e.g. clarithromycin, ketoconazole, voriconazole, ritonavir, mibefradil) and strong CYP3A4 inducers (e.g. carbamazepine, phenytoin, rifampicin, St. John's wort).
Special Precautions
Patient with known or history of CV disease (e.g. previous MI, ischaemic heart disease, heart failure); history of cerebrovascular disease, condition predisposing to orthostatic hypotension (e.g. dehydration, hypovolaemia, receiving concomitant antihypertensive treatment); history of seizures or condition that may lower seizure threshold (e.g. Alzheimer's disease); Parkinson's disease; diabetes or risk factors for diabetes mellitus (e.g. family history of diabetes, obesity); condition that may elevate core body temperature (e.g. undergoing strenuous exercise, exposure to extreme heat, concomitant use of anticholinergic agents); pre-existing low WBC count, history of drug-induced leucopenia or neutropenia; at risk of aspiration pneumonia. Not intended for the treatment of dementia-related psychosis. Patient taking moderate CYP3A4 inhibitor or inducer. Avoid abrupt withdrawal. Renal and hepatic impairment. Children and elderly. Pregnancy and lactation.
Adverse Reactions
Significant: Orthostatic hypotension, syncope, sedating effects (e.g. drowsiness), increased risk of falls; increased risk of suicidal thoughts and behaviour; extrapyramidal symptoms (e.g. akathisia, drug-induced parkinsonism, dystonia; rarely, tardive dyskinesia); VTE; metabolic changes (including dyslipidaemia, weight gain, and hyperglycaemia), hyperprolactinaemia (some cases may lead to gynaecomastia, galactorrhoea, amenorrhoea, and erectile dysfunction); activation of mania or hypomania; oesophageal dysmotility and aspiration; altered cardiac conduction, temperature dysregulation. Rarely, haematologic abnormalities (e.g. neutropenia, leucopenia, thrombocytopenia, anaemia). Cardiac disorders: Tachycardia. Gastrointestinal disorders: Nausea, vomiting, diarrhoea, dyspepsia, salivary hypersecretion, dry mouth, stomach discomfort, upper abdominal pain. General disorders and administration site conditions: Fatigue. Immune system disorders: Hypersensitivity. Investigations: Increased serum creatinine, increased blood creatine phosphokinase. Metabolism and nutrition disorders: Decreased appetite. Musculoskeletal and connective tissue disorders: Back pain, musculoskeletal stiffness. Nervous system disorders: Dizziness. Psychiatric disorders: Insomnia, agitation, anxiety, restlessness. Skin and subcutaneous tissue disorders: Rash, pruritus. Vascular disorders: Hypertension. Potentially Fatal: Increased risk of CVA and transient ischaemic attack (particularly in elderly patients with dementia); neuroleptic malignant syndrome.
Patient Counseling Information
This drug may cause drowsiness or impaired thinking, judgement, or motor skills, if affected, do not drive or operate machinery.
Monitoring Parameters
Monitor electrolytes, renal function, LFTs, and TSH annually; lipid panel 12 weeks after initiation of treatment and dose adjustment, then annually; CBC as clinically indicated. Monitor for clinical worsening and for emergence of suicidal thoughts and behaviour. Regularly assess adherence, risk for fall, mental status and alertness; signs and symptoms of hyperprolactinaemia at every visit, and extrapyramidal symptoms every visit, 4 weeks after initiation and dose adjustment, then annually. Obtain vital signs (e.g. blood pressure, pulse, temperature, orthostatics) at least weekly during the 1st 3-4 weeks of therapy, then 4 weeks after dose adjustment; fasting blood glucose at the start of treatment and periodically throughout. Monitor weight before initiating treatment and periodically during treatment. Evaluate for personal and family history of metabolic syndrome and history of drug abuse.
Drug Interactions
May increase exposure with moderate CYP3A4 inhibitors (e.g. atazanavir, erythromycin, fluconazole, diltiazem, verapamil). May decrease exposure with moderate CYP3A4 inducers (e.g. bosentan, efavirenz, etravirine, modafinil, nafcillin). May result in additive CNS effects with other CNS agents. May increase the exposure of midazolam. Potentially Fatal: Increased exposure with strong CYP3A4 inhibitors (e.g. clarithromycin, ketoconazole, voriconazole, mibefradil, ritonavir). Decreased serum concentration with strong CYP3A4 inducers (e.g. carbamazepine, phenytoin, rifampicin). Concomitant use with other serotonergic agents (e.g. opioids, MAOIs, SSRIs, SNRIs, TCAs) may result in serotonin syndrome.
Food Interaction
Increased absorption with food (containing at least 350 calories). May increase serum concentration with grapefruit or grapefruit juice. Decreased serum concentration with St. John's wort. May result in additive CNS effects with alcohol.
Action
Description: Mechanism of Action: Lurasidone is a benzisothiazol-derivative atypical antipsychotic. The exact mechanism of action in bipolar depression and schizophrenia is unknown; however, it has been suggested that its action may be mediated by combination of serotonin-dopamine antagonist activity. Lurasidone is an antagonist with high affinity at dopamine D2, serotonin 5-HT2A and 5-HT7 receptors and with moderate affinity at α2C-adrenergic receptors. It also acts as a partial agonist at 5-HT1A receptors and has no significant affinity for histamine H1 and muscarinic M1 receptors. Onset: Depressive episode of bipolar disorder: Within 1 week. Schizophrenia: Within 1-2 weeks. Pharmacokinetics: Absorption: Rapidly absorbed. Food increases absorption. Bioavailability: 9-19%. Time to peak plasma concentration: Approx 1-3 hours. Distribution: Volume of distribution: 6,173 L. Plasma protein binding: Approx 99%, including albumin and α1-acid glycoprotein. Metabolism: Metabolised in the liver via oxidative N-dealkylation, hydroxylation of norbornane ring and S-oxidation mainly by CYP3A4 into 2 active metabolites (ID-14283 and ID-14326) and 2 major inactive metabolites (ID-20219 and ID-20220). Excretion: Via faeces (approx 80%); urine (approx 9%). Elimination half-life: 18-40 hours.
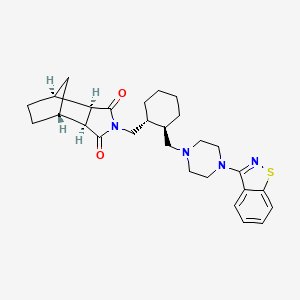
Chemical Structure
Lurasidone Source: National Center for Biotechnology Information. PubChem Compound Summary for CID 213046, Lurasidone. https://pubchem.ncbi.nlm.nih.gov/compound/Lurasidone. Accessed Oct. 25, 2023.
N05AE05 - lurasidone ; Belongs to the class of indole derivatives antipsychotics.
References
Anon. Lurasidone. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 06/07/2023.Anon. Lurasidone. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 06/07/2023.Buckingham R (ed). Lurasidone. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 06/07/2023.Joint Formulary Committee. Lurasidone Hydrochloride. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 06/07/2023.Latuda 20 mg, 40 mg, and 80 mg Film-coated Tablets (Sumitomo Pharma Malaysia Sdn. Bhd.). National Pharmaceutical Regulatory Agency - Ministry of Health Malaysia. https://www.npra.gov.my. Accessed 06/07/2023.Latuda 74 mg Film-coated Tablets (CNX Therapeutics Ltd.). MHRA. https://products.mhra.gov.uk. Accessed 06/07/2023.Lurasidone Hydrochloride Tablet (Aurobindo Pharma Limited). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed. Accessed 06/07/2023.



 Sign Out
Sign Out