Tablets containing 40mg thioguanine.
Excipients/Inactive Ingredients: Lactose monohydrate, Potato starch, Acacia, Stearic acid, Magnesium stearate.
Pharmacotherapeutic group: Anti-neoplastic and immunomodulating agent/purine analogue. ATC code: L01BB03.
Pharmacology: Pharmacodynamics: Thioguanine is a sulphydryl analogue of guanine and behaves as a purine antimetabolite. It is activated to its nucleotide, thioguanylic acid.
Thioguanine metabolites inhibit de novo purine synthesis and purine nucleotide interconversions. Thioguanine is also incorporated into nucleic acids and DNA (deoxyribonucleic acid) incorporation is claimed to contribute to the agent's cytotoxicity.
There is usually a cross-resistance between thioguanine and mercaptopurine: it is therefore not to be expected that patients with a tumour resistant to one will respond to the other.
Pharmacokinetics: Absorption: Studies with radioactive thioguanine show that peak blood levels of total radioactivity are achieved about 8 to 10 h after oral administration and decline slowly thereafter. Later studies using HPLC have shown 6-thioguanine to be the major thiopurine present for at least the first 8 h after intravenous administration. Peak plasma concentrations of 61 to 118 nanomol (nmol)/ml are obtainable following intravenous administration of 1 to 1.2 g of 6-thioguanine/m2 body surface area. Plasma levels decay biexponentially with initial and terminal half lives of 3 and 5.9 h, respectively.
Following oral administration of 100 mg/m2, peak levels as measured by HPLC occur at 2 to 4 h and lie in the range of 0.03 to 0.94 micromolar (0.03 to 0.94 nmol/ml). Levels are reduced by concurrent food intake (as well as vomiting).
Distribution: Limited data on the distribution of TG in humans are available in the scientific literature.
6-TG penetrates into the CSF following constant IV infusion administration after doses of 20 mg/m2/h over 24 hours in children with ALL.
Biotransformation: Thioguanine is extensively metabolised in vivo. The four different enzymes responsible for 6-TG metabolism are as follows: hypoxanthine (guanine) phosphoribosyl transferase (H(G)PRT), which converts 6-TG into thioguanosine monophosphate (6-TGMP), which is further metabolized by protein kinases to the active species, thioguanine nucleotides (6-TGN); TPMT, which converts 6-TG to 6-methylthioguanine (6-MTG, inactive metabolite) as well as 6-TGMP to 6-methyl-TGMP (an inactive metabolite) and xanthine oxidase (XDH or XO) and aldehyde oxidase (AO), which also convert 6-TG into inactive metabolites. 6-TG is initially deaminated by guanine deaminase (GDA) to form 6-thioxanthine (6-TX) and this becomes a substrate for the XDH catalysed formation of 6-thiouric acid (6-TUA).
NUDT15 R139C (NUDT15 c.415C>T) Variant: Recent studies indicate that a strong association exists between the NUDT15 variant NUDT15 c.415C>T [pArg139Cys] (also known as NUDT15 R139C [rs116855232], which is thought to lead to a loss of function of the NUDT15 enzyme, and thiopurine-mediated toxicity such as leukopenia and alopecia. The frequency of NUDT15 c415C>T has an ethnic variability of 9.8% in East Asians, 3.9% in Hispanics, 0.2% in Europeans and 0.0% in Africans, indicating an increased risk for the Asian population. Patients who are NUDT15 variant homozygotes (NUDT15 T risk alleles) are at an excessive risk of thiopurine toxicity compared with the C homozygotes.
Reduced thiopurine doses of patients who carry the NUDT15 variants may decrease their risk of toxicity. Therefore, genotypic analysis determining NUDT15 genotype should be determined for all patients, including paediatric patients, prior to initiating thiopurine treatment (see Dosage & Administration). The prescribing physician is advised to establish whether dose reduction is required based on patient response to treatment as well as their genetic profile.
Patients with variants in both the NUDT15 and TPMP enzymes are significantly less tolerant of thiopurines than those with risk alleles in only one of these two genes.
The precise mechanism of NUDT15-associated thiopurine-related toxicity is not understood.
LANVIS is indicated primarily for the treatment of acute leukaemias especially, acute myelogenous leukaemia and acute lymphoblastic leukaemia.
The exact dose and duration of administration will depend on the nature and dosage of other cytotoxic drugs given in conjunction with LANVIS.
LANVIS is variably absorbed following oral administration and plasma drug levels may be reduced following emesis or intake of food.
LANVIS can be used at various stages of treatment in short term cycles. However it is not recommended for use during maintenance therapy or similar long term continuous treatments due to the high risk of liver toxicity (see Precautions and Adverse Reactions).
Induction therapy: For adults, the usual dosage of LANVIS is between 60 and 200 mg/m2 body surface area per day.
For children, similar dosages to those used in adults, with appropriate correction for body surface area have been used.
Elderly patients: There are no specific dosage recommendations in elderly patients (See Dosage in renal or hepatic impairment as follows). LANVIS has been used in various combination chemotherapy schedules in elderly patients with acute leukaemia at equivalent dosages to those used in younger patients.
Dosage in renal or hepatic impairment: Consideration should be given to reducing the dosage in patients with impaired hepatic or renal function.
TPMT-deficient patients: Patients with inherited little or no thiopurine S-methyltransferase (TPMT) activity are at increased risk for severe thioguanine toxicity from conventional doses of thioguanine and generally require substantial dose reduction. The optimal starting dose for homozygous deficient patients has not been established (see Monitoring under Precautions and Pharmacology: Pharmacokinetics under Actions).
Most patients with heterozygous TPMT deficiency can tolerate recommended thioguanine doses, but some may require dose reduction. Genotypic and phenotypic tests of TPMT are available (see Monitoring under Precautions and Pharmacology: Pharmacokinetics under Actions). Consideration should be given to reducing the dosage in patients with impaired hepatic function.
Patients with NUDT15 variant: Patients with inherited mutated NUDT15 gene are at increased risk for severe thiopurine toxicity, such as early leukopenia and alopecia, from conventional doses of thiopurine therapy and generally require substantial dose reduction. Patients of Asian ethnicity are particularly at risk, due to the increased frequency of the mutation in this population. The optimal starting dose for heterozygous or homozygous deficient patients has not been established.
Genotypic and phenotypic testing of NUDT15 variants should be considered before initiating thiopurine therapy in all patients (including paediatric patients) to reduce the risk of thiopurine-related severe leukocytopenia and alopecia, especially in Asian populations (see Pharmacology: Pharmacokinetics under Actions).
Symptoms: The principal toxic effect is on the bone marrow and haematological toxicity is likely to be more profound with chronic overdosage than with a single ingestion of LANVIS.
Treatment: As there is no known antidote the blood picture should be closely monitored and general supportive measures, together with appropriate blood transfusion, instituted if necessary.
Further management should be as clinically indicated or as recommended by the national poisons centre, where available.
Hypersensitivity to the active substance or to any of the excipients listed in Description. In view of the seriousness of the indications there are no other absolute contraindications.
LANVIS IS AN ACTIVE CYTOTOXIC AGENT FOR USE ONLY UNDER THE DIRECTION OF PHYSICIANS EXPERIENCED IN THE ADMINISTRATION OF SUCH AGENTS.
Immunisation using a live organism vaccine has the potential to cause infection in immunocompromised hosts. Therefore, immunisations with live organism vaccines are not recommended. In all cases, patients in remission should not receive live organism vaccines until at least 3 months after their chemotherapy treatment has been completed.
Hepatic Effects: LANVIS IS NOT RECOMMENDED FOR MAINTENANCE THERAPY OR SIMILAR LONG TERM CONTINUOUS TREATMENTS DUE TO THE HIGH RISK OF LIVER TOXICITY ASSOCIATED WITH VASCULAR ENDOTHELIAL DAMAGE (see Dosage & Administration and Adverse Reactions).
This liver toxicity has been observed in a high proportion of children receiving LANVIS as part of maintenance therapy for acute lymphoblastic leukaemia and in other conditions associated with continuous use of LANVIS. This liver toxicity is particularly prevalent in males. Liver toxicity usually presents as the clinical syndrome of hepatic veno-occlusive disease (hyperbilirubinaemia, tender hepatomegaly, weight gain due to fluid retention and ascites) or with signs of portal hypertension (splenomegaly, thrombocytopenia and oesophageal varices). Histopathological features associated with this toxicity include hepatoportal sclerosis, nodular regenerative hyperplasia, peliosis hepatis and periportal fibrosis.
LANVIS therapy should be discontinued in patients with evidence of liver toxicity as reversal of signs and symptoms of liver toxicity have been reported upon withdrawal.
Patients must be carefully monitored during therapy including blood cell counts and weekly liver function tests. Early indications of liver toxicity are signs associated with portal hypertension such as thrombocytopenia out of proportion with neutropenia and splenomegaly. Elevations of liver enzymes have also been reported in association with liver toxicity but do not always occur.
Haematological Effects: Treatment with LANVIS causes bone marrow suppression leading to leucopoenia and thrombocytopenia (see Hepatic Effects as previously mentioned). Anaemia has been reported less frequently. Bone marrow suppression is readily reversible if LANVIS is withdrawn early enough.
Thiopurine S-methyltransferase (TPMT) deficiency: There are individuals with an inherited deficiency of the enzyme TPMT who may be unusually sensitive to the myelosuppressive effect of LANVIS and prone to developing rapid bone marrow depression following the initiation of treatment with LANVIS. This problem could be exacerbated by coadministration with drugs that inhibit TPMT, such as olsalazine, mesalazine or sulphasalazine. Some laboratories offer testing for TPMT deficiency, although these tests have not been shown to identify all patients at risk of severe toxicity. Therefore close monitoring of blood counts is still necessary.
Patients with NUDT15 variant: Patients with inherited mutated NUDT15 gene are at increased risk for severe thiopurine toxicity, such as early leukopenia and alopecia, from conventional doses of thiopurine therapy and generally require substantial dose reduction. Patients of Asian ethnicity are particularly at risk, due to the increased frequency of the mutation in this population. The optimal starting dose for heterozygous or homozygous deficient patients has not been established. Genotypic and phenotypic testing of NUDT15 variants should be considered before initiating thiopurine therapy in all patients (including paediatric patients) to reduce the risk of thiopurine-related severe leukocytopenia and alopecia, especially in Asian populations (see Pharmacology: Pharmacokinetics under Actions).
During remission induction in acute myelogenous leukaemia the patient may frequently have to survive a period of relative bone marrow aplasia and it is important that adequate supportive facilities are available.
Patients on myelosuppressive chemotherapy are particularly susceptible to a variety of infections.
During remission induction, particularly when rapid cell lysis is occurring, adequate precautions should be taken to avoid hyperuricaemia and/or hyperuricosuria and the risk of uric acid nephropathy (see Adverse Reactions).
Monitoring: SINCE 6-THIOGUANINE IS STRONGLY MYELOSUPPRESSIVE FULL BLOOD COUNTS MUST BE CARRIED OUT FREQUENTLY DURING REMISSION INDUCTION. PATIENTS MUST BE CAREFULLY MONITORED DURING THERAPY.
The leucocyte and platelet counts continue to fall after treatment is stopped, so at the first sign of an abnormally large fall in these counts, treatment should be temporarily discontinued.
Lesch-Nyhan syndrome: Since the enzyme hypoxanthine guanine phosphoribosyl transferase is responsible for the conversion of thioguanine to its active metabolite, it is possible that patients deficient in this enzyme, such as those suffering from Lesch-Nyhan syndrome, may be resistant to the drug. Resistance to azathioprine, which has one of the same active metabolites as thioguanine, has been demonstrated in two children with Lesch-Nyhan syndrome.
UV Exposure: Patient treated with 6-thioguanine are more sensitive to the sun. Exposure to sunlight and UV light should be limited, and patients should be recommended to wear protective clothing and to use a sunscreen with a high protection factor.
Mutagenicity and Carcinogenicity: In view of its action on DNA, LANVIS is potentially mutagenic and carcinogenic.
EFFECTS ON ABILITY TO DRIVE AND USE MACHINES: There are no data on the effect of LANVIS on driving performance or the ability to operate machinery. A detrimental effect on these activities cannot be predicted from the pharmacology of the drug.
LANVIS like other cytotoxic agents is potentially teratogenic.
There have been isolated cases where men who have received combinations of cytotoxic agents including LANVIS, have fathered children with congenital abnormalities.
The use of LANVIS should be avoided whenever possible during pregnancy, particularly during the first trimester. In any individual case the potential hazard to the foetus must be balanced against the expected benefit to the mother.
As with all cytotoxic chemotherapy, adequate contraceptive precautions should be advised when either partner is receiving LANVIS.
There are no reports documenting the presence of thioguanine or its metabolites in maternal milk. It is suggested that mothers receiving LANVIS should not breast feed.
For this product there is a lack of modern clinical documentation which can be used as support for determining the frequency of undesirable effects. LANVIS is usually one component of combination chemotherapy and consequently it is not possible to ascribe the side effects unequivocally to this drug alone.
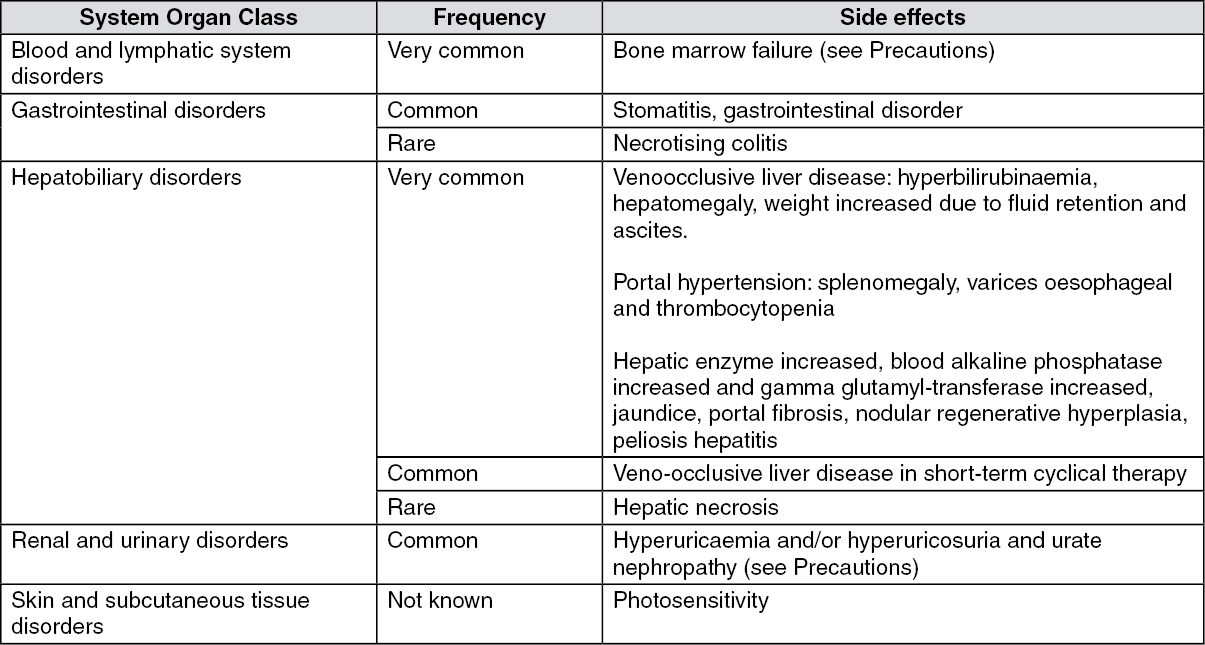
The following convention has been utilised for the classification of frequency of undesirable effects: very common ≥1/10 (≥10%), common ≥1/100 and < 1/10 (≥ 1% and <10%), uncommon ≥1/1000 and <1/100 (≥0.1% and <1%), rare ≥1/10,000 and <1/1000 (≥0.01% and <0.1%), very rare <1/10.000 (<0.01%). (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions: Hepatobiliary disorders:
Click on icon to see table/diagram/image
Description of selected adverse reactions: Hepatobiliary disorders: The liver toxicity associated with vascular endothelial damage occurs at a frequency of very common when thioguanine is used in maintenance or similar long term continuous therapy which is not recommended (see Dosage & Administration and Precautions).
Rare: Centrilobular hepatic necrosis has been reported in a few cases including patients receiving combination chemotherapy, oral contraceptives, high dose thioguanine and alcohol.
Reversal of signs and symptoms of this liver toxicity has been reported upon withdrawal of short term or long term continuous therapy.
Vaccines: Vaccinations with live organism vaccines are not recommended in immunocompromised individuals (see Precautions).
Other myelotoxic substances or radiation therapy: During concomitant administration of other myelotoxic substances or radiation therapy, the risk of myelosuppression is increased.
Allopurinol: The concomitant use of allopurinol to inhibit uric acid formation does not necessitate reduction of dosage of LANVIS as is necessary with mercaptopurine and azathioprine.
Aminosalicylate derivatives: As there is in vitro evidence that aminosalicylate derivatives (e.g. olsalazine, meslazine or sulphasalazine) inhibit the TPMT enzyme, they should be administered with caution to patients receiving concurrent LANVIS therapy (see Precautions).
Instructions for Use/Handling: Safe Handling of LANVIS: It is recommended that the handling of LANVIS tablets follows the 'Guidelines for the Handling of Cytotoxic Drugs' according to prevailing local recommendations and/or regulations. If halving of a tablet is required, care should be taken not to contaminate the hands or inhale the drug.
Disposal: LANVIS tablets surplus to requirements should be destroyed in a manner appropriate to the prevailing local regulations for the destruction of dangerous substances.
Incompatibilities: None reported.
Store below 30°C.
Protect from light.
Keep dry.
L01BB03 - tioguanine ; Belongs to the class of antimetabolites, purine analogues. Used in the treatment of cancer.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
