Levobupivacaine hydrochloride.
Each ml contains: Levobupivacaine HCl monohydrate 5.94 mg/ml equivalent to levobupivacaine 5 mg.
Clear, colorless solution, not more intensly coloured than reference solution B9 after dilution.
B9 is volumes in 1.0 ml standard solution B in 99.0 hydrochloric acid (~10 g/l) TS.
Pharmacology: Levobupivacaine is a member of the amino amide class of local anesthetics. Local anesthetics block the generation and the conduction of nerve impulses by increasing the threshold for electrical excitation in the nerve, by slowing propagation of the nerve impulse, and by reducing the rate of rise of the action potential. In general, the progression of anesthesia is related to the diameter, myelination, and conduction velocity of affected nerve fibers. Clinically, the order of loss of nerve function is as follows: 1) pain; 2) temperature; 3) touch; 4) proprioception; and 5) skeletal muscle tone.
Pharmacodynamics: Levobupivacaine can be expected to share the pharmacodynamic properties of other local anesthetics. Systemic absorption of local anesthetics can produce effects on the central nervous system and cardiovascular systems. At blood concentrations achieved with therapeutic doses, changes in cardiac conduction, excitability, refractoriness, contractility, and peripheral vascular resistance have been reported. Toxic blood concentrations depress cardiac conduction and excitability, which may lead to atrioventricular block, ventricular arrhythmias, and cardiac arrest, sometimes resulting in death. In addition, myocardial contractility is depressed and peripheral vasodilation occurs, leading to decreased cardiac output and arterial blood pressure.
Following systemic absorption, local anesthetics can produce central nervous system stimulation, depression, or both. Apparent central nervous system stimulation is usually manifested as restlessness, tremors, and shivering, progressing to convulsions. Ultimately central nervous system depression may progress to coma and cardio-respiratory arrest. However, the local anesthetics have a primary depressant effect on the medulla and on higher centers. The depressed stage may occur without a prior excited stage.
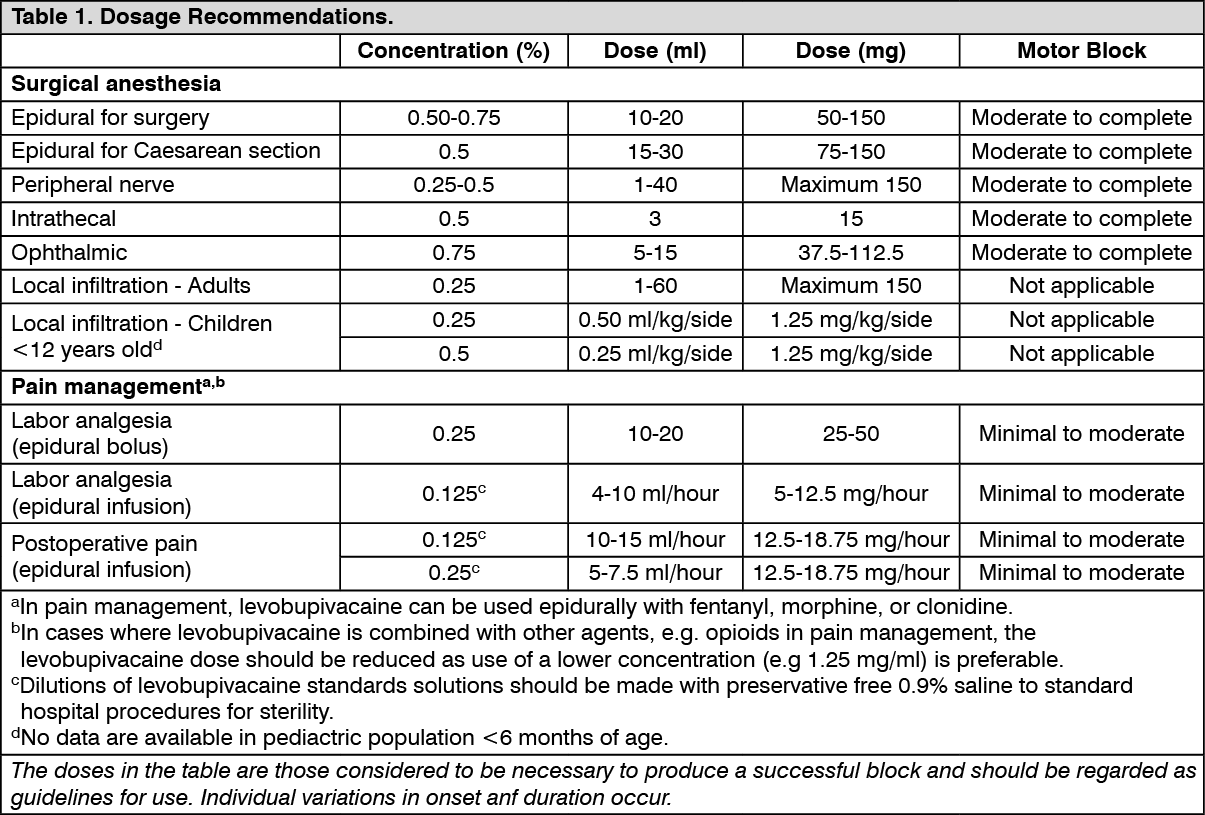
Adults: Levobupivacaine is indicated in adults for: Surgical Anesthesia: Major: epidural (for obstetric procedures, including Caesarean section, concentrations higher than 0.5% are not recommended, see Contraindications, Precautions, Use in Pregnancy & Lactation), intrathecal, peripheral nerve block.
Minor: local infiltration, peribulbar block in ophthalmic surgery.
Pain Management: Continous epidural infusion, single or multiple bolus administration for postoperative, labor or chronic pain.
For continuous epidural analgesia, levobupivacaine may be administered in combination with epidural fentanyl, morphine, or clonidine.
Children: Levobupivacaine is indicated in children for infiltration analgesia (ilioinguinal/iliohypogastric blocks). No data are available in pediatric population <6 months of age.
The rapid injection of a large volume of local anesthetic solution should be avoided and fractional (incremental) doses should always be used. The smallest dose and concentration required to produce the desired result should be administered. The dose of any local anesthetic differs with the anesthetic procedure, the area to be anesthetized, the vascularity of the tissues, the number of neuronal segments to be blocked, the intensity of the block, the degree of muscle relaxation required, the duration of the anesthesia desired, individual tolerance, and the physical condition of the patient. Patients in poor general condition due to aging or other compromising factors, such as impaired cardiovascular function, advanced liver disease, or several renal dysfunction, require special attention.
To reduce the risk of potentially serious adverse reactions, attempts should be made to optimize the patient's condition before major blocks are performed, and the dosage should be adjusted accordingly. Use an adequate test dose (3 to 5 ml) of a short-acting local anesthetic solution containing epinephrine prior to induction ofcomplete nerve block. This test dose should be repeated if the patient is moved in such a fashion as to have displaced the epidural catheter. It is recommended that adequate time be allowed for the onset of anesthesia following administration of each test dose.
The use of levobupivacaine hydrochloride monohydrate is not recommended for more than 24 hours (see Precautions).
Disinfecting agents containing heavy metals, which cause release of ions (mercury, zinc, copper, etc.) should not be used for skin or mucous membrane disinfection since they have been related to incidents of swelling and edema.
When chemical disinfection of the container surface is desired, either isopropyl alcohol (91%) or ethyl alcohol (70%) is recommended. It is recommended that chemical disinfection be accomplished by wiping the ampule thoroughly with cotton or gauze that has been moistened with the recommended alcohol prior to use.
These products are intended for single use and do not contain preservatives; any solution remaining from an open container should be discarded. For specific techniques and procedures, refer to standard contemporary textbooks.
Levobupivacaine hydrochloride monohydrate compatibility: Levobupivacaine hydrochloride monohydrate is compatible with 0.9% sodium chloride injection.
Dilution stability: After dilution in 0.9% sodium chloride solution, levobupivacaine hydrochloride monohydrate is physically and chemically stable at temperature 30°C for 7 days. Aseptic technique should be used to prepare the diluted products. Admixtures of levobupivacaine should be prepared for single patient use only. The unused portion of diluted levobupivacaine hydrochloride monohydrate should be discarded after each use.
From a microbiological poin of view, the product should be used immediately. If not used immediately, in-use storage times and conditions prior to use are the responsibility of the user and would normally not be longer than 24 hours at 2 to 8°C.
Note: parenteral products should be inspected visually for particulate matter and discoloration prior to administration whenever solution and container permit. Solutions that are not clear and colorless should not be used. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Epidural doses of up to 375 mg have been administered incrementally to patients during a surgical procedure.
The maximum dose in 24 hours for intraoperative block and postoperative pain management was 695 mg.
The maximum dose administered as a postoperative epidural infusion over 24 hours was 570 mg.
The maximum dose administered to patients as a single fractionated injection was 300 mg for brachial plexus block.
For Caesarean section, the maximum recommended dose is 150 mg.
In children, the maximum recommended dose for infiltration analgesia (ilioinguinal-iliohypogastric block) is 1.25 mg/kg/side.
Route of Administration: For parenteral use.
Acute emergencies from local anesthetics are generally related to high plasma levels or high dermatomal levels ("high spinal") encountered during therapeutic use of local anesthetics or to unintended intrathecal or intravascular injection of local anesthetic solution.
Management of local anesthetic emergencies: The first consideration is prevention, best accomplished by incremental injection of levobupivacaine hydrochloride monohydrate, careful and constant monitoring of cardiovascular and respiratory vital signs and the patient's state of consciousness after each local anesthetic injection and during continuous infusion. At the first sign of change, oxygen should be administered, and further measures as warranted.
General contraindications related to regional anesthesia should be taken into account with the use of any regional anesthetic agent, including levobupivacaine. Levobupivacaine solutions are contraindicated in those with a known sensitivity to local anesthetic amide agents.
Levobupivacaine is contraindicated in patients with severe hypotension such as cardiogenic or hypovolemic shock (see Precautions).
Levobupivacaine is contraindicated for use in paracervical block in obstetrics, and for intravenous regional anesthesia (e.g., Bier's block).
Additionally, levobupivacaine 7.5 mg/ml solution should not be employed for any obstetric procedures due to an enhanced risk for cardiotoxic events based on experience with bupivacaine.
In performing levobupivacaine blocks, unintended intravenous injection is possible and may result in cardiac arrest (some cases fatal). Despite rapid detection and appropriate treatment, prolonged resuscitation may be required. The resuscitability relative to bupivacaine is unknown at this point in time as it has not been studied. As with all local anesthetics of the amide-type, levobupivacaine should be administered in incremental doses. Cases of severe bradycardia, hypotension, and respiratory compromise with cardiac arrest (some of them fatal), have been reported in conjunction with local anesthetics, including levobupivacaine. Since levobupivacaine should not be injected rapidly in large doses, it is not recommended for emergency situations, where a fast onset of surgical anesthesia is necessary.
Historically, pregnant patients were reported to have a high risk for cardiac arrhythmias, cardiac/circulatory arrest and death when bupivacaine was inadvertently rapidly injected intravenously. For Caesarean section, the 5 mg/ml (0.5%) levobupivacaine solution in doses up to 150 mg is recommended.
Local anesthetics should only be administered by clinicians who are well versed in the diagnosis and management of drug-related toxicity and other acute emergencies which might arise from the block being administered. The immediate availability of oxygen, other resuscitative drugs, cardiopulmonary resuscitative equipment, and the personnel resources needed for proper management of toxic reactions and related emergencies must be ensured. Delay in proper management of drug-related toxicity, underventilation from any cause, and/or altered sensitivity may lead to the development of acidosis, cardiac arrest, and possibly death.
When contemplating a peripheral nerve block, where large volumes of local anesthetic are needed, caution should be exercised when using the higher mg/ml concentrations of levobupivacaine.
The safe and effective use of local anesthetics depends on proper dosage, correct technique, adequate precautions, and readiness for emergencies.
Resuscitative equipment, oxygen, and resuscitative drugs should be available for immediate use (see Adverse Reactions). The lowest dosage that results in effective anesthesia should be used to avoid high plasma or dermatomal levels and serious adverse effects. Injections should be made slowly and incrementally, with frequent aspirations before and during the injection to avoid intravascular injection. When a continuous catheter technique is used, syringe aspirations should also be performed before and during each supplemental injection. During the administration of epidural anesthesia, it is recommended that a test dose of a local anesthetic with a fast onset be administered initially and that the patient be monitored for central nervous system and cardiovascular toxicity, as well as for signs of unintended intrathecal administration before proceeding. When clinical conditions permit, consideration should be given to employing local anesthetic solutions that contain epinephrine for the test dose because circulatory changes compatible with epinephrine may also serve as a warning sign of unintended intravascular injection. An intravascular injection is still possible even if aspirations for blood are negative.
Systemic adverse reactions following overdose for accidental intravascular injection reported with long acting local anesthetic agents involve both CNS and cardiovascular effects.
Levobupivacaine should be used with caution in conditions associated with impaired cardiovascular functions.
Injection of repeated doses of local anesthetics may cause significant increases in plasma levels with each repeated dose due to slow accumulation of the drug or its metabolites or to slow metabolic degradation. Tolerance to elevated blood levels varies with the physical condition of the patient. Local anesthetics should also be used with caution in patients with hypotension, hypovolemia, or impaired cardiovascular function, especially heart block.
Careful and constant monitoring of cardiovascular and respiratory vital signs (adequacy of ventilation) and the patient's state of consciousness should be performed after each local anesthectic injection. The clinician must be aware that restlessness, anxiety, incoherent speech, lightheadedness, numbness and tingling of the mouth and lips, metallic taste, tinnitus, dizziness, blurred vision, tremors, twitching, depression, or drowsiness may be early signs of central nervous system toxicity.
Amide-type local anesthetics, such as levobupivacaine, are metabolized by the liver, therefore, these drugs especially repeat doses, should be used cautiously in patients with hepatic disease. Patients with severe hepatic disease, because of their inability to metabolize local anesthetics normally, are at greater risk for developingtoxic plasma concentrations. Local anesthetics should also be used with caution in patients with impaired cardiovascular function as they may be less able to compensate for functional changes associated with prolonged A-V conduction caused by these drugs.
Many drugs used during the conduct of anesthesia are considered potential triggering agents for malignant hyperthermia. Amide-type local anesthetics are not known to trigger this reaction.
Epidural anesthesia: During epidural anesthesia, levobupivacaine should be administered in incremental volumes of three to five milliliters (3 to 5 ml), with sufficient time between doses to detect toxic manifestations of unintentional intravascular or intrathecal injection. Syringe aspirations should also be performed before and during each supplemental injection in continuous catheter techniques. An intravascular injection is still possible even if aspirations are negative. During the administration of epidural anesthesia, it is recommended that a test dose is administered initially and the effects monitored before the full dose is given. A test dose of a short-acting amide anesthetic, such as three milliliters (3 ml) of lidocaine, is recommended to detect unintentional intrathecal administration. This will be manifested within a few minutes by signs of a subarachnoid block (e.g., decreased sensation of the buttocks, paresis of the legs or, in the sedated patient, absent knee jerk). Unintentional intrathecal injection of local anesthetics can lead to very high spinal anesthesia, possibly apnea, severe hypotension and loss of consciousness. An intravascular or intrathecal injection is still possible, even if the results of the test dose are negative. The test dose itself may produce a systemic toxic reaction, extensive subarachnoid block, or cardiovascular effects.
Epidural analgesia: There have been postmarketing reports of cauda equina syndrome and events indicative of neurotoxicity temporally associated with the use of levobupivacaine for greater than or equal to 24 hours for epidural analgesia. These events were more severe and, in some cases, led to permanent sequelae when levobupivacaine was administered for greater than 24 hours. Therefore, the use of levobupivacaine is not recommended for more than 24 hours.
It is essential that aspiration for blood or cerebrospinal fluid (where applicable) be done prior to injecting any local anesthetic, both before the original dose and all subsequent doses, to avoid intravascular or intrathecal injection. However, a negative aspiration does not ensure against intravascular or intrathecal injection. Levobupivacaine should be used with caution in patients receiving other local anesthetics or agents structurally related to amide-type local anesthetics, since the toxic effects of these drugs are additive.
Use in head and neck area: Small doses of local anesthetics injected into the head and neck area may produce adverse reactions similar to systemic toxicity seen with unintentional intravascular injections of larger doses. The injection procedures require the utmost care. Confusion, convulsions, respiratory depression, and/or respiratory arrest and cardiovascular stimulation or depression have been reported. These reactions may be due to intra-arterial injection of the local anesthetic with retrograde flow to the cerebral circulation. Patients receiving these blocks should have their respirations and circulation monitored and be constantly observed. Resuscitative equipment and personnel for treating adverse reactions should be immediately available. Dosage recommendations should not be exceeded.
Information for the patient: When appropriate, patients should be informed in advance that they may experience temporary loss of sensation and motor activity in the anesthetized part of the body following correct administration of the regional anesthesia. Also, when appropriate, the physician should discuss other information including adverse reactions in the levobupivacaine package insert.
Effects on Ability to Drive and Use Machines: Levobupivacaine can have a major influence on the ability to drive or use machines. Patients should be warned not to drive or operate machinery until all the effects of the anesthesia and the immediate effects of surgery are passed.
Use in the Elderly: No overall differences in safety and effectiveness between geriatric patients and younger patients. Greater sensitivity of some older individuals cannot be rulled out.
Pregnancy: Levobupivacaine should only be used during pregnancy if the benefits outweigh the risks.
Labor and Delivery: Local anesthetics, including levobupivacaine, rapidly cross the placenta, and when used for epidural block, can cause varying degrees of maternal, fetal, and neonatal toxicity. The incidence and degree of toxicity depend upon the procedure performed, the type and amount of drug used, and the technique of drug administration. Adverse reactions in the parturient, fetus, and neonate involve alterations of the central nervous system, peripheral vascular tone, and cardiac function. Maternal hypotension, fetal bradycardia, and fetal decelerations have resulted from regional anesthesia with levobupivacaine for obstetrical pain relief. Local anesthetics produce vasodilation by blocking sympathetic nerves. Administration of intravenous fluids, elevation of the patient's legs and left uterine displacement will help prevent decreases in blood pressure. The fetal heart rate should also be monitored continuously and electronic fetal monitoring is highly advisable.
Lactation: Some local anesthetic drugs are excreted in breast milk and caution should be exercised when levobupivacaine is administered to a nursing woman. The excretion of levobupivacaine or its metabolites in human milk has not been studied.
Reactions to levobupivacaine are characteristic of those associated with other amide-type anesthetics. A major cause of the adverse effects to this group of drugs is associated with excessive plasma levels, or high dermatomal levels, which may be due to overdose, unintentional intravascular injection, or slow metabolic degradation. Systems involved may include the central nervous system, the cardiovascular system, and the respiratory system. (See Table 2.)
Click on icon to see table/diagram/image
Levobupivacaine should be used with caution in patients receiving other local anesthetics or agents structurally related to amide-type local anesthetics since the toxic effects of these drugs could be additive. CYP3A4 isoform and CYP1A2 isoform mediate the metabolism of levobupivacaine to desbutyl levobupivacaine and 3-hydroxy levobupivacaine, respectively. Thus, agents likely to be concomitantly administered with levobupivacaine that are metabolized by this isoenzyme family may potentially interact with levobupivacaine. It is likely that the metabolism of levobupivacaine may be affected by the known CYP3A4 inducers (such as phenytoin, phenobarbital, rifampin); CYP3A4 inhibitors (azole antimycotics, e.g., ketoconazole; certain protease inhibitors, e.g., ritonavir; macrolide antibiotics, e.g., erythromycin; and calcium channel antagonists, e.g. verapamil), CYP1A2 inducers (omeprazole) and CYP1A2 inhibitors (furafylline and clarithromycin). Dosage adjustments may be warranted when levobupivacaine hydrochloride monohydrate is concurrently administered with CYP3A4 inhibitors and CYP1A2 inhibitors, as systemic levobupivacaine levels may rise resulting in toxicity.
Levobupivacaine should be used with caution in patients receiving antiarrythmic agents with local anesthetic activity, e.g., mexiletine, or class III antiarrythmic agents since their use may be additive.
Unopened ampoules: Store at temperatures below 30°C.
After first opening: The product should be used immediately.
After dilution: After dilution in 0.9% sodium chloride solution, levobupivacaine hydrochloride monohydrate is physically and chemically stable at temperature 30°C for 7 days. Aseptic technique should be used to prepare the diluted products. Admixtures of levobupivacaine should be prepared for single patient use only. The unused portion of diluted levobupivacaine hydrochloride monohydrate should be discarded after each use. From a microbiological point of view, the product should be used immediately. If not used immediately, in-use storage times and conditions prior to use are the responsibility of the user and would normally not be longer than 24 hours at 2 to 8°C.
Shelf life: L-Ascain 5.0 mg/ml Injection can be used within 24 months from the date of manufacture is kept as recommended (see previously mentioned).
N01BB10 - levobupivacaine ; Belongs to the class of amides. Used as local anesthetics.
L-Ascain soln for inj 5 mg/mL
10 mL x 5 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image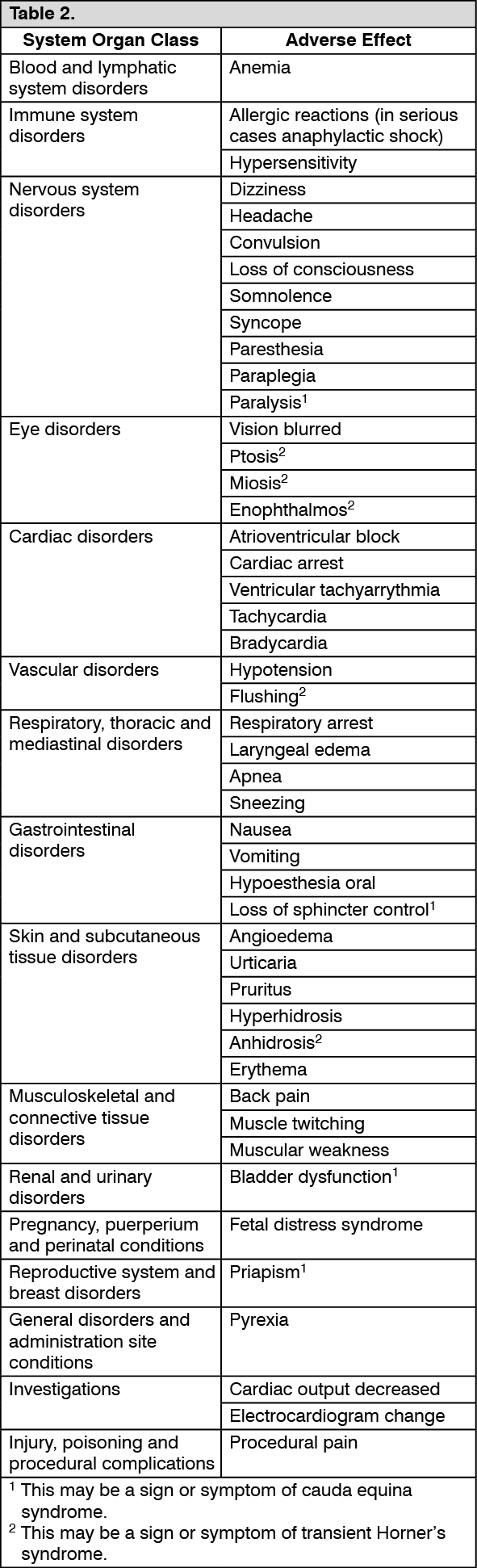 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
