25 mg tablet: Each film-coated tablet contains quetiapine fumarate equivalent to quetiapine 25 mg.
100 mg tablet: Each film-coated tablet contains quetiapine fumarate equivalent to quetiapine 100 mg.
200 mg tablet: Each film-coated tablet contains quetiapine fumarate equivalent to quetiapine 200 mg.
Pharmacotherapeutic group: Diazepines, oxazepines and thiazepines. ATC code: N05A H04.
Pharmacology: Pharmacodynamics: Mechanism of action: Quetiapine is an atypical antipsychotic agent which interacts with a broad range of neurotransmitter receptors. Quetiapine exhibits affinity for brain serotonin (5HT2) and dopamine D1- and D2- receptors. It is this combination of receptor antagonism with a higher selectivity for 5HT2 relative to D2- receptors, which is believed to contribute to the antipsychotic properties and low extrapyramidal side effects (EPS) liability of quetiapine. Quetiapine also has high affinity at histaminergic and adrenergic α1- receptors, with a lower affinity at adrenergic α2- receptors, but no appreciable affinity at cholinergic muscarinic or benzodiazepine receptors.
Quetiapine is active in tests for antipsychotic activity, such as conditioned avoidance. It also blocks the action of dopamine agonists, measured either behaviourally or electrophysiologically, and elevates dopamine metabolite concentrations, a neurochemical index of D2- receptor blockage.
Pharmacodynamic effects: Unlike standard antipsychotics, quetiapine has an atypical profile. Quetiapine does not produce dopamine D2- receptor supersensitivity after chronic administration. Quetiapine produces only weak catalepsy at effective dopamine D2- receptor blocking doses. Quetiapine demonstrates selectivity for the limbic system by producing depolarisation blockade of the mesolimbic but not the nigrostriatal dopamine-containing neurones following chronic administration. Quetiapine exhibits minimal dystonic liability in haloperidol-sensitised or drug-naïve Cebus monkeys after acute and chronic administration. Quetiapine shows minimal EPS liability, and it has been hypothesised that agents with a lower EPS liability may also have a lower liability to produce tardive dyskinesia (see Adverse Reactions).
Clinical Efficacy: Lack of induction of EPS is considered a feature of atypical antipsychotics. Unlike many other antipsychotics, quetiapine does not produce sustained elevations in prolactin, which is considered a feature of atypical antipsychotics. In the treatment of moderate to severe manic episodes, quetiapine demonstrated efficacy in reduction of manic symptoms at 3 and 12 weeks. Use of quetiapine in combination with divalproex or lithium in moderate have been found to be well-tolerated in moderate to severe manic episodes.
Quetiapine is effective when given twice a day, although it has a pharmacokinetic half-life of approximately 7 hours. This is further supported by the data from a positron emission tomography (PET) study which identified that for quetiapine, 5HT2- and D2- receptor occupancy are maintained for up to 12 hours. The safety and efficacy of doses greater than 800 mg/day have not been established.
The long-term efficacy of quetiapine in prevention of relapses has not been verified. In patients with schizophrenia, quetiapine was effective in maintaining the clinical improvement during continuation therapy in those who showed an initial treatment response, suggesting some long-term efficacy.
Pharmacokinetics: Quetiapine is well absorbed and extensively metabolised following oral administration. The principal human plasma metabolites do not have significant pharmacological activity.
The bioavailability of quetiapine is not significantly affected by administration with food. The elimination half-life of quetiapine is approximately 7 hours. Quetiapine is approximately 83% bound to plasma proteins. The pharmacokinetics of quetiapine are linear, and do not differ between men and women.
The mean clearance of quetiapine in the elderly is approximately 30 to 50% lower than that seen in adults aged 18 to 65 years.
The mean plasma clearance of quetiapine was reduced by approximately 25% in subjects with severe renal impairment (creatinine clearance less than 30 ml/min/1.73m2), but the individual clearance values are within the range for normal subjects.
Quetiapine is extensively metabolized in the liver, with parent compound accounting for less than 5% of unchanged drug-related material in the urine or faeces, following the administration of radiolabelled quetiapine. Approximately 73% of the radioactivity is excreted in the urine and 21% in the faeces. The mean quetiapine plasma clearance decreases with approx. 25% in persons with known hepatic impairment (stable alcoholic cirrhosis). As quetiapine is extensively metabolized in the liver, elevated plasma levels are expected in the population with hepatic impairment. Dose adjustments may be necessary in these patients (see Dosage & Administration).
CYP3A4 is the primary enzyme responsible for cytochrome P450 mediated metabolism of quetiapine.
Quetiapine and several of its metabolites were found to be weak inhibitors of human cytochrome P450 1A2, 2C9, 2C19, 2D6 and 3A4 activities, but only at concentrations at least 10- to 50-fold higher than those observed in the usual effective dose range of 300 to 450 mg/day in humans. Based on this, it is unlikely that co-administration of quetiapine with other drugs will result in clinically significant drug inhibition of cytochrome P450 mediated metabolism of the other drug. From animal studies it appears that quetiapine can induce cytochrome P450 enzymes. In a specific interaction study in psychotic patients, however, no increase in the cytochrome P450 activity was found after administration of quetiapine.
Treatment of schizophrenia.
Treatment of acute manic episodes associated with bipolar 1 disorder, as either monotherapy or adjunct to lithium or divalproex.
Ketipinor can be administered with or without food.
Usual dose: Ketipinor should generally be administered with an initial dose of 25 mg twice daily, with increases in increments of 25 - 50 mg twice or thrice daily on the 2nd and 3rd day, as tolerated, to a target range of 300 - 400 mg daily by the 4th day, given twice or thrice daily.
Further dosage adjustments, if indicated, should generally occur at intervals of not less than 2 days, as steady state for Ketipinor would not be achieved for approximately 1 - 2 days in the typical patient. When dosage adjustments are necessary, dose increments/decrements of 25 - 50 mg twice daily are recommended.
Antipsychotic efficacy was demonstrated in a dose range of 150 - 750 mg/day. Although it has been reported that doses more than 300 mg/day were not more efficacious than 300 mg/day dose, in some cases, doses in the range of 400 - 500 mg/day appeared to be needed. The safety of doses more than 800 mg/day has not been established.
Maintenance treatment: While the effectiveness of long term use of quetiapine has not been clearly demonstrated, the effectiveness of maintenance treatment is well established for many other antipsychotic drugs. It is recommended that responding patients be continued on Ketipinor at the lowest dose needed to maintain remission. Patients should be periodically reassessed for efficacy and the need for maintenance treatment.
Reinitiation of treatment in patients previous discontinued: It is recommended that when restarting patients who had stopped therapy with Ketipinor for less than 1 week, initiation with Ketipinor is not required and the maintenance dose may be reinitiated. However, for patients who have been off Ketipinor for more than 1 week, the initiation titration schedule should be followed.
Acute Manic Episodes Associated with Bipolar Disorder: As monotherapy or as adjunct therapy to mood stabilizers (lithium or divalproex), total daily dose for the first 4 days of therapy is 100 mg (Day 1), 200 mg (Day 2), 300 mg (Day 3) and 400 mg (Day 4). Further dosage adjustment up to 800 mg/day by Day 6 should be in increments of no more than 200 mg/day. Depending on the clinical response and tolerability of the individual patient, the dose may be adjusted within the range of 200 - 800 mg/day. The usual effective dose range is 400 - 800 mg/day.
Children and adolescents: The safety and efficacy of quetiapine have not been evaluated in children and adolescents.
Elderly: As with other antipsychotics, Ketipinor should be used with caution in the elderly, especially during the initial dosing period. Elderly patients should be started on Ketipinor 25 mg/day. The dose should be increased daily, in increments of 25 - 50 mg to an effective dose, which is likely to be lower than in younger patients.
Note: the mean plasma clearance of quetiapine was reduced by 30-50% in elderly subjects when compared to younger patients.
Renal and Hepatic Impairment: The oral clearance of quetiapine is reduced by approximately 25 % in patients with renal or hepatic impairment. Quetiapine is extensively metabolized by the liver, and therefore should be used with caution in patients with known hepatic impairment.
Patients with renal or hepatic impairment should be started on Ketipinor 25 mg/day. The dosage should be increased daily with increments of 25 to 50 mg/day until an effective dosage, depending on the clinical response and tolerability of the individual patient.
Experience with quetiapine in overdosage is limited. Estimated doses of quetiapine up to 20 g have been taken, without fatal consequences. Patients recovered without sequelae. There have been very rare reports of overdose of quetiapine alone resulting in death or coma, or QT-interval prolongation.
In general, reported signs and symptoms were those resulting from an exaggeration of the drug’s known pharmacological effects, i.e., drowsiness and sedation, tachycardia and hypotension.
There is no specific antidote to quetiapine. In cases of severe signs, the possibility of multiple drug involvement should be considered, and intensive care procedures are recommended, including establishing and maintaining a patent airway, ensuring adequate oxygenation and ventilation, and monitoring and support of the cardiovascular system. Whilst the prevention of absorption in overdose has not been investigated, gastric lavage (after intubation, if patient is unconscious) and administration of activated charcoal together with a laxative should be considered.
Close medical supervision and monitoring should be continued until the patient recovers.
Hypersensitivity to the active substance or to any of the excipients of the product.
Concomitant administration of cytochrome P450 3A4 inhibitors, such as HIV-protease inhibitors, azole-antifungal agents, erythromycin, clarithromycin and nefazodone (see also Interactions).
Cardiovascular: Ketipinor should be used with caution in patients with known cardiovascular disease or family history of QT prolongation, cerebrovascular disease, or other conditions predisposing to hypotension. Ketipinor may induce orthostatic hypotension, especially during the initial dose-titration period and therefore dose reduction or more gradual-titration should be considered if this occurs.
Seizures: As with other antipsychotics, caution is recommended when treating patients with a history of seizures.
Extrapyramidal symptoms: Clinical experience thus far indicates that the incidence of extrapyramidal symptoms was no different from that of placebo across the recommended therapeutic dose range.
Tardive dyskinesia: If signs and symptoms of tardive dyskinesia appear, dose reduction or discontinuation of Ketipinor should be considered (see Adverse Reactions).
Neuroleptic malignant syndrome: Neuroleptic malignant syndrome has been associated with antipsychotic treatment, including quetiapine (see also Adverse Reactions). Clinical manifestations include hyperthermia, altered mental status, muscular rigidity, autonomic instability, and increased creatine phosphokinase. In such an event, Ketipinor should be discontinued and appropriate medical treatment given.
Acute withdrawal reactions: Acute withdrawal symptoms including nausea, vomiting and insomnia have very rarely been described after abrupt cessation of high doses of antipsychotic drugs. Recurrence of psychotic symptoms may also occur, and the emergence of involuntary movement disorders (such as akathisia, dystonia and dyskinesia) has been reported. Therefore, gradual withdrawal is advisable.
Elderly patients with dementia-related psychosis: Quetiapine is not approved for the treatment of patients with dementia-related psychosis. Increased risk of cerebrovascular adverse events has been reported in the dementia population with some atypical antipsychotics. The mechanism for this increased risk is not known. An increased risk cannot be excluded for other antipsychotics or other patient populations. Ketipinor should be used with caution in patients with risk factors for stroke.
It has also been reported that elderly patients with dementia-related psychosis are at increased risk of death when treated with quetiapine although the causal relationship between quetiapine treatment and death in these elderly patients with dementia has not been established.
Interactions: See also Interactions.
Concomitant use of quetiapine with a strong hepatic enzyme inducer such as carbamazepine or phenytoin substantially decreases quetiapine plasma concentrations, which could affect the efficacy of quetiapine therapy. In patients receiving a hepatic enzyme inducer, initiation of Ketipinor treatment should only occur if the physician considers that the benefits of quetiapine outweigh the risks of removing the hepatic enzyme inducer. It is important that any change in the inducer is gradual, and if required, replaced with a non-inducer (e.g. sodium valproate).
Hyperglycemia and Diabetes Mellitus: Hyperglycemia in some cases, extreme, and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients treated with atypical antipsychotics. Assessment of the relationship between atypical antipsychotic use and glucose abnormalities is complicated by the possibility of an increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population. Given this confounders, the relationship between atypical antipsychotic use and hyperglycemiarelated adverse events is not completely understood. However, epidemiological studies suggest an increased risk of treatment-emergent hyperglycemia-related events in patients treated with the atypical antipsychotics. Precise risk estimates for hyperglycemia-related adverse events in patients treated with atypical antipsychotics are not available.
Patients with an established diagnosis of diabetes mellitus who are started on antipsychotics should be monitored regularly for worsening of glucose control. Patients with risk factors for diabetes mellitus (e.g., obesity, family history of diabetes) who are starting treatment with atypical antipsychotics should undergo fasting blood glucose testing at the beginning of treatment and periodically during treatment. Any patient treated with atypical antipsychotics should be monitored for symptoms of hyperglycemia including polydipsia, polyuria, polyphagia, and weakness. Patients who develop symptoms of hyperglycemia during treatment with atypical antipsychotics should undergo fasting blood glucose testing. In some cases, hyperglycemia has resolved when the atypical antipsychotic was discontinued; however, some patients required continuation of anti-diabetic treatment despite discontinuation of the suspect drug.
QT prolongation: QT prolongation has been observed in cases of overdose with quetiapine. As with other antipsychotics, caution should be exercised when quetiapine is prescribed with medicines known to increase the QTc interval, especially in the elderly, in patients with congenital long QT syndrome, congestive heart failure, heart hypertrophy, hypokalaemia and hypomagnesaemia. Concomitant use of quetiapine with other neuroleptics should be avoided.
Additional information: Use of quetiapine in combination with divalproex or lithium in moderate to severe manic episodes is limited; however, combination therapy was well tolerated (see Adverse Reactions and Pharmacology: Pharmacodynamics under Actions).
Ketipinor 100 mg and 200 mg tablets contain lactose monohydrate. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: Given its primary central nervous system effects, quetiapine may interfere with activities requiring mental alertness. Therefore, patients should be advised not to drive or operate machinery, until individual susceptibility to this is known.
Pregnancy: Neonates exposed to antipsychotic drugs during the third trimester of pregnancy are at risk for extrapyramidal and/or withdrawal symptoms following delivery. There have been reports of agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress, and feeding disorder in these neonates. These complications have varied in severity; while in some cases symptoms have been self-limited, in other cases neonates have required intensive care unit support and prolonged hospitalization.
Ketipinor should be used during pregnancy only if the potential benefit justifies the potential risk of the foetus.
Lactation: The degree to which quetiapine is excreted into human milk is unknown. Women who are breast-feeding should therefore be advised to avoid breast-feeding while taking Ketipinor.
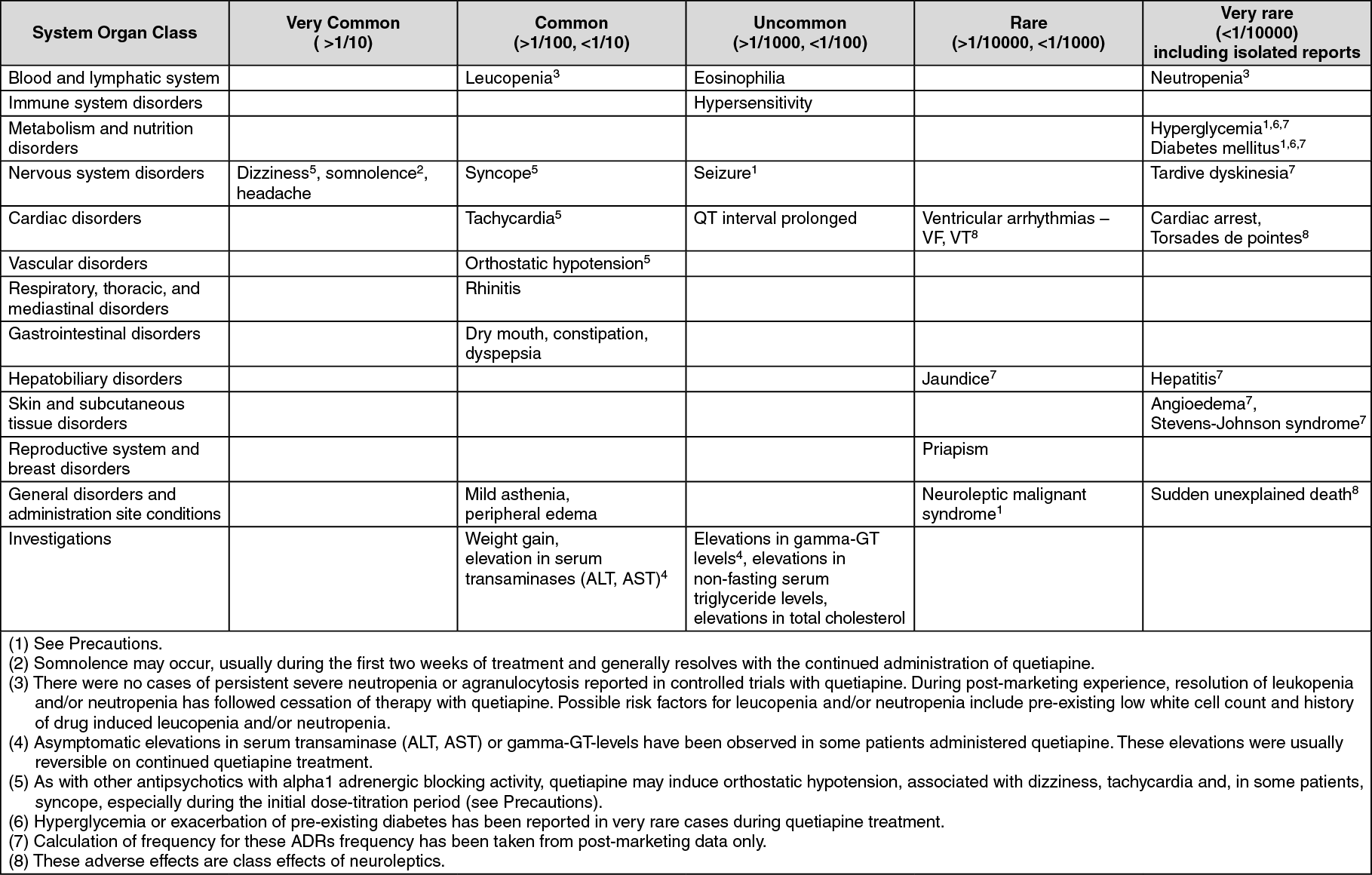
The most commonly reported Adverse Drug Reactions (ADRs) with quetiapine are somnolence, dizziness, dry mouth, mild asthenia, constipation, tachycardia, orthostatic hypotension, and dyspepsia.
As with other antipsychotics, weight gain, syncope, neuroleptic malignant syndrome, leucopenia, neutropenia and peripheral edema, have been associated with quetiapine.
The incidences of ADRs associated with quetiapine therapy are tabulated below according to the format recommended by the Council for International Organizations of Medical Sciences (CIOMS III Working Group; 1995).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Quetiapine treatment was associated with small dose-related decreases in thyroid hormone levels, particularly total T4 and free T4. The reduction in total and free T4 was maximal within the first two to four weeks of quetiapine treatment, with no further reduction during long-term treatment. In nearly all cases, cessation of quetiapine treatment was associated with a reversal of the effects on total and free T4, irrespective of the duration of treatment.
Smaller decreases in total T3 and reverse T3 were seen only at higher doses. Levels of TBG were unchanged and in general, reciprocal increases in TSH were not observed, with no indication that quetiapine causes clinically relevant hypothyroidism.
Given the primary central nervous system effects of quetiapine, Ketipinor should be used with caution in combination with other centrally acting drugs and alcohol.
Cytochrome P450 (CYP) 3A4 is the enzyme that is primarily responsible for the cytochrome P450 mediated metabolism of quetiapine. Concomitant administration of quetiapine (dosage of 25 mg) with ketoconazole, a CYP3A4 inhibitor, has been reported to cause a 5- to 8-fold increase in the AUC of quetiapine. On the basis of this, concomitant use of quetiapine with CYP3A4 inhibitors is contraindicated. It is also not recommended to take quetiapine together with grapefruit juice. As a consequence of this interaction, lower plasma concentrations can occur, which could affect the efficacy of quetiapine therapy.
Co-administration of quetiapine with phenytoin (another microsomal enzyme inducer) can cause a greatly increased clearance of quetiapine by approx. 450%.
In patients receiving a hepatic enzyme inducer, initiation of Ketipinor treatment should only occur if the physician considers that the benefits of quetiapine outweigh the risks of removing the hepatic enzyme inducer. It is important that any change in the inducer is gradual, and if required, replaced with a non-inducer (e.g. sodium valproate) (see also Precautions).
The pharmacokinetics of quetiapine were not significantly altered by co-administration of the antidepressants imipramine (a known CYP2D6 inhibitor) or fluoxetine (a known CYP3A4 and CYP2D6 inhibitor).
The pharmacokinetics of quetiapine were not significantly altered by co-administration of the antipsychotics risperidone or haloperidol. Concomitant use of quetiapine and thioridazine caused an increased clearance of quetiapine with approx. 70%.
The pharmacokinetics of quetiapine were not altered when co-administered with cimetidine.
The pharmacokinetics of lithium were not altered when co-administered with quetiapine.
The pharmacokinetics of sodium valproate and quetiapine were not altered to a clinically relevant extent during concomitant administration.
Formal interaction studies with commonly used cardiovascular drugs have not been performed.
As with other antipsychotics, caution should be exercised when quetiapine is prescribed with medicines known to increase the QTc interval (see also Precautions).
Caution should be exercised when quetiapine is prescribed with drugs causing electrolyte imbalance.
Incompatibilities: Not applicable.
Store below 30°C.
Shelf-life: 3 years.
N05AH04 - quetiapine ; Belongs to the class of diazepines, oxazepines and thiazepines antipsychotics.
Ketipinor FC tab 100 mg
3 × 10's
Ketipinor FC tab 200 mg
3 × 10's
Ketipinor FC tab 25 mg
10 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
