


 Sign Out
Sign Out




Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described in Precautions reflect exposure to IMFINZI in 1889 patients from the PACIFIC study (a randomized, placebo-controlled study that enrolled 475 patients with Stage III NSCLC), and Study 1108 (an open-label, single-arm, multicohort study that enrolled 970 patients with advanced solid tumours), and additional open-label, single-arm trial that enrolled 444 patients with metastatic lung cancer, indications for which durvalumab is not approved. In these trials, IMFINZI was administered at a dose of 10 mg/kg every 2 weeks. Among the 1889 patients, 38% were exposed for 6 months or more and 18% were exposed for 12 months or more. The data also reflects exposure to IMFINZI in combination with chemotherapy in 265 patients from the CASPIAN study (a randomized, open-label study in patients with ES-SCLC), in 338 patients from the TOPAZ-1 study (a randomized, double-blind study in patients with BTC). In the CASPIAN and TOPAZ-1 studies, IMFINZI was administered at a dose of 1500 mg every 3 or 4 weeks.
The data described in this section reflect exposure to IMFINZI in patients with Stage III NSCLC enrolled in the PACIFIC study and in patients with ES-SCLC enrolled in the CASPIAN study and in patients with BTC enrolled in the TOPAZ-1 study.
Non-Small Cell Lung Cancer: The safety of IMFINZI in patients with Stage III NSCLC who completed concurrent platinum-based chemoradiotherapy within 42 days prior to initiation of study drug was evaluated in the PACIFIC study, a multicenter, randomized, double-blind, placebo-controlled study. A total of 475 patients received IMFINZI 10 mg/kg intravenously every 2 weeks. The study excluded patients who had disease progression following chemoradiation, with active or prior autoimmune disease within 2 years of initiation of the study or with medical conditions that required systemic immunosuppression [see Pharmacology: Pharmacodynamics: Clinical Studies under Actions].
The study population characteristics were: median age of 64 years (range: 23 to 90), 45% age 65 years or older, 70% male, 69% White, 27% Asian, 75% former smoker, 16% current smoker, and 51% had WHO performance status of 1. All patients received definitive radiotherapy as per protocol, of which 92% received a total radiation dose of 54 Gy to 66 Gy. The median duration of exposure to IMFINZI was 10 months (range: 0.2 to 12.6).
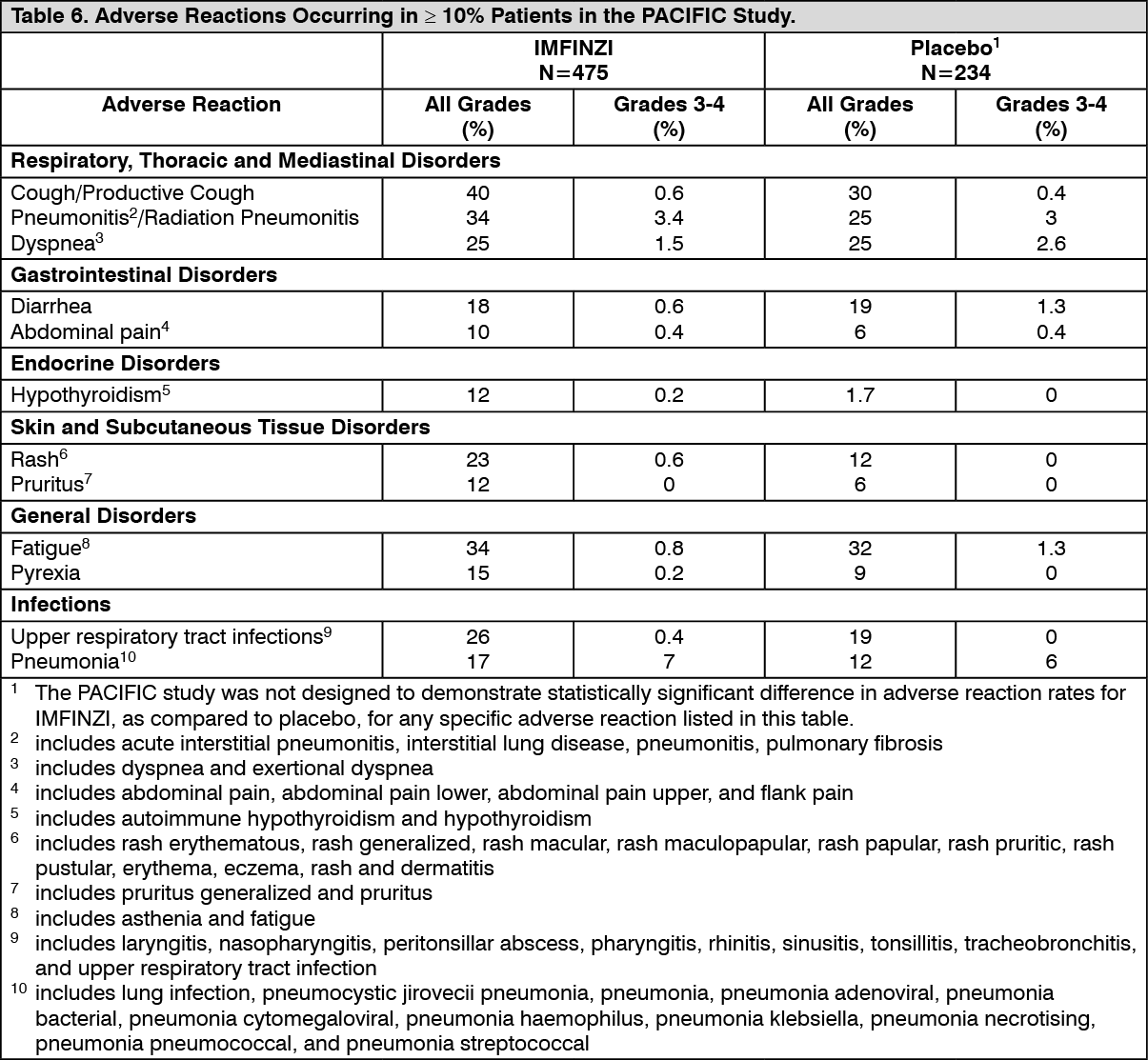
IMFINZI was discontinued due to adverse reactions in 15% of patients. The most common adverse reactions leading to IMFINZI discontinuation were pneumonitis or radiation pneumonitis in 6% of patients. Serious adverse reactions occurred in 29% of patients receiving IMFINZI. The most frequent serious adverse reactions reported in at least 2% of patients were pneumonitis or radiation pneumonitis (7%) and pneumonia (6%). Fatal pneumonitis or radiation pneumonitis and fatal pneumonia occurred in < 2% of patients and were similar across arms. The most common adverse reactions (occurring in ≥ 20% of patients) were cough, fatigue, pneumonitis or radiation pneumonitis, upper respiratory tract infections, dyspnea and rash.
Table 6 summarizes the adverse reactions that occurred in at least 10% of patients treated with IMFINZI. (See Table 6.)
 Click on icon to see table/diagram/image
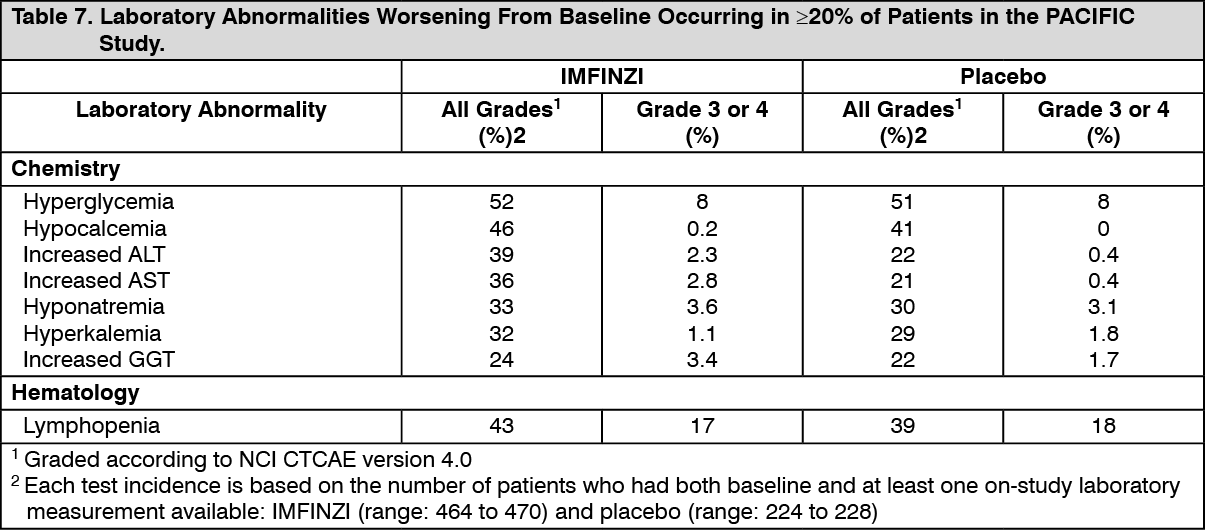
Click on icon to see table/diagram/imageOther adverse reactions occurring in less than 10% of patients treated with IMFINZI were dysphonia, dysuria, night sweats, peripheral edema, and increased susceptibility to infections. Table 7 summarizes the laboratory abnormalities that occurred in at least 20% of patients treated with IMFINZI. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSmall Cell Lung Cancer: The safety of IMFINZI in combination with etoposide and either carboplatin or cisplatin in previously untreated ES-SCLC was evaluated in CASPIAN, a randomized, open-label, multicenter, active-controlled trial. A total of 265 patients received IMFINZI 1500 mg in combination with chemotherapy every 3 weeks for 4 cycles followed by IMFINZI 1500 mg every 4 weeks until disease progression or unacceptable toxicity. The trial excluded patients with active or prior autoimmune disease or with medical conditions that required systemic corticosteroids or immunosuppressants [see Pharmacology: Pharmacodynamics: Clinical Studies under Actions]. Among 265 patients receiving IMFINZI, 49% were exposed for 6 months or longer and 19% were exposed for 12 months or longer.
Among 266 patients receiving chemotherapy alone, 57% of the patients received 6 cycles of chemotherapy and 8% of the patients received PCI after chemotherapy.
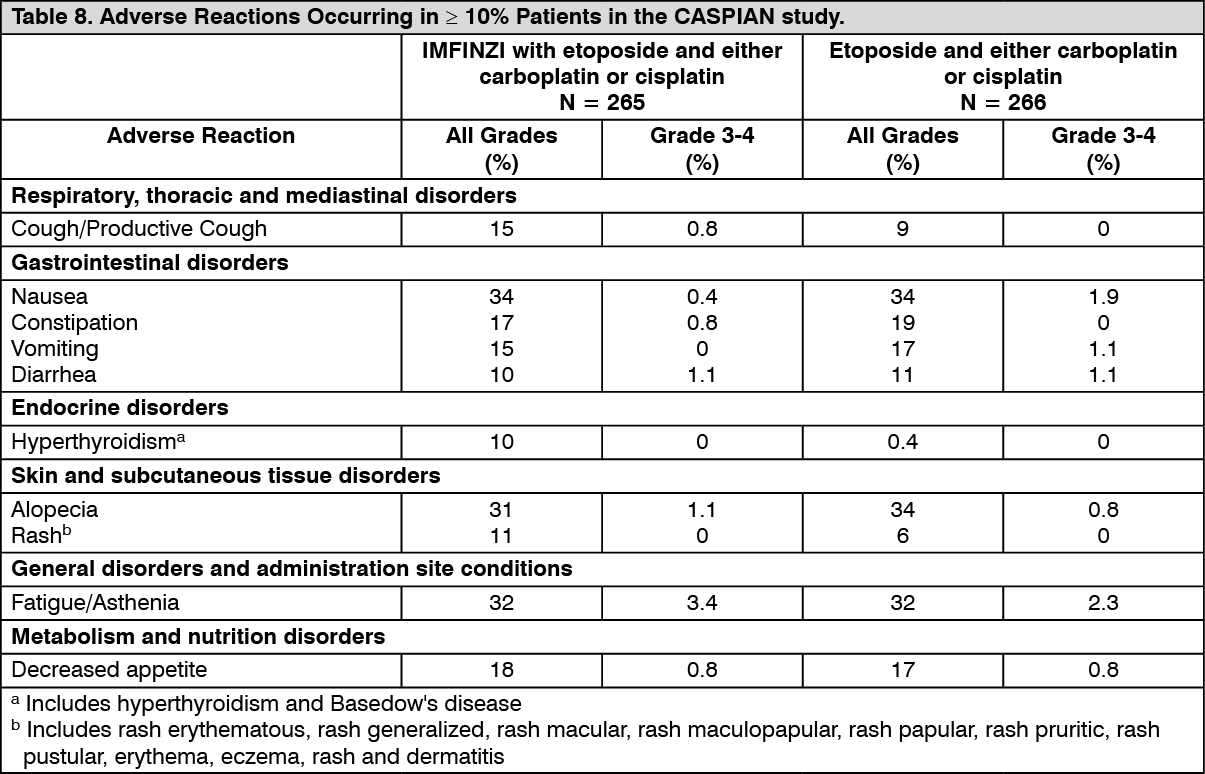
IMFINZI was discontinued due to adverse reactions in 7% of the patients receiving IMFINZI plus chemotherapy. These include pneumonitis, hepatotoxicity, neurotoxicity, sepsis, diabetic ketoacidosis and pancytopenia (1 patient each). Serious adverse reactions occurred in 31% of patients receiving IMFINZI plus chemotherapy. The most frequent serious adverse reactions reported in at least 1% of patients were febrile neutropenia (4.5%), pneumonia (2.3%), anemia (1.9%), pancytopenia (1.5%), pneumonitis (1.1%) and COPD (1.1%). Fatal adverse reactions occurred in 4.9% of patients receiving IMFINZI plus chemotherapy. These include pancytopenia, sepsis, septic shock, pulmonary artery thrombosis, pulmonary embolism, and hepatitis (1 patient each) and sudden death (2 patients). The most common adverse reactions (occurring in ≥ 20% of patients) were nausea, fatigue/asthenia and alopecia.
Table 8 summarizes the adverse reactions that occurred in patients treated with IMFINZI plus chemotherapy. (See Table 8.)
 Click on icon to see table/diagram/image
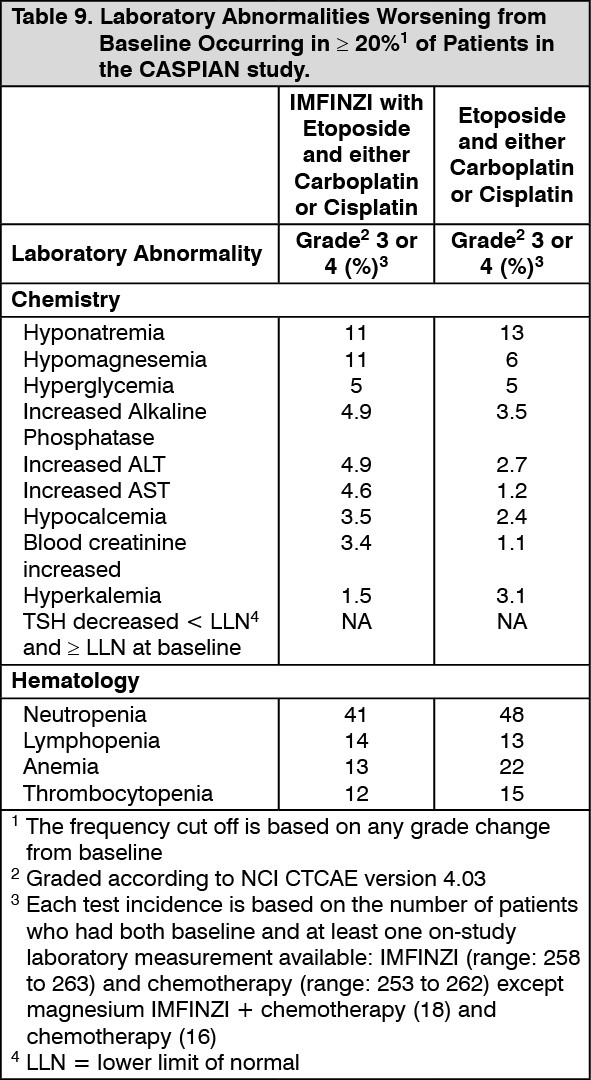
Click on icon to see table/diagram/imageTable 9 summarizes the laboratory abnormalities that occurred in at least 20% of patients treated with IMFINZI plus chemotherapy. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBiliary Tract Cancer: The safety of IMFINZI in combination with gemcitabine and cisplatin in locally advanced or metastatic BTC was evaluated in TOPAZ-1, a randomized, double-blind, placebo-controlled, multicenter trial. A total of 338 patients received IMFINZI 1,500 mg in combination with gemcitabine and cisplatin every 3 weeks up to 8 cycles followed by IMFINZI 1,500 mg every 4 weeks until disease progression or unacceptable toxicity. Patients with active or prior documented autoimmune or inflammatory disorders, HIV infection or other active infections, including tuberculosis or hepatitis C were ineligible [see Pharmacology: Clinical Studies under Actions].
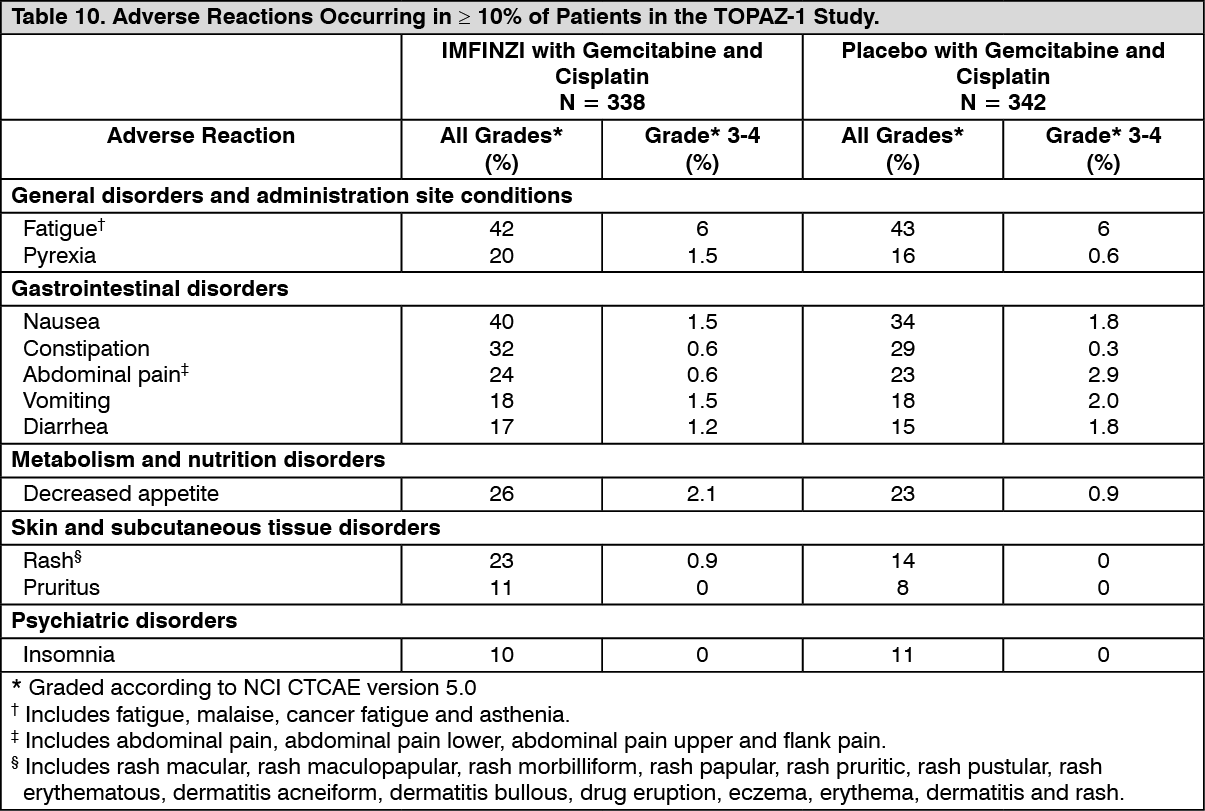
IMFINZI was discontinued due to adverse reactions in 6% of the patients receiving IMFINZI plus chemotherapy. The most frequently reported events resulting in discontinuation were sepsis (3 patients) and ischemic stroke (2 patients). The remaining events were dispersed across system organ classes and reported in 1 patient each. Serious adverse reactions occurred in 47% of patients receiving IMFINZI plus chemotherapy. The most frequent serious adverse reactions reported in at least 2% of patients were cholangitis (7%), pyrexia (3.8%), anemia (3.6%), sepsis (3.3%) and acute kidney injury (2.4%). Fatal adverse reactions occurred in 3.6% of patients receiving IMFINZI plus chemotherapy. These include ischemic or hemorrhagic stroke (4 patients), sepsis (2 patients), upper gastrointestinal hemorrhage (2 patients). The most common adverse reactions (occurring in ≥ 20% of patients) were fatigue, nausea, constipation, decreased appetite, abdominal pain, rash and pyrexia. Table 10 summarizes the adverse reactions that occurred in patients treated with IMFINZI plus chemotherapy. (See Table 10.)
 Click on icon to see table/diagram/image
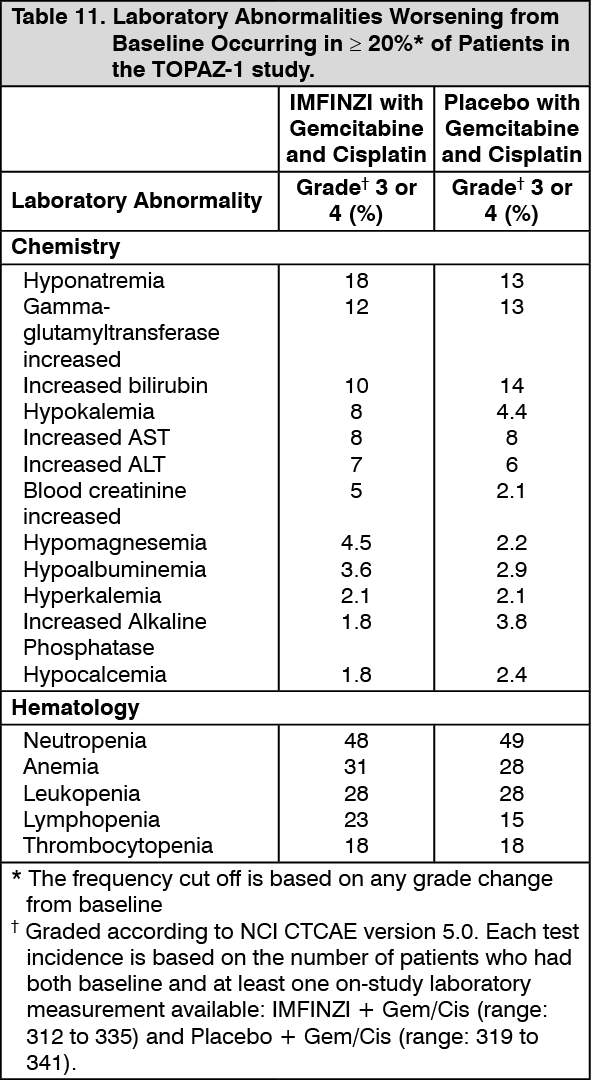
Click on icon to see table/diagram/imageTable 11 summarizes the laboratory abnormalities in patients treated with IMFINZI plus chemotherapy. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmunogenicity: As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to durvalumab to the incidence of antibodies to other products may be misleading.
Of 2280 patients who received IMFINZI 10 mg/kg every 2 weeks or 20 mg/kg every 4 weeks as a single-agent, 69 patients (3%) tested positive for treatment-emergent anti-drug antibodies (ADA) and 12 (0.5%) tested positive for neutralizing antibodies. The development of ADA against durvalumab appears to have no clinically relevant effect on its pharmacokinetics or safety profile.
Of 201 patients in the CASPIAN study who received IMFINZI 1500 mg every 3 weeks in combination with chemotherapy for four doses followed by IMFINZI 1500 mg every 4 weeks no patients tested positive for treatment-emergent ADA.
Of the 240 patients in the TOPAZ-1 study who received IMFINZI 1500 mg every 3 weeks in combination with chemotherapy up to 8 cycles followed by IMFINZI 1500 mg every 4 weeks, 2 (0.8%) patients tested positive for treatment emergent ADAs and neutralizing antibodies, respectively. There were insufficient numbers of patients with treatment-emergent ADAs or neutralizing antibodies (2 patients each) to determine whether ADAs have an impact on pharmacokinetics, pharmacodynamics, safety and/or effectiveness of IMFINZI.
View ADR Monitoring Form