Dexmedetomidine hydrochloride.
Each mL of solution for injection contains 118 micrograms of Dexmedetomidine HCl equivalent to 100 micrograms of Dexmedetomidine.
After dilution with 5% Dextrose, 0.9% NaCl, Ringer Lactate or 20% Mannitol infusion solution, the solution of product remain clear and colourless for 24 hours at temperature below 30°C.
Pharmacology: Pharmacodynamics: Dexmedetomidine is a selective alpha-2 receptor agonist with a broad range of pharmacological properties. It has a sympatholytic effect through the decrease of the release of noradrenaline in sympathetic nerve endings. The sedative effects are mediated through the decreased firing of locus coeruleus, the predominant noradrenergic nucleus, situated in the brainstem. Dexmedetomidine has analgesic and anaesthetic/ analgesic-sparing effects. The cardiovascular effects depend on the dose; with lower infusion rates the central effects dominate leading to decrease in heart rate and blood pressure. With higher doses, peripheral vasoconstriction effects prevail leading to an increase in systemic vascular resistance and blood pressure, while the bradycardic effect is further emphasised. Dexmedetomidine is relatively free from respiratory depressive effects when given as monotherapy to healthy subjects.
Dexmedetomidine was similar to midazolam and propofol on the time in target sedation range in a predominantly medical population requiring prolonged light to moderate sedation (RASS 0 to -3) in the ICU for up to 14 days, reduced the duration of mechanical ventilation compared to midazolam and reduced the time to extubation compared to midazolam and propofol. Compared to both propofol and midazolam, patients were more easily roused, more cooperative and better able to communicate whether or not they had pain. Dexmedetomidine treated patients had more frequent hypotension and bradycardia but less tachycardia than those receiving midazolam and more frequent tachycardia but similar hypotension to propofol-treated patients.
Pharmacokinetics: Distribution: Following IV administration, Icunes exhibits the following pharmacokinetic parameters: A rapid distribution phase with a distribution half-life (t½) of approximately 6 min; a terminal elimination t½ of approximately 2 hrs; and steady-state volume of distribution (Vss) approximately 118 L. Clearance is estimated to be approximately 39 L/hr. The mean body weight associated with this clearance estimate was 72 kg. Icunes exhibits linear kinetics in the dosage range of 0.2 - 0.7 mcg/kg/hr when administered by IV infusion for up to 24 hrs and it does not accumulate in treatments lasting up to 14 days. Dexmedetomidine is 94% bound to plasma proteins. Plasma protein binding is constant over the concentration range of 0.85 to 85 ng/ml. Dexmedetomidine binds to both human serum albumin and Alpha-1-acid glycoprotein with serum albumin as the major binding protein of dexmedetomidine in plasma.
Biotransformation and Elimination: Dexmedetomidine is eliminated by extensive metabolism in the liver. There are three types of initial metabolic reactions; direct N-glucuronidation, direct N-methylation and cytochrome P450 catalysed oxidation. The most abundant circulating dexmedetomidine metabolites are two isomeric N-glucuronides. Metabolite H-1, N-methyl 3-hydroxymethyl dexmedetomidine O-glucuronide, is also a major circulating product of dexmedetomidine biotransformation. Cytochrome P-450 catalyses the formation of two minor circulating metabolites, 3-hydroxymethyl dexmedetomidine produced by hydroxylation at the 3-methyl group of dexmedetomidine and H-3 produced by oxidation in the imidazole ring. Available data suggest that the formation of the oxidised metabolites is mediated by several CYP forms (CYP2A6, CYP1A2, CYP2E1, CYP2D6 and CYP2C19). These metabolites have negligible pharmacological activity.
Following IV administration of radiolabelled dexmedetomidine, an average 95% of the radioactivity was recovered in the urine and 4% in the faeces after nine days. The major urinary metabolites are the two isomeric N-glucuronides, which together accounted for approximately 34% of the dose and N-methyl 3-hydroxymethyl dexmedetomidine O-glucuronide that accounted for 14.51% of the dose. The minor metabolites dexmedetomidine carboxylic acid, 3-hydroxymethyl dexmedetomidine and its O-glucuronide individually comprised 1.11 to 7.66% of the dose. Less than 1% of unchanged parent drug was recovered in the urine. Approximately 28% of the urinary metabolites are unidentified minor metabolites.
Special Populations: No major pharmacokinetic differences have been observed based on gender or age. Dexmedetomidine plasma protein binding is decreased in patients with hepatic impairment. Patients with varying degrees of hepatic impairment (Child-Pugh Class A, B, or C) had decreased hepatic clearance of dexmedetomidine and prolonged plasma elimination t1/2. Although dexmedetomidine is administered to effect, it may be necessary to consider initial/maintenance dose reduction in patients with hepatic impairment depending on the degree of impairment and the response.
Icunes pharmacokinetics were not significantly different in patients with severe renal impairment [creatinine clearance (CrCl) <30 mL/min].
The pharmacokinetic profile of Icunes has not been studied in paediatric patients.
Intensive Care Unit Sedation: Dexmedetomidine hydrochloride is indicated for sedation of initially intubated and mechanically ventilated patients during treatment in an intensive care setting. Dexmedetomidine hydrochloride should be administered by continuous infusion not to exceed 24 hours.
Dexmedetomidine hydrochloride has been continuously infused in mechanically ventilated patients prior to extubation, during extubation, and post-extubation. It is not necessary to discontinue Dexmedetomidine hydrochloride prior to extubation.
Procedural Sedation: Dexmedetomidine hydrochloride is indicated for sedation of non-intubated patients prior to and/or during surgical and other procedures.
Recommended Dosage: Icunes dosing should be individualized and titrated to the desired clinical effect.
Icunes is not indicated for infusions lasting longer than 24 hr.
Icunes should be administered using a controlled infusion device.
Adults: Intensive Care Unit Sedation: A loading infusion of 1 mcg/kg over 10 min, followed by a maintenance infusion of 0.2-0.7 mcg/kg/hr. The rate of the maintenance infusion should be adjusted to achieve the desired level of sedation.
Procedural Sedation: A loading infusion of 1 mcg/kg over 10 min. For less invasive procedures e.g., ophthalmic surgery, a loading infusion of 0.5 mcg/kg given over 10 min may be suitable.
The maintenance infusion is generally initiated at 0.6 mcg/kg/hr and titrated to achieve desired clinical effect with doses ranging from 0.2-1 mcg/kg/hr. The rate of the maintenance infusion should be adjusted to achieve the targeted level of sedation.
Awake Fiberoptic Intubation Patients: A loading infusion of 1 mcg/kg over 10 min. A fixed maintenance infusion of 0.7 mcg/kg/hr is administered until the endotracheal tube is secured.
Hepatic and Renal Impairment: A dose reduction should be considered.
Elderly >65 Years: A loading infusion of 0.5 mcg/kg over 10 min. A dose reduction should be considered.
Dosage Adjustment: Due to possible pharmacodynamics interactions, a reduction in dosage of Icunes or other concomitant anaesthetics, sedatives, hypnotics or opioids may be required when co-administered.
Dosage reductions may need to be considered for patients with renal or hepatic impairment, and geriatric patients.
Method of administration: Icunes must be administered only as a diluted intravenous infusion using a controlled infusion device. For instructions on dilution of the medicinal product before administration, see Instruction for Use under Cautions for Usage.
Route of Administration: Intravenous Infusion.
The most common adverse reactions reported in conjunction with overdose included bradycardia, hypotension, over sedation, somnolence and cardiac arrest.
In cases of overdose with clinical symptoms, dexmedetomidine infusion should be reduced or stopped. Expected effects are primarily cardiovascular and should be treated as clinically indicated. At high concentration, hypertension may be more prominent than hypotension. Cases of sinus arrest reversed spontaneously or responded to treatment with atropine and glycopyrrolate. Resuscitation was required in isolated cases of severe overdose resulting in cardiac arrest.
Hypersensitivity to the active substance or to any of the excipients listed.
Advance heart block (grade 2 or 3) unless paced.
Uncontrolled hypotension.
Acute cerebrovascular conditions.
Monitoring: Dexmedetomidine injection is intended for use in an intensive care setting and use in other environments is not recommended. All patients should have continuous cardiac monitoring during Dexmedetomidine infusion. Respiration should be monitored in non-intubated patients due to the risk of respiratory depression and in some case apnoea.
General precautions: Since Dexmedetomidine injection should not be administered by loading or bolus dose, users should be ready to use an alternative sedative for acute control of agitation or during procedures, especially during the first few hours of treatment.
Some patients receiving Dexmedetomidine injection have been observed to be arousable and alert when stimulated. This alone should not be considered as evidence of lack of efficacy in the absence of other clinical signs and symptoms.
Dexmedetomidine injection should not be used as an induction agent for intubation or to provide sedation during muscle relaxant used. Dexmedetomidine lacks the anticonvulsant action of some other sedatives and so will not suppress underlying seizure activity.
Care should be taken if combining dexmedetomidine with other substances with sedative or cardiovascular actions as additive effects may occur.
Cardiovascular effects and precautions: Dexmedetomidine reduces heart rate and blood pressure through central sympatholysis but at higher concentrations causes peripheral vasoconstriction leading to hypertension.
Dexmedetomidine normally does not cause deep sedation and patients may be easily roused. Dexmedetomidine is therefore not suitable in patients who will not tolerate this profile of effects, for example, those requiring continuous deep sedation or with severe cardiovascular instability.
Caution should be exercised when administering dexmedetomidine to patients with pre-existing bradycardia. Data on the effects of Dexmedetomidine injection in patients with a heart rate <60 are very limited and particular care should be taken with such patients. Bradycardia does not normally require treatment but has commonly responded to anticholinergic medicine or dose reduction where needed. Patients with high physical fitness and slow resting heart rate may be particularly sensitive to bradycardic effects of alpha-2 receptor agonists and cases of transient sinus arrest have been reported.
The hypotensive effects of dexmedetomidine may be of greater significance in those patients with pre-existing hypotension (especially if not responsive to vasopressors), hypovolaemia, chronic hypotension or reduced functional reserve such as patients with severe ventricular dysfunction and the elderly and special care is warranted in these cases. Hypotension does not normally require specific treatment but, where needed, users should be ready to intervene with dose reduction, fluids and/or vasoconstrictors.
Patients with impaired peripheral autonomic activity (e.g. due to spinal cord injury) may have more pronounced haemodynamic changes after starting dexmedetomidine and so should be treated with care.
Transient hypertension has been observed primarily during the loading dose in association with the peripheral vasoconstrictive effects of dexmedetomidine and a loading dose is not recommended. Treatment of hypertension has generally not been necessary but decreasing the continuous infusion rate may be advisable.
Local vasoconstriction at higher concentration may be of greater significance in patients with ischaemic heart disease or severe cerebrovascular disease who should be monitored closely. Dose reduction or discontinuation should be considered in a patient developing sign of myocardial or cerebral ischaemia.
Patients with neurological disorders: Experience of dexmedetomidine in severe neurological disorders such as head injury and after neurosurgery is limited and it should be used with caution here, especially if deep sedation is required. Dexmedetomidine may reduce cerebral blood flow and intracranial pressure and this should be considered when selecting therapy.
Patients with hepatic impairment: Since Icunes clearance decreases with severity of hepatic impairment, dose reduction should be considered in patients with impaired hepatic function. Care should be taken in severe hepatic impairment as excessive dosing may increase the risk of adverse reactions, over-sedation or prolonged effect as a result of reduced dexmedetomidine clearance.
Other: Alpha-2 agonists have rarely been associated with withdrawal reactions when stopped abruptly after prolonged use. This possibility should be considered if the patient develops agitation and hypertension shortly after stopping dexmedetomidine.
It is not known whether dexmedetomidine is safe to use in malignant hyperthermia-sensitive individuals, therefore, it is not recommended. Dexmedetomidine injection treatment should be discontinued in the event of a sustained unexplained fever.
Effect on Ability to Drive and Use Machine: Patients should be advised to refrain from driving or other hazardous tasks for a suitable period of time after receiving Icunes for procedural sedation.
There are no or limited amount of data from the use of Icunes in pregnant women. Icunes is not recommended during pregnancy and in women of childbearing potential not using contraception.
It is not known whether Icunes is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when Icunes is administered to a nursing woman.
Summary of the safety profile: The most frequently reported adverse reactions with dexmedetomidine are hypotension, hypertension and bradycardia.
List of adverse reactions: Metabolism and nutrition disorders: Common: Hyperglycaemia, hypoglycaemia.
Uncommon: Metabolic acidosis, hypoalbuminaemia.
Psychiatric disorders: Common: Agitation.
Uncommon: Hallucination.
Cardiac disorders: Very common: Bradycardia*.
Common: Myocardial ischaemia or infarction, tachycardia.
Uncommon: Atrioventricular block first degree, cardiac output decreased.
Vascular disorders:Very Common: Hypotension*, hypertension*.
Respiratory, thoracic and mediastinal disorders: Common: Respiratory depression.
Uncommon: Dyspnoea, apnoea.
Gastrointestinal disorders: Common: Nausea, vomiting, dry mouth.
Uncommon: Abdominal distension.
General disorders and administration site conditions: Common: Withdrawal syndrome, hyperthermia.
Uncommon: Drug ineffective, thirst.
* See Description of selected adverse reactions as follows.
Description of selected adverse reactions: Clinically significant hypotension or bradycardia should be treated as described in Precautions.
Bradycardia has occasionally led to sinus arrest or pause. The symptoms responded to leg raising and anticholinergics such as atropine or glycopyrrolate. In isolated cases, bradycardia has progressed to periods of asystole in patients with pre-existing bradycardia.
Hypertension has been associated with the use of a loading dose and this reaction can be reduced by avoiding such a loading dose or reducing the infusion rate or size of the loading dose.
Interaction studies have only been performed in adults.
Co-administration of dexmedetomidine with anaesthetics, sedatives, hypnotics, and opioids is likely to lead to an enhancement of effects, including sedative, anaesthetic and cardiorespiratory effects. Specific studies have confirmed enhanced effects with isoflurane, propofol, alfentanil, and midazolam.
No pharmacokinetic interactions between dexmedetomidine and isoflurane, propofol, alfentanil and midazolam have been demonstrated. However, due to possible pharmacodynamic interactions, when co-administered with dexmedetomidine, a reduction in dosage of dexmedetomidine or the concomitant anaesthetic, sedative, hypnotic or opioid may be required.
Inhibition of CYP enzymes including CYP2B6 by dexmedetomidine has been studied in human liver microsome incubations. In vitro study suggests that interaction potential in vivo exists between dexmedetomidine and substrates with dominant CYP2B6 metabolism.
Induction of dexmedetomidine in vitro was observed on CYP1A2, CYP2B6, CYP2C8, CYP2C9 and CYP3A4, and induction in vivo cannot be excluded. The clinical significance is unknown.
The possibility of enhanced hypotensive and bradycardic effects should be considered in patients receiving other medicinal products causing these effects, for example, beta blockers, although additional effects in an interaction study with esmolol were modest.
Instruction for Use: Vials are intended for single patient use only.
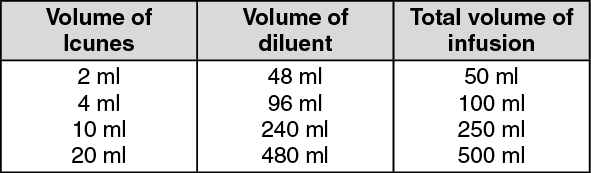
Preparation of solution: Dexmedetomidine 100 micrograms/ml Concentrate for Solution for Infusion can be diluted in glucose 50 mg/ml (5%), Ringers Lactate, mannitol or sodium chloride 9 mg/ml (0.9%) solution for injection to achieve the required concentration of 4 micrograms/ml prior to administration. Please see as follows in tabulated form the volumes needed to prepare the infusion.
In case the required concentration is 4 micrograms/ml: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The solution should be shaken gently to mix well.
Icunes should be inspected visually for particulate matter and discoloration prior to administration.
Icunes has been shown to be compatible when administered with the following intravenous fluids: 5% Dextrose, 0.9% NaCl, Ringer Lactate, and 20% Mannitol Infusion Solution.
Incompatibilities: Icunes must not be mixed with other medicinal products except these following intravenous fluids and medicinal products: 5% dextrose, 0.9% NaCl, Ringer Lactate, and 20% mannitol infusion solutions.
The mixed solution should be stored at a temperature not exceeding 30°C and to be used within 24 hours of dilution.
Store at below 30°C.
After dilution: Store Icunes that has been diluted with 5% Dextrose, 0.9% NaCl, Ringer Lactate or 20% mannitol infusion solution at below 30°C for not more than 24 hours.
Shelf-Life: 24 months.
After dilution: The mixed solution should be stored at a temperature not exceeding 30°C and to be used within 24 hours of dilution.
N05CM18 - dexmedetomidine ; Belongs to the class of other hypnotics and sedatives.
Icunes infusion conc 100 mcg/mL
2 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
