Pharmacotherapeutic group: immune sera and immunoglobulins: immunoglobulins, normal human, for extravascular administration.
ATC code: J06BA01.
Pharmacology: Hizentra contains IgG with a broad spectrum of antibodies against infectious agents. It has a distribution of IgG subclasses closely proportional to that in native human plasma. The Fc and Fab functions of the IgG molecule are retained.
Hizentra is usually prepared from pooled human plasma from not less than 1,000 donors by a combination of cold ethanol fractionation, octanoic acid fractionation, combined with a filter aid-assisted depth filtration, and anion exchange chromatography.
Mechanism of action: This medicine supplies a broad spectrum of opsonizing and neutralizing IgG antibodies against a wide variety of bacterial and viral agents. In immunodeficiency, adequate doses of Hizentra may restore abnormally low IgG antibody levels to the normal range and thus help against infections.
The mechanism of action in CIDP is not fully understood, but may include immunomodulatory effects.
Pharmacodynamics effects: The safety and efficacy of Hizentra in patients with has been assessed in 7 phase III studies in patients with PID, 2 phase IV studies with PID, and 1 phase III study in patients with CIDP including 1 extension study.
PID: In the European pivotal prospective open label, single arm and multicentre study, a total of 51 subjects with primary immunodeficiency syndromes aged between 3 and 60 years old were treated with Hizentra for up to 41 weeks. The mean dose administered each week was 119 mg/kg body weight. Sustained IgG trough levels with mean concentrations of 7.99 - 8.25 g/l were thereby achieved throughout the treatment period. Subjects received in total 1831 weekly Hizentra infusions.
In the subsequent extension study a total of 40 patients treated previously in the pivotal study (age 4 to 52 years) were enrolled and treated up to 46 months under the same dosing. Patients received a total of 5405 weekly Hizentra infusions.
Over the entire treatment period constant IgG trough levels were achieved with average concentrations of 7.5 to 8.5 g/l, confirming the results of the pivotal study. The rate of acute serious bacterial infections (aSBI) was 0.0478 per patient per year, with an upper 99% confidence interval (CI) of 0.1252.
In the US prospective open label, single arm and multicentre study, a total of 49 subjects with primary immunodeficiency syndromes aged between 5 and 72 years old were treated with Hizentra for up to 15 months. The mean dose administered each week was 228 mg/kg body weight. Sustained IgG trough levels with a mean concentration of 12.53 g/l were thereby achieved throughout the treatment period. Subjects received in total 2264 weekly Hizentra infusions.
In the subsequent US extension study, a total of 21 previously treated patients (aged 5 to 69 years) were enrolled and treated up to 87 weeks at the same dosing. Patients received a total of 1735 weekly Hizentra infusions.
Over the entire treatment period constant IgG trough levels were achieved with average concentrations of 11.71 to 12.76 g/l (overall average 11.98 g/l), confirming the results of the pivotal study. In none of the patients treated the trough levels have been shown below 5 g/l during the treatment. The aSBI rate was 0.06 per patient per year, with an upper 99% confidence interval of 0.257.
To assess the safety and tolerability of higher infusion rates applied via the manual push and pump-assisted administration technique, 49 PID subjects aged 2 to 75 years were enrolled in an open-label, multicentre, parallel-arm, nonrandomised phase IV study and treated with Hizentra for at least 12 weeks (11 paediatric patients aged 2 to <18, 35 adult patients aged 18 to 65, and 3 geriatric patients aged >65 years). In the patient group (n=16) receiving Hizentra via the manual push technique (manual push flow rate cohort), 2 to 7 infusions per week were administered with the flow rates of 30, 60 and 120 ml/hour/site corresponding to 0.5 ml/min, 1.0 ml/min or 2.0 ml/min per site. In the patient group (n=18) receiving Hizentra via pump-assisted administration (pump-assisted flow rate cohort), weekly Hizentra infusions were administered with 25, 50, 75 and 100 ml/hour/site flow rate. In addition, higher infusion volumes of 25, 40 and 50ml per site (pump-assisted volume cohort) were evaluated in pump-assisted administration of weekly Hizentra doses (n=15). In all three groups, each infusion parameter was used for 4 weeks, after which tolerating subjects could switch to the next higher infusion parameter.
Overall, the tolerability* was ≥ 0.98 for all infusion parameter levels in all cohorts. The percentage of subjects responding to a higher infusion parameter (= responder**) was: in the manual push flow rate cohort 100.0% at the 30 ml/hour and 60 ml/hour, and 87.5% at the 120 ml/hour per site; in the pump-assisted flow rate cohort 77.8% at the 25 ml/hour and the 50 ml/hour, 66.7% at the 75 ml/hour, and 61.1% at the 100 ml/hour per site; in the pump-assisted volume cohort 86.7% at the 25 ml and 73.3% at the 40 ml and 50 ml per site. No clinically relevant differences in the serum IgG trough concentrations were observed between the baseline at day 1 and at the end of the study in all subjects.
* Tolerability: number of infusions without severe local reactions divided by the total number of infusions.
** Responder: in the pump-assisted group a subject who performed ≥3 valid infusions out of 4 for an infusion parameter; in the manual push group a subject who performed ≥60 % of valid infusions for an infusion parameter. An infusion was considered valid, if ≥95 % of the planned flow rate/volume per ≥1 infusion site was achieved.
Paediatric population: The safety and effectiveness of Hizentra have been established in paediatric subjects 2 to 18 years of age.
Hizentra was evaluated in 68 paediatric subjects with PID 2 to <12 years of age and in 57 paediatric subjects 12 to <18 years of age. There were no differences in the pharmacokinetics, safety and efficacy profiles as compared with adult subjects. No paediatric-specific dose adjustments were necessary to achieve the desired serum IgG levels. No differences were seen in the pharmacodynamic properties between adult and paediatric study patients.
Geriatric population: No overall differences in safety or efficacy were observed between PID subjects >65 years and PID subjects 18 to 65 years of age. In the clinical studies Hizentra was evaluated in 13 patients with PID >65 years of age.
CIDP: The safety, efficacy and tolerability of Hizentra in patients with CIDP has been assessed in a multicentre, double-blind, randomised, placebo-controlled, parallel-group phase III PATH [Polyneuropathy and Treatment with Hizentra] study. 172 subjects previously treated with IVIg were randomised to weekly 0.2 g/kg bw Hizentra, weekly 0.4 g/kg bw Hizentra or placebo groups, and followed for a subsequent 24 weeks. The mean duration of exposure was 118.9 days in the 0.2 g/kg bw and 129 days in the 0.4 g/kg bw Hizentra group (maximum exposure up to 167 and 166 days in each group, respectively). Subjects generally used 4 infusion sites in parallel (up to 8 sites in parallel). In total, 57 subjects received 1514 infusions in the placebo group, 57 subjects received 2007 infusions in the 0.2 g/kg bw Hizentra group, and 58 subjects received 2218 infusions in the 0.4 g/kg bw Hizentra group (in total 5739 infusions).
The primary efficacy endpoint was the percentage of subjects who had a CIDP relapse (defined as a ≥ 1 point increase in adjusted Inflammatory Neuropathy Cause and Treatment [INCAT] score compared with baseline) or were withdrawn for any other reason in the Hizentra treatment period.
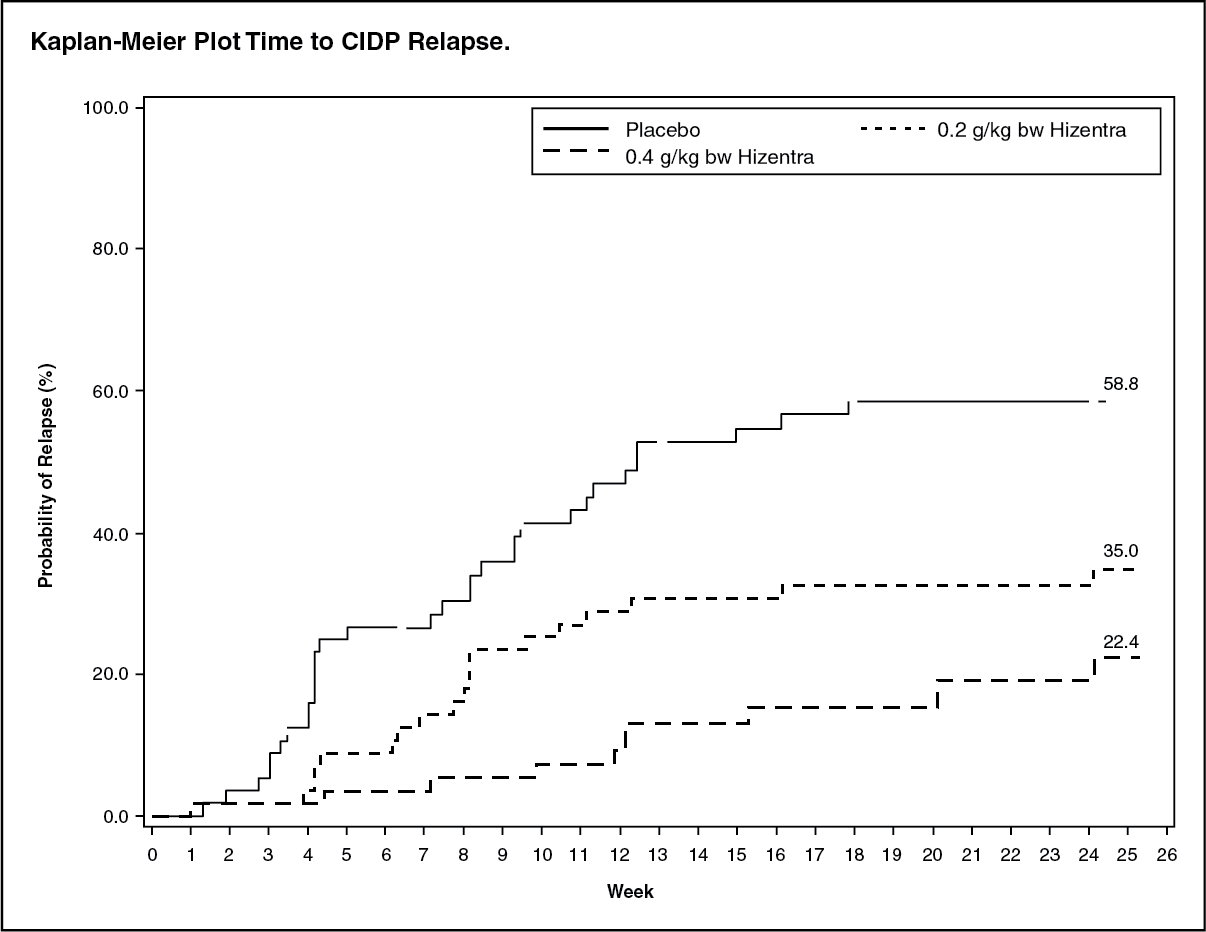
Both Hizentra doses demonstrated superiority over placebo for the primary endpoint. A statistically significant lower percentage of subjects treated with Hizentra, 32.8 % for 0.4 g/kg bw and 38.6 % for 0.2 g/kg bw, had CIDP relapse or was withdrawn for other reasons compared with 63.2 % subjects treated with placebo (p < 0.001 or p = 0.007, respectively). When only considering relapse, the CIDP relapse rates were 19.0 % for 0.4 g/kg bw Hizentra and 33.3 % for 0.2 g/kg bw Hizentra compared with 56.1 % for placebo (p < 0.001 or p = 0.012, respectively). Accordingly, over the treatment period for up to 24 weeks Hizentra prevented relapse in 81 % and 67 % of subjects in the 0.4 g/kg bw and 0.2 g/kg bw group, respectively, while in the placebo group 44 % of subjects remained relapse-free.
Time to CIDP relapse (figure) was evaluated, and the corresponding probabilities for CIDP relapse based on Kaplan-Meier estimates were: placebo, 58.8 %; 0.2/kg bw Hizentra, 35.0 %; and 0.4 g/kg bw Hizentra, 22.4 %. The hazard ratios (95 % CI) for the lower dose and higher dose compared to placebo was 0.48 (0.27, 0.85) and 0.25 (0.12, 0.49), respectively.
The difference observed between the 0.2 g/kg bw and the 0.4 g/kg bw Hizentra groups did not reach statistical significance. (See figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the efficacy scores (INCAT score, mean grip strength, and Medical Research Council (MRC) sum score), subjects in both Hizentra dose groups remained stable while subjects in the placebo group deteriorated. Subjects in the high dose Hizentra group remained stable in the Rasch-built Overall Disability Scale (R-ODS) centile score. Subjects in both Hizentra dose groups remained stable in electrophysiology parameters.
A phase III, multicentre, 48-week open-label extension study enrolled 82 CIDP patients from the PATH study. The extension study investigated the long-term safety and efficacy of Hizentra maintenance therapy in the two weekly doses, 0.2 g/kg and 0.4 g/kg bw. Due to the study design, the same subject could receive both doses during the study; 72 subjects received doses of 0.4 g/kg and 73 subjects received doses of 0.2 g/kg during the efficacy evaluation period. The mean efficacy evaluation period was 125.8 days (range: 1-330) in the 0.2 g/kg, and 196.1 days (range: 1-330) in the 0.4 g/kg bw group. Patients who completed the pivotal PATH study without relapse on 0.4 g/kg bw dose and initially received this dose in the extension study had a relapse rate of 5.6 % (1/18 patients). For all patients who received 0.4 g/kg bw in the PATH extension study, 9.7 % (7/72 patients) had a relapse. Patients who completed the PATH study without relapse on 0.2 g/kg bw dose and initially received this dose in the extension study had a relapse rate of 50 % (3/6 patients). For all patients who received 0.2 g/kg bw in the extension study, 47.9 % (35/73 patients) had a relapse. Down-titrating patients in the extension study from 0.4 g/kg to 0.2 g/kg bw dose without occurrence of relapse was possible in 67.9 % of subjects (19/28 patients). All relapsers recovered within 4 weeks after treatment with 0.4 g/kg bw dose. Grip strength, MRC sum score, and R-ODS centile score remained stable as compared to baseline for patients who never had a relapse in the extension study.
Paediatric population: Hizentra was not evaluated in clinical studies in paediatric patients with CIDP who were under the age of 18.
Geriatric population: No overall differences in safety or efficacy were observed between CIDP subjects >65 years of age and subjects 18 to 65 years of age. In the clinical studies with CIDP patients, 61 subjects >65 years of age were treated with Hizentra.
Pharmacokinetics: Absorption and Distribution: Following subcutaneous administration of Hizentra, peak serum levels are achieved after approximately 2 to 3 days. The serum concentrations of total serum IgG, IgG subclasses, and specific IgGs are stable throughout the dosing interval.
Elimination: IgG and IgG-complexes are broken down in cells of the reticuloendothelial system.
PID: In a clinical phase III trial with Hizentra (n = 46), the subjects achieved sustained trough levels (median 8.1 g/l) over a period of 29 weeks when receiving median weekly doses of 0.06 to 0.24 g/kg bw. Simulations with population-pharmacokinetic models suggested that a comparable IgG exposure (C
max, AUC
0-14days, C
min, 14 days) is achieved when the double weekly Hizentra dose is administered every two weeks.
These simulations further suggested that a comparable IgG exposure is achieved when the weekly maintenance dose of Hizentra is divided in several doses (e.g. 2 times per week, 3 times per week, 5 times per week or daily).
If 2-3 daily doses were missed at continuous daily dosing, this resulted in simulations in a median serum IgG level decrease of about ≤ 4% compared to consistent daily dosing. By subsequent administration of the missed doses at the first day in addition to the daily dose, when daily dosing is resumed, the median concentration profile recovers within 2 to 3 days. However, if missed doses are not replaced when daily dosing is resumed, the steady-state IgG trough levels can be first achieved after a treatment time of up to 5-6 weeks.
Paediatric population: No differences were seen in the pharmacokinetic parameters between adult and paediatric PID study patients.
Geriatric population: No overall differences in the pharmacokinetic parameters were observed between PID subjects >65 years and subjects 18 to 65 years of age.
CIDP: In the PATH study, subjects (n = 172) achieved sustained trough levels over a period of 24 weeks when receiving weekly doses of 0.2 g/kg bw and 0.4 g/kg bw, respectively. The mean (SD) IgG trough concentration after Hizentra treatment in the 0.4 g/kg bw group was 20.4 (3.24) g/l and 15.4 (3.06) g/l in the 0.2 g/kg bw group. Simulations with population-pharmacokinetic models in the PATH study suggest that a comparable IgG exposure (C
max, AUC
0-14days, C
min, 14 days) is achieved when the double weekly Hizentra dose is administered every two weeks in the CIDP subjects. These simulations further suggest that a comparable IgG exposure is correspondingly achieved when the weekly maintenance dose of Hizentra is divided in several, more frequent doses (2 to 7 times per week) in the CIDP patients' population.
Paediatric population: Hizentra was not evaluated in clinical studies in paediatric patients with CIDP who were under the age of 18.
Geriatric population: No overall differences in the pharmacokinetic parameters were observed between CIDP subjects >65 years and subjects 18 to 65 years of age.
Toxicology: Preclinical data: Immunoglobulins are a normal constituent of the human body. L-proline is a physiological, non-essential amino acid.
The safety of Hizentra has been assessed in several preclinical studies, with particular reference to the excipient L-proline. Non-clinical data reveal no special risk for humans based on safety pharmacology and toxicity studies.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
