Intravenous drip infusion: HEAMOFER 20 must be diluted only in sterile 0.9% m/V sodium chloride solution: 100 mg iron (5 ml HEAMOFER 20) in maximum 100 ml sterile 0.9% m/V sodium chloride solution.
500 mg iron (25 ml HEAMOFER 20) in maximum 500 ml sterile 0.9% m/V sodium chloride solution.
For stability reasons, dilutions to lower HEAMOFER 20 concentrations are not permissible.
As infusion, maximum tolerated single dose per day given not more than once per week: Patients above 70 kg: 500 mg iron (25 ml HEAMOFER 20) in at least 3½ hours.
Patients of 70 kg and below: 7 mg iron/kg body weight in at least 3½ hours.
Dilution must take place immediately prior to infusion and the solution should be administered as follows: 100 mg iron (5 ml HEAMOFER 20) in at least 15 minutes.
200 mg iron (10 ml HEAMOFER 20) in at least 30 minutes.
300 mg iron (15 ml HEAMOFER 20) in at least 1½ hours.
400 mg iron (20 ml HEAMOFER 20) in at least 2½ hours.
Before administration of the therapeutic dose in a new patient the first 20 mg iron in adults and in children with a body weight greater than 14 kg and half the daily dose (1.5 mg iron/kg) in children with a body weight less than 14 kg should be infused over 15 minutes as a test dose. If no adverse reactions occur, the remaining portion of the infusion can be administered at recommended speed.
Intravenous injection: HEAMOFER 20 can be administered undiluted by slow intravenous injection as follows: 100 mg iron (5 ml HEAMOFER 20) in at least 5 minutes.
200 mg iron (10 ml HEAMOFER 20) in at least 10 minutes.
Before administration of the therapeutic dose in a new patient a test dose of 1 ml HEAMOFER 20 (20 mg iron) in adults and in children with a body weight greater than 14 kg and half the daily dose (1.5 mg iron/kg) in children with a body weight less than 14 kg should be injected over 1 to 2 minutes. If no adverse reactions occur within a waiting period of 15 minutes, the remaining portion of the injection can be administered at recommended speed.
Injection into dialyser: HEAMOFER 20 may be administered during a haemodialysis session directly into the venous limb of the dialyser under the same conditions as for intravenous injection.
Calculation of dosage: The total cumulative dose of HEAMOFER 20, equivalent to the total iron deficit (mg), is determined by the haemoglobin level and body weight. The dose of HEAMOFER 20 must be individually determined for each patient according to the total iron deficit calculated with the following formula: (See Equation 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Below 35 kg body weight: target Hb = 130 g/l and depot iron = 15 mg/kg body weight.
35 kg body weight and above: target Hb = 150 g/l and depot iron = 500 mg.
* Factor 0.24 = 0.0034 x 0.07 x 1000: Iron content of haemoglobin ≅ 0.34%.
Blood volume ≅ 7% of body weight.
Conversion from g/l to mg/l = Factor 1000.
(See Equation 2.)
Click on icon to see table/diagram/image
(See table.)
Click on icon to see table/diagram/image
To convert Hb (mM) to Hb (g/l), multiply the former by 16.1145.
If the total necessary dose exceeds the maximum allowed single dose, then the administration has to be split, please see section Administration.
Calculation of dosage for iron replacement secondary to blood loss and to support autologous blood donation: The required HEAMOFER 20 dose to compensate the iron deficit is calculated according the following formulas: If the quantity of blood lost is known: The administration of 200 mg i.v. iron (= 10 ml HEAMOFER 20) results in an increase in haemoglobin which is equivalent to 1 unit blood (= 400 ml with 150 g/l Hb content).
Iron to be replaced [mg] = number of blood units lost x 200 or Amount of HEAMOFER 20 needed [ml] = number of blood units lost x 10.
If the Hb level is reduced: Use the following formula considering that the depot iron does not need to be restored.
Iron to be replaced [mg] = body weight [kg] x 0.24 x (target Hb - actual Hb) [g/l].
e. g.: body weight 60 kg, Hb deficit = 10 g/l.
⇒ ≅150 mg iron to be replaced.
⇒ 7.5 ml HEAMOFER 20 needed.
Normal posology: Adults and the elderly: 5-10 ml HEAMOFER 20 (100-200 mg iron) one to three times a week depending on the haemoglobin level.
Children: There is limited data on children under study conditions. If there is a clinical need, it is recommended not to exceed 0.15 ml HEAMOFER 20 (3 mg iron) per kg body weight one to three times per week depending on the haemoglobin level.
Maximum tolerated dose: As injection, maximum tolerated dose per day, given not more than three times per week: 200 mg iron (10 ml HEAMOFER 20) injected over at least 10 minutes.
As infusion, maximum tolerated single dose per day given not more than once per week: Patients above 70 kg: 500 mg iron (25 ml HEAMOFER 20) in at least 3½ hours.
Patients of 70 kg and below: 7 mg iron/kg body weight in at least 3½ hours.
The maximum tolerated single dose is 7 mg iron per kg body weight given once per week, but not exceeding 500 mg iron. Administration time and dilution ratio see section Administration. The infusion times given in section administration. Must be strictly adhered to, even if the patient does not receive the maximum tolerated single dose.
Route of Administration: HEAMOFER 20 must only be administered by the intravenous route. This may be by a slow intravenous injection or by an intravenous drip infusion.
HEAMOFER 20 must not be used for intramuscular injection.
Before administration of the first therapeutic dose, a test dose should be given. If any allergic reactions or intolerance occurs during administration, the therapy must be stopped immediately.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image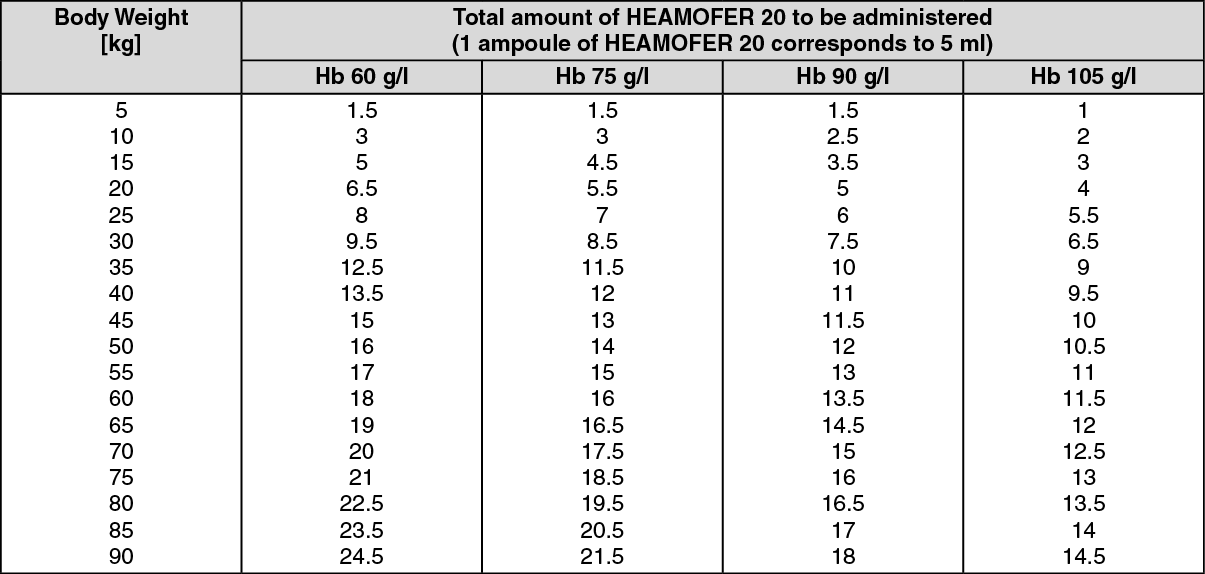 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
