


 Sign Out
Sign Out



Pharmacology: Pharmacodynamics: DYMISTA is a novel formulation of azelastine hydrochloride and fluticasone propionate. Therefore, the mechanisms of actions described as follows for the individual components apply to DYMISTA.
Azelastine hydrochloride, a phthalazinone derivative, is classified as a potent long-acting anti-allergic compound with selective H1-antagonist, mast cell stabilizing and anti- inflammatory properties. Data from in vivo (preclinical) and in vitro studies show that azelastine inhibits the synthesis or release of the chemical mediators known to be involved in early and late stage allergic reactions, e.g. leukotrienes, histamine, platelet-activating factor (PAF) and serotonin. The major metabolite, desmethylazelastine, also exhibits H1 - receptor antagonist activity. DYMISTA is administered as a racemic mixture. The racemate, R- and S- enantiomers were equally potent at inhibiting eyelid histamine-induced oedema in rats, however the R-enantiomer was 2-fold less active at inhibiting eyeball histamine-induced oedema.
Azelastine nasal spray has a faster onset of action than orally administered antihistamines and nasally administered corticosteroids. A relief of nasal allergic symptoms is observed within 15 minutes after administration.
Fluticasone propionate has potent anti-inflammatory activity but when used topically on the nasal mucosa at recommended doses has little or no detectable systemic activity.
Clinical Trials: The efficacy of DYMISTA was established in four randomised, double-blind, placebo- controlled studies in subjects with seasonal allergic rhinitis (SAR), namely MP4001, MP4002, MP4004, and MP4006.
Study MP4001 compared DYMISTA with commercial azelastine nasal spray (Astelin Nasal Spray) and commercial Fluticasone propionate Nasal Spray from Roxane Laboratories Inc available in the US at that time. Studies MP4002, MP4004, and MP4006 compared DYMISTA with the single compounds in the DYMISTA vehicle. All 4 trials had in common 4 treatment groups, the same regimen (1 spray per nostril twice daily), the same duration of treatment (2 weeks), and the same primary and almost the same secondary endpoints. These studies included male and female subjects 12 years of age or older with a minimum 2-year history of SAR.
During the study, nasal symptoms of itchy nose, nasal congestion, runny nose, sneezing, and ocular symptoms of itchy eyes, watery eyes, and eye redness were rated twice daily in a diary, using a 4-point scale from 0 (no symptoms) to 3 (severe symptoms). The scores were summed up to a total nasal symptom score (TNSS) and a total ocular symptom score (TOSS), respectively. In addition, postnasal drip was rated on the same 4-point scale. The Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) was completed by each subject 18 years of age or older, at the start and end of 14-day treatment (or early termination).
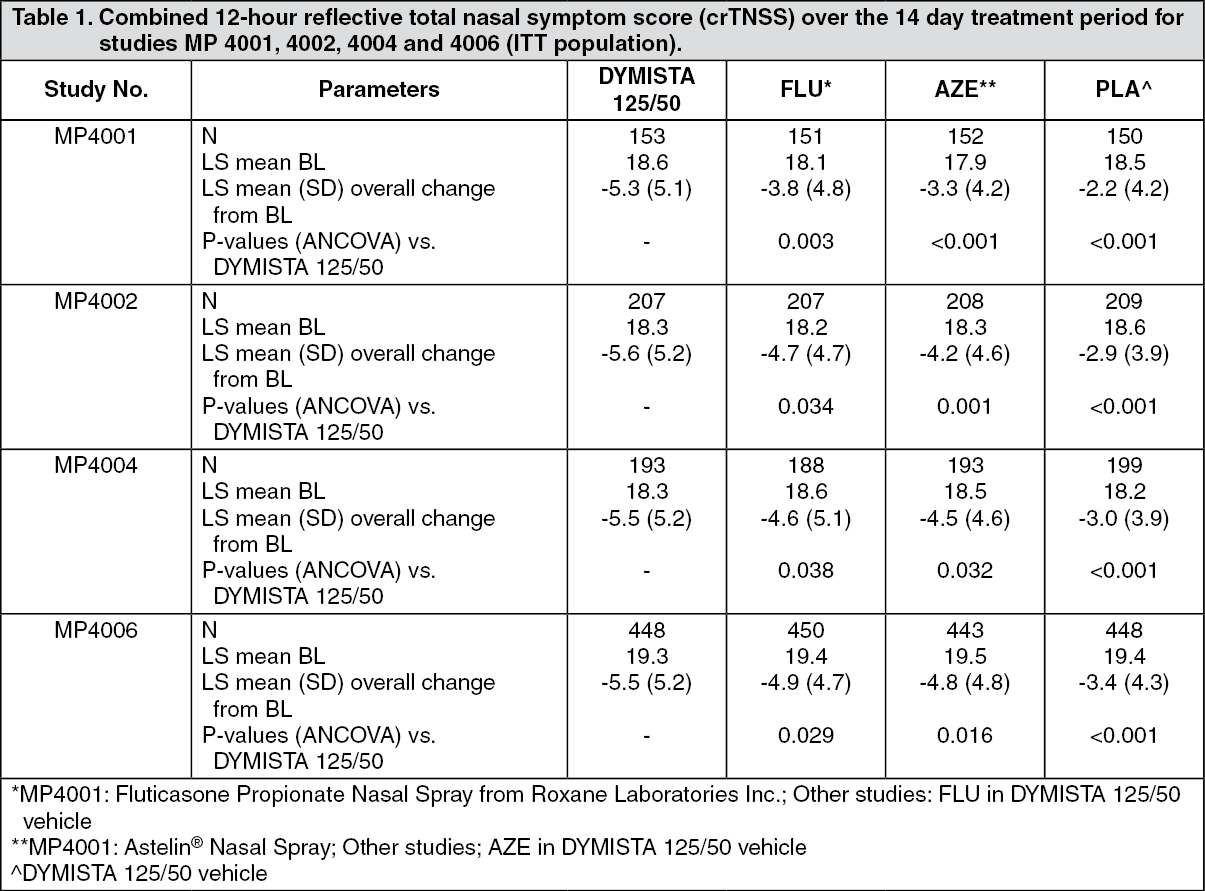
The primary efficacy endpoint for all four placebo-controlled studies was the change from baseline in the combined (i.e. AM and PM data added) 12-hour reflective total nasal symptom score (crTNSS) over the 14 day treatment period, tested primarily in the ITT set based on last observation. Secondary efficacy endpoints included the 12-hour AM and PM reflective TNSS, the instantaneous TNSS (iTNSS), the 12-hour reflective score for postnasal drip, the 12-hour reflective TOSS, the instantaneous TOSS, the 12-hour reflective and instantaneous individual nasal and ocular symptoms and the RQLQ score. In studies MP4002, MP4004 and MP4006, an attempt was made to evaluate the onset of action.
The pooled study population was primarily female (62.9%), white (80.3%) and between 18 and 65 years of age (87.3%).
Table 1 shows the primary efficacy results for the individual pivotal studies expressed as absolute change in crTNSS compared with placebo and all active treatments. Across the individual studies, DYMISTA was significantly superior to placebo and the monotherapy components. In addition, each individual component was significantly superior to placebo. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageData from studies MP4004 and MP4006 indicate that the onset of clinically relevant action for DYMISTA occurs within 30 minutes after first application of the combination.
In the meta-analysis that pooled data from the 4 efficacy studies, DYMISTA was shown to be statistically significantly superior to both azelastine and fluticasone monoproducts and all active treatments were statistically significantly superior to placebo for almost all secondary efficacy variables including the reflective TNSS confined to daytime (denominated as 12hr PM) or night time (12hr AM), the instantaneous TNSS, the reflective TOSS, post nasal drip, and all individual nasal and ocular symptom scores (all p<0.05) except the comparison DYMISTA with azelastine for eye redness (p=0.0513).
DYMISTA at least doubled the effect of azelastine and fluticasone propionate in reducing nasal and ocular symptoms score.
The RQLQ score for DYMISTA was significantly improved over placebo for overall score and for each individual RQLQ domain in each individual study and in the meta- analysis. Across all studies and in the meta-analysis, the treatment difference in overall score between DYMISTA and placebo exceeded the minimum clinically significant difference of -0.50.
Dymista provided substantial allergic rhinitis symptom relief (50% reduction in crTNSS) at least 3 days faster than azelastine and 6 days faster than fluticasone propionate nasal spray. The superior effect of DYMISTA to fluticasone propionate nasal spray was maintained throughout a one-year study in patients with chronic persistent allergic rhinitis and nonallergic/vasomotor rhinitis.
Pharmacokinetics: Two pharmacokinetic studies demonstrated that simultaneous intranasal administration of azelastine hydrochloride and fluticasone propionate with DYMISTA does not result in altered systemic absorption of either agent.
Absorption: After intranasal administration of two sprays per nostril (500 μg of azelastine and 200 μg of fluticasone propionate) of DYMISTA nasal spray, the mean (± standard deviation) peak plasma exposure (Cmax) was 194.5 ± 74.4 pg/mL for azelastine and 10.3±3.9 pg/mL for fluticasone and the mean total exposure (AUC) was 4217 ± 2618 pg/mL*hr for azelastine and 97.7 ± 43.1 pg/mL*hr for fluticasone. The median time to peak exposure (tmax) from a single dose was 0.5 hours for azelastine and 1.0 hours for fluticasone.
After intranasal administration, the systemic bioavailability of azelastine hydrochloride is approximately 40%. The absolute bioavailability of intranasal fluticasone at high doses (2,400 μg/day i.e. 12 times the recommended dose) is estimated as 1.26% (90% CI 0.85,1.86).
Distribution: After oral and intravenous administration of azelastine, the mean volume of distribution was 14.5 L/kg. In vitro studies with human plasma indicate that the plasma protein binding of azelastine and desmethylazelastine are approximately 88% and 97%, respectively.
Fluticasone propionate has a large volume of distribution at steady-state (approximately 318 L). Plasma protein binding is 91%.
Metabolism: Azelastine is extensively metabolised, desmethylazelastine being the principal metabolite. No specific isoform of cytochrome P450 was found to be specific in the metabolism of azelastine at low concentrations (6 - 30 ng/mL) in human liver microsomes.
Fluticasone propionate is cleared rapidly from the systemic circulation, principally by hepatic metabolism to an inactive carboxylic acid metabolite, by the cytochrome P450 enzyme CYP3A4. Swallowed fluticasone propionate is also subject to extensive first pass metabolism. Care should be taken when co-administering potent CYP3A4 inhibitors such as ketoconazole and ritonavir as there is potential for increased systemic exposure to fluticasone propionate (see Use of Cytochrome P450 3A4 Inhibitors under Precautions and Interactions).
Elimination: Plasma elimination half-lives after a single dose of azelastine are 22 hours for azelastine and 56 hours for the therapeutically active metabolite N-desmethyl azelastine. Up to 74% of radiolabelled oral or intravenous dose is excreted in faeces and 26% in urine. Thirteen percent is excreted in urine as unchanged azelastine.
The elimination rate of intravenous administered fluticasone propionate is linear over the 250-1000 μg dose range and is characterised by a high plasma clearance (CL=1.1 L/min). Peak plasma concentrations are reduced by approximately 98% within 3-4 hours and only low plasma concentrations were associated with the 7.8 h terminal half-life. The renal clearance of fluticasone propionate is negligible (<0.2%) and less than 5% as the carboxylic acid metabolite. The major route of elimination is the excretion of fluticasone propionate and its metabolites in the bile.
Special Populations: DYMISTA was not studied in any special populations, and no gender-specific pharmacokinetic data have been obtained. The following data are available for the individual active component, azelastine: Hepatic Impairment: No significant difference was found in t½, Cmax or AUC in an oral single dose study of azelastine in 6 patients with hepatic impairment compared to normal subjects. Caution is warranted in extrapolating these data to long - term use. (see Use in Patients with Hepatic Impairment under Precautions).
Renal Impairment: In a single oral dose study of azelastine in 9 patients, renal insufficiency (creatinine clearance <50 mL/min) resulted in a 70-75% higher Cmax and AUC compared to normal subjects. However, the number of patients evaluated in this study is too small to draw meaningful conclusions. No information regarding the use of azelastine nasal spray in renally impaired patients is available. (see Use in Patients with Renal Impairment under Precautions).
Age: A pharmacokinetic study in elderly patients (n=15) receiving oral azelastine 4.4 mg twice daily found a prolongation of the Tmax and an increase in Cmax and AUC compared to results in healthy volunteers. There have been no specific studies in the elderly with the nasal spray. In clinical and post-marketing studies of the nasal spray, no increase in the incidence of adverse reactions has been seen in elderly patients.
The efficacy and safety of DYMISTA in children under 12 years of age have not been established (see Use in Children and Adolescents under Precautions).
Race: The effect of race has not been evaluated.