Supplementary analgesic agents are generally required in addition to DIPRIVAN.
DIPRIVAN has been used in association with spinal and epidural anaesthesia and with commonly used premedicants, neuromuscular blocking drugs, inhalation agents and analgesic agents; no pharmacological incompatibility has been encountered. Lower doses of DIPRIVAN may be required where general anaesthesia is used as an adjunct to regional anaesthetic techniques.
A. Adults: INDUCTION OF GENERAL ANAESTHESIA: DIPRIVAN may be used to induce anaesthesia by slow bolus injection or infusion.
In unpremedicated and premedicated patients, it is recommended that DIPRIVAN should be titrated (approximately 40 mg every 10 seconds in an average healthy adult by bolus injection or infusion) against the response of the patient until the clinical signs show the onset of anaesthesia. Most adult patients aged less than 55 years are likely to require 1.5 to 2.5 mg/kg of DIPRIVAN. The total dose required can be reduced by lower rates of administration (20 - 50 mg/min). Over this age, the requirement will generally be less. In patients of ASA Grades 3 and 4, lower rates of administration should be used (approximately 20 mg every 10 seconds).
MAINTENANCE OF GENERAL ANAESTHESIA: Anaesthesia can be maintained by administering DIPRIVAN either by continuous infusion or by repeat bolus injections to maintain the depth of anaesthesia required.
Continuous Infusion: The required rate of administration varies considerably between patients but rates in the region of 4 to 12 mg/kg/h usually maintain satisfactory anaesthesia.
Repeat Bolus Injections: If a technique involving repeat bolus injections is used, increments of 25 mg to 50 mg may be given according to clinical need.
SEDATION DURING INTENSIVE CARE: When used to provide sedation for ventilated adult patients undergoing intensive care, it is recommended that DIPRIVAN be given by continuous infusion.
The infusion rate should be adjusted according to the depth of sedation required but rates in the region of 0.3 to 4.0 mg/kg/h should achieve satisfactory sedation in most adult patients.
CONSCIOUS SEDATION FOR SURGICAL AND DIAGNOSTIC PROCEDURES: To provide sedation for surgical and diagnostic procedures rates of administration should be individualised and titrated to clinical response.
Most patients will require 0.5 to 1 mg/kg over 1 to 5 minutes to initiate sedation.
Maintenance of sedation may be accomplished by titrating DIPRIVAN infusion to the desired level of sedation - most patients will require 1.5 to 4.5 mg/kg/h. In addition to the infusion, bolus administration of 10 to 20 mg may be used if a rapid increase in the depth of sedation is required. In patients in ASA grades 3 and 4 the rate of administration and dosage may need to be reduced.
B. Elderly Patients: In elderly patients the dose requirement for induction of anaesthesia with DIPRIVAN is reduced. The reduction should take account of the physical status and age of the patient. The reduced dose should be given at a slower rate and titrated against the response. Where DIPRIVAN is used for maintenance of anaesthesia or sedation the rate of infusion or 'target concentration' should also be reduced. Patients of ASA grades 3 and 4 will require further reductions in dose and dose rate. Rapid bolus administration (single or repeated) should not be used in the elderly as this may lead to cardiorespiratory depression.
C. Children: INDUCTION OF GENERAL ANAESTHESIA: DIPRIVAN is not recommended for use in children less than 3 years of age (see Adverse Reactions).
When used to induce anaesthesia in children, it is recommended that DIPRIVAN be given slowly until the clinical signs show the onset of anaesthesia. The dose should be adjusted for age and/or weight.
Most patients over 8 years of age are likely to require approximately 2.5 mg/kg of DIPRIVAN for induction of anaesthesia. Under this age the requirement may be more. Lower dosage is recommended for children of ASA grades 3 and 4.
MAINTENANCE OF GENERAL ANAESTHESIA: DIPRIVAN is not recommended for use in children less than 3 years of age.
Anaesthesia can be maintained by administering DIPRIVAN by infusion or repeat bolus injection to maintain the depth of anaesthesia required. The required rate of administration varies considerably between patients but rates in the region of 9 to 15 mg/kg/h usually achieve satisfactory anaesthesia.
CONSCIOUS SEDATION FOR SURGICAL & DIAGNOSTIC PROCEDURES: DIPRIVAN is not recommended for conscious sedation in children as safety and efficacy have not been demonstrated.
SEDATION DURING INTENSIVE CARE: DIPRIVAN is not recommended for sedation in children as safety and efficacy have not been demonstrated.
Although no causal relationship has been established, serious adverse events (including fatalities) have been observed from spontaneous reports of unlicensed use and these events were seen most often in children with respiratory tract infections given doses in excess of those recommended for adults.
D. Administration: DIPRIVAN can be used for infusion undiluted from plastic syringes or glass infusion bottles. When DIPRIVAN is used undiluted to maintain anaesthesia, it is recommended that equipment such as syringe pumps or volumetric infusion pumps should always be used to control infusion rates.
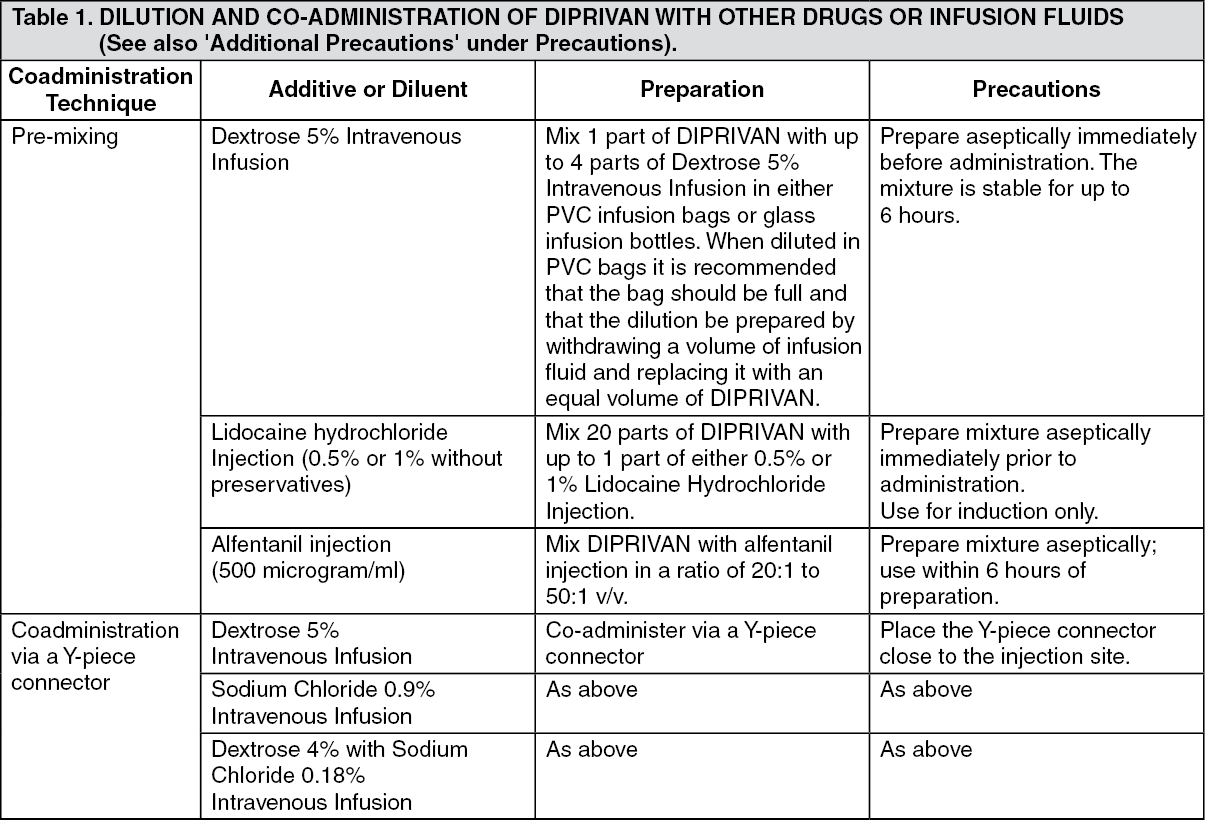
DIPRIVAN may also be used diluted with 5% Dextrose Intravenous Infusion only, in PVC infusion bags or glass infusion bottles. Dilutions, which must not exceed 1 in 5 (2 mg Propofol/ml) should be prepared aseptically immediately before administration. The mixture is stable for up to 6 hours.
The dilution may be used with a variety of infusion control techniques but a giving set used alone will not avoid the risk of accidental, uncontrolled infusion of large volumes of diluted DIPRIVAN. A burette, drop counter or volumetric pump must be included in the infusion line. The risk of uncontrolled infusion must be taken into account when deciding the maximum amount of dilution in the burette.
DIPRIVAN may be administered via a Y-piece close to the injection site, into infusions of Dextrose 5% Intravenous Infusion, Sodium Chloride 0.9% Intravenous Infusion or Dextrose 4% with Sodium Chloride 0.18% Intravenous Infusion.
DIPRIVAN may be premixed with alfentanil injection containing 500 micrograms/ml alfentanil ('Rapifen'; Janssen Pharmaceuticals Ltd.) in the ratio of 20:1 to 50:1 v/v. Mixtures should be prepared using sterile technique and used within 6 hours of preparation.
To reduce pain on initial injection, DIPRIVAN used for induction may be mixed with Lidocaine Injection in a plastic syringe in the ratio of 20 parts DIPRIVAN with up to one part of either 0.5% or 1% Lidocaine Injection immediately prior to administration. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
