


 Sign Out
Sign Out

Pharmacology: Mechanism of Action: Dexlansoprazole is a PPI that suppresses gastric acid secretion by specific inhibition of the (H+,K+)-ATPase in the gastric parietal cell. By acting specifically on the proton pump, dexlansoprazole blocks the final step of acid production.
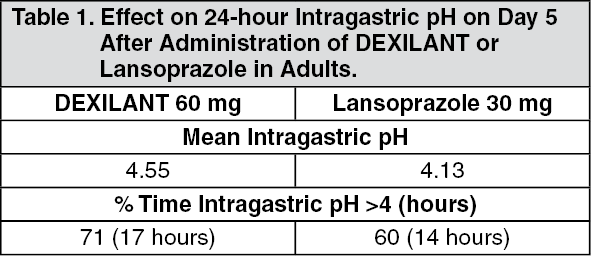
Pharmacodynamics: Antisecretory Activity: The effects of Dexilant 60 mg (n=20) or lansoprazole 30 mg (n=23) once daily for five days on 24-hour intragastric pH were assessed in healthy subjects in a multiple-dose crossover study. The results are summarized in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSerum Gastrin Effects: The effect of Dexilant on serum gastrin concentrations was evaluated in approximately 3460 patients in clinical trials up to 8 weeks and in 1023 patients for up to 6 to 12 months. The mean fasting gastrin concentrations increased from baseline during treatment with Dexilant 30 mg and 60 mg doses. In patients treated for more than 6 months, mean serum gastrin levels increased during approximately the first 3 months of treatment and were stable for the remainder of treatment. Mean serum gastrin levels returned to pre-treatment levels within one month of discontinuation of treatment.
During treatment with antisecretory medicinal products, serum gastrin increases in response to the decreased acid secretion. Also CgA increases due to decreased gastric acidity. The increased CgA level may interfere with investigations for neuroendocrine tumours.
Available published evidence suggests that proton pump inhibitors should be discontinued between 5 days and 2 weeks prior to CgA measurements. This is to allow CgA levels that might be spuriously elevated following PPI treatment to return to reference range.
Enterochromaffin-Like Cell (ECL) Effects: There were no reports of ECL cell hyperplasia in gastric biopsy specimens obtained from 653 patients treated with Dexilant 30 mg, 60 mg or 90 mg for up to 12 months.
During lifetime exposure of rats dosed daily with up to 150 mg per kg per day of lansoprazole, marked hypergastrinemia was observed followed by ECL cell proliferation and formation of carcinoid tumors, especially in female rats.
Effect on Cardiac Repolarization: A study was conducted to assess the potential of Dexilant to prolong the QT/QTc interval in healthy adult subjects. Dexilant doses of 90 mg or 300 mg did not delay cardiac repolarization compared to placebo. The positive control (moxifloxacin) produced statistically significantly greater mean maximum and time-averaged QT/QTc intervals compared to placebo.
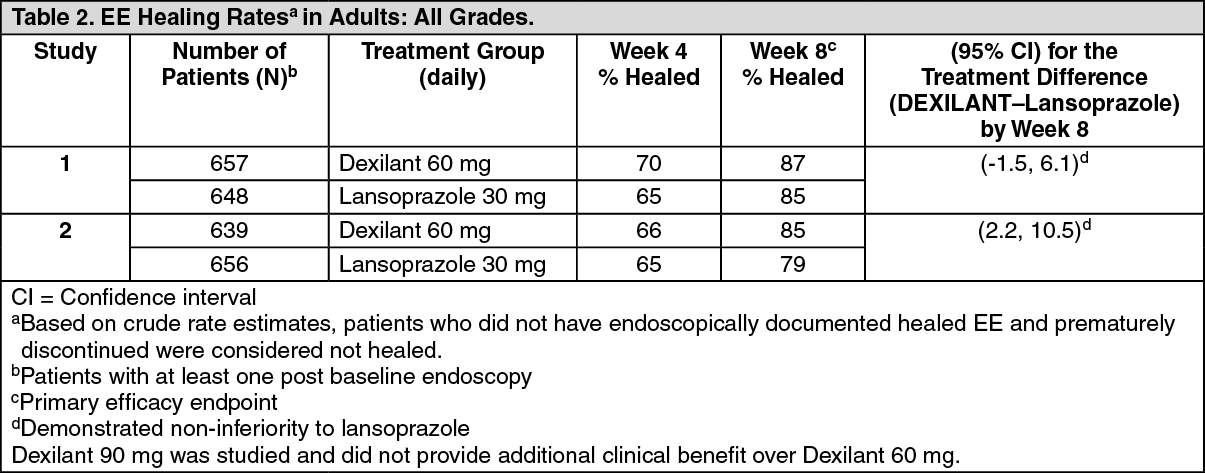
Clinical Studies: Healing of Erosive Esophagitis: Two multi-center, double-blind, active-controlled, randomized, 8-week studies were conducted in patients with endoscopically confirmed EE. Severity of the disease was classified based on the Los Angeles Classification Grading System (Grades A-D). Patients were randomized to one of the following three treatment groups: Dexilant 60 mg daily, Dexilant 90 mg daily or lansoprazole 30 mg daily. Patients who were H. pylori positive or who had Barrett's Esophagus and/or definite dysplastic changes at baseline were excluded from these studies. A total of 4092 patients were enrolled and ranged in age from 18 to 90 years (median age 48 years) with 54% male. Race was distributed as follows: 87% Caucasian, 5% Black and 8% other. Based on the Los Angeles Classification, 71% of patients had mild EE (Grades A and B) and 29% of patients had moderate to severe EE (Grades C and D) before treatment.
The studies were designed to test non-inferiority. If non-inferiority was demonstrated then superiority would be tested. Although non-inferiority was demonstrated in both studies, the finding of superiority in one study was not replicated in the other.
The proportion of patients with healed EE at week 4 or 8 is presented as follows in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
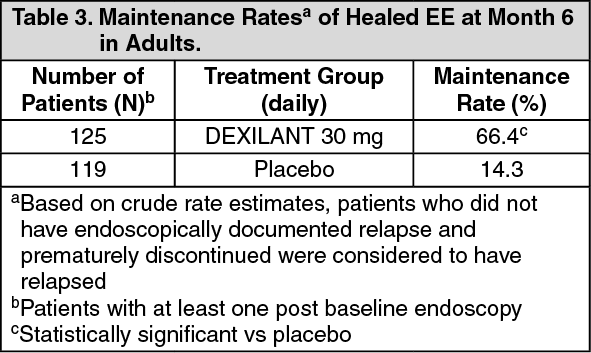
Click on icon to see table/diagram/imageMaintenance of Healed Erosive Esophagitis: A multi-center, double-blind, placebo-controlled, randomized study was conducted in patients who successfully completed an EE study and showed endoscopically confirmed healed EE. Maintenance of healing and symptom resolution over a six-month period were evaluated with Dexilant 30 mg or 60 mg once daily compared to placebo. A total of 445 patients were enrolled and ranged in age from 18 to 85 years (median age 49 years), with 52% female. Race was distributed as follows: 90% Caucasian, 5% Black and 5% other.
Sixty-six percent of patients treated with 30 mg of Dexilant remained healed over the six-month time period as confirmed by endoscopy (see Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDexilant 60 mg was studied and did not provide additional clinical benefit over Dexilant 30 mg.
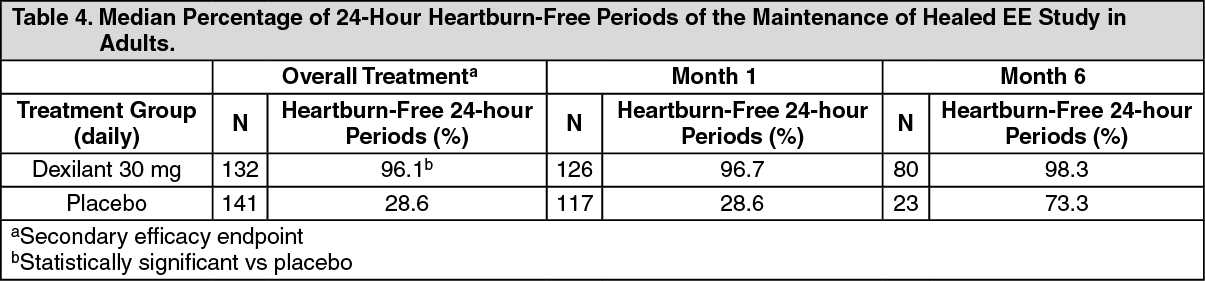
The effect of Dexilant 30 mg on maintenance of relief of heartburn was also evaluated. Upon entry into the maintenance study, a majority of patients' baseline heartburn severity was rated as none. Dexilant 30 mg demonstrated a statistically significantly higher percent of 24-hour heartburn-free periods compared to placebo over the 6-month treatment period (see Table 4). The majority of patients treated with placebo discontinued due to relapse of EE between month two and month six. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSymptomatic Non-Erosive GERD: A multi-center, double-blind, placebo-controlled, randomized, 4-week study was conducted in patients with a diagnosis of symptomatic non-erosive GERD made primarily by presentation of symptoms. These patients who identified heartburn as their primary symptom, had a history of heartburn for 6 months or longer, had heartburn on at least 4 of 7 days immediately prior to randomization and had no esophageal erosions as confirmed by endoscopy. However, patients with symptoms which were not acid-related may not have been excluded using these inclusion criteria. Patients were randomized to one of the following treatment groups: Dexilant 30 mg daily, 60 mg daily, or placebo. A total of 947 patients were enrolled and ranged in age from 18 to 86 years (median age 48 years) with 71% female. Race was distributed as follows: 82% Caucasian, 14% Black and 4% other.
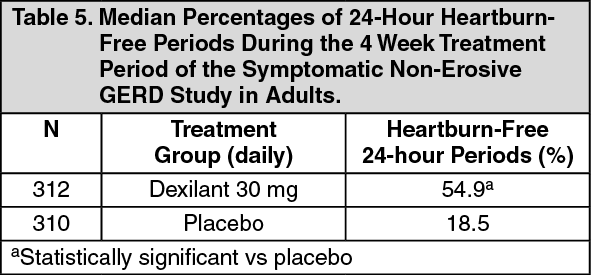
Dexilant 30 mg provided statistically significantly greater percent of days with heartburn-free 24-hour periods over placebo as assessed by daily diary over 4 weeks (see Table 5). Dexilant 60 mg was studied and provided no additional clinical benefit over Dexilant 30 mg.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA higher percentage of patients on Dexilant 30 mg had heartburn-free 24-hour periods compared to placebo as early as the first three days of treatment and this was sustained throughout the treatment period (percentage of patients on Day 3: Dexilant 38% versus placebo 15%; on Day 28: Dexilant 63% versus placebo 40%).
Pediatric GERD: Use of DEXILANT in patients 12 to 17 years of age is supported by evidence from adequate and well-controlled studies of DEXILANT capsules in adults, with additional safety, efficacy, and pharmacokinetic data from studies performed in pediatric patients.
Treatment of Symptomatic Non-Erosive GERD: In a single-arm, open-label, multi-center trial, 104 pediatric patients 12 to 17 years of age with symptomatic non-erosive GERD were treated with DEXILANT 30 mg capsules once daily, for four weeks to evaluate safety and effectiveness. Patients had a documented history of GERD symptoms for at least three months prior to screening, reported heartburn on at least three out of seven days during screening, and had no esophageal erosions as confirmed by endoscopy. The median age was 15 years, with females accounting for 70% of the patients. During the four week treatment period, the median percentage of 24 hour heartburn free periods was 47%.
Healing of EE, Maintenance of Healed EE and Relief of Heartburn: Patients 12 to 17 Years of Age: In a multi-center, 24-week study, 62 adolescents with a documented history of GERD for at least 3 months and endoscopically-proven EE were treated with dexlansoprazole 60 mg capsule once daily, for 8 weeks to evaluate safety and effectiveness. Patients ranged in age from 12 to 17 years (median age 15 years) with males accounting for 61% of the patients. Based on the Los Angeles Classification Grading Scale, 96.8% of the EE patients had mild EE (Grades A and B), and 3.2% of patients had moderate to severe EE (Grades C and D) before treatment.
EE healing rates in adolescents (87.9%) were similar to adults (85% - 87%) for up to 8 weeks of treatment.
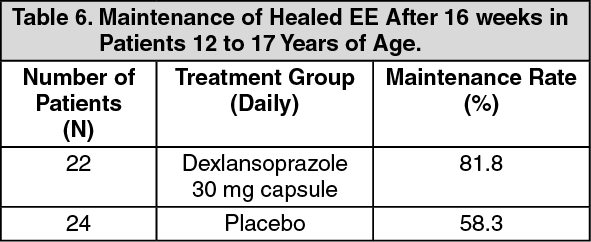
After the initial 8 weeks of treatment, patients with endoscopically confirmed healed EE were randomized to receive treatment with dexlansoprazole 30 mg capsule or placebo, once daily for an additional 16 weeks. Eighty-two percent of patients treated with dexlansoprazole 30 mg capsule remained healed over the four-month treatment period as confirmed by endoscopy (see Table 6).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDuring the 16 week maintenance period, median percentage of 24-hour heartburn-free periods were 86.6% for those receiving dexlansoprazole 30 mg capsule compared to 68.1% for those receiving placebo. The results for maintenance of healed EE and heartburn relief were similar to adults.
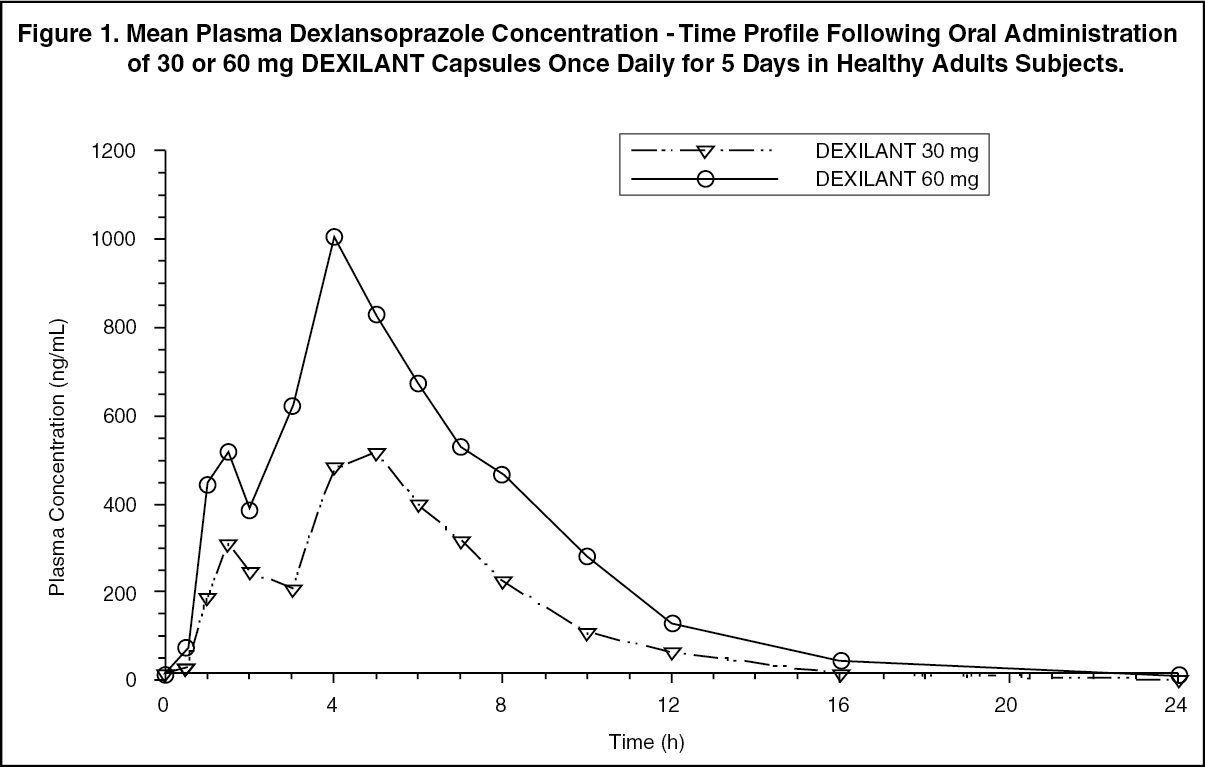
Pharmacokinetics: The dual delayed release formulation of Dexilant results in a dexlansoprazole plasma concentration-time profile with two distinct peaks; the first peak occurs 1 to 2 hours after administration, followed by a second peak within 4 to 5 hours (see Figure 1). Dexlansoprazole is eliminated with a half-life of approximately 1 to 2 hours in healthy subjects and in patients with symptomatic GERD. No accumulation of dexlansoprazole occurs after multiple, once daily doses of Dexilant 30 mg or 60 mg, although mean AUCt and Cmax values of dexlansoprazole were slightly higher (less than 10%) on day 5 than on day 1. (See Figure 1.)
 Click on icon to see table/diagram/image
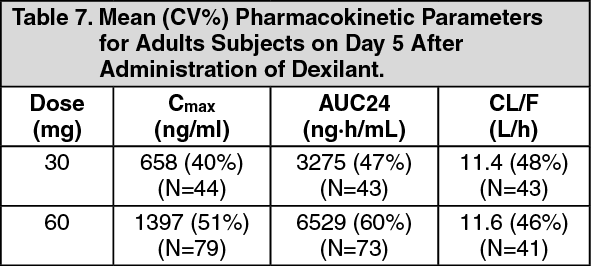
Click on icon to see table/diagram/imageThe pharmacokinetics of dexlansoprazole are highly variable, with percent coefficient of variation (CV%) values for Cmax, AUC, and CL/F of greater than 30% (see Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAbsorption: After oral administration of Dexilant 30 mg or 60 mg to healthy subjects and symptomatic GERD patients, mean Cmax and AUC values of dexlansoprazole increased approximately dose proportionally (see Figure 1).
Distribution: Plasma protein binding of dexlansoprazole ranged from 96.1% to 98.8% in healthy subjects and was independent of concentration from 0.01 to 20 mcg per mL. The apparent volume of distribution (Vz/F) after multiple doses in symptomatic GERD patients was 40.3 L.
Metabolism: Dexlansoprazole is extensively metabolized in the liver by oxidation, reduction, and subsequent formation of sulfate, glucuronide and glutathione conjugates to inactive metabolites. Oxidative metabolites are formed by the cytochrome P450 (CYP) enzyme system including hydroxylation mainly by CYP2C19, and oxidation to the sulfone by CYP3A4.
CYP2C19 is a polymorphic liver enzyme which exhibits three phenotypes in the metabolism of CYP2C19 substrates; extensive metabolizers (*1/*1), intermediate metabolizers (*1/mutant) and poor metabolizers (mutant/mutant). Dexlansoprazole is the major circulating component in plasma regardless of CYP2C19 metabolizer status. In CYP2C19 intermediate and extensive metabolizers, the major plasma metabolites are 5-hydroxy dexlansoprazole and its glucuronide conjugate, while in CYP2C19 poor metabolizers dexlansoprazole sulfone is the major plasma metabolite.
Elimination: Following the administration of Dexilant, no unchanged dexlansoprazole is excreted in urine. Following the administration of [14C] dexlansoprazole to 6 healthy male subjects, approximately 50.7% (standard deviation (SD): 9.0%) of the administered radioactivity was excreted in urine and 47.6% (SD: 7.3%) in the feces. Apparent clearance (CL/F) in healthy subjects was 11.4 to 11.6 L/h, respectively, after 5-days of 30 or 60 mg once daily administration.
Effect of CYP2C19 Polymorphism on Systemic Exposure of Dexlansoprazole: Systemic exposure of dexlansoprazole is generally higher in intermediate and poor metabolizers. In male Japanese subjects who received a single dose of Dexilant 30 mg or 60 mg (N=2 to 6 subjects/group), mean dexlansoprazole Cmax and AUC values were up to 2 times higher in intermediate compared to extensive metabolizers; in poor metabolizers, mean Cmax was up to 4 times higher and mean AUC was up to 12 times higher compared to extensive metabolizers. Though such study was not conducted in Caucasians and African Americans, it is expected dexlansoprazole exposure in these races will be affected by CYP2C19 phenotypes as well.
Effect of Food on Pharmacokinetics and Pharmacodynamics: In food-effect studies in healthy subjects receiving Dexilant under various fed conditions compared to fasting, increases in Cmax ranged from 12% to 55%, increases in AUC ranged from 9% to 37%, and tmax varied (ranging from a decrease of 0.7 hours to an increase of 3 hours). No significant differences in mean intragastric pH were observed between fasted and various fed conditions. However, the percentage of time intragastric pH exceeded 4 over the 24-hour dosing interval decreased slightly when Dexilant was administered after a meal (57%) relative to fasting (64%), primarily due to a decreased response in intragastric pH during the first 4 hours after dosing. Because of this, while Dexilant can be taken without regard to food, some patients may benefit from administering the dose prior to a meal if post-meal symptoms do not resolve under post-fed conditions.
Special Populations: Pediatric Use: The pharmacokinetics of dexlansoprazole in patients under the age of 12 years have not been studied.
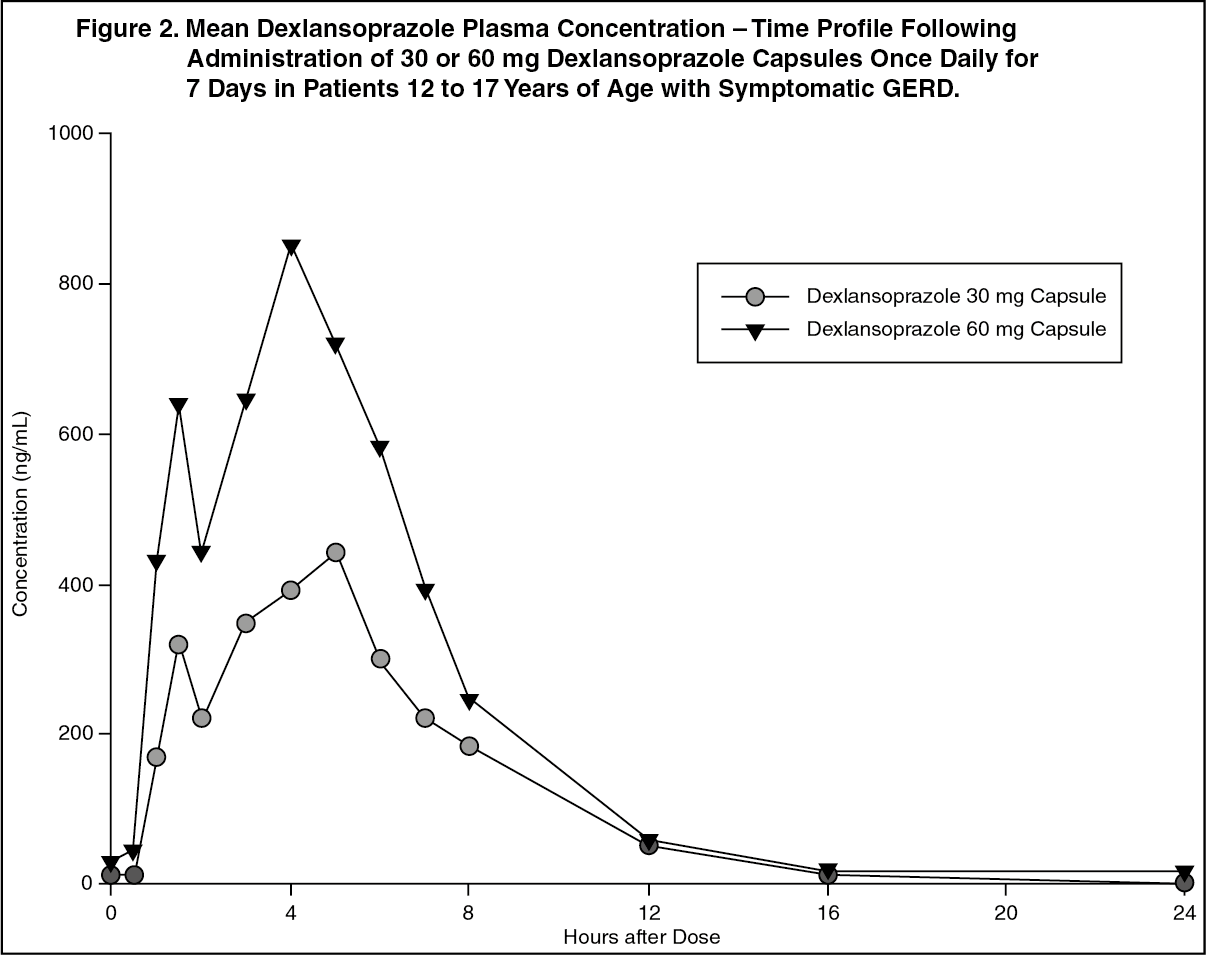
Patients 12 to 17 Years of Age: The pharmacokinetics of dexlansoprazole were studied in 36 patients with symptomatic GERD 12 to 17 years of age in a multi-center study. Patients were randomized to receive Dexilant 30 mg or 60 mg once daily for 7 days (see Figure 2 and Table 8). In adolescents, dexlansoprazole mean Cmax was 81% to 105% of the adult mean Cmax value, mean AUC was 78% to 88% of the adult mean AUC value, and mean CL/F was 112% to 132% of the adult mean CL/F value. Overall, dexlansoprazole pharmacokinetics in patients 12 to 17 years of age were similar to those observed in healthy adults (see Figure 1 and Table 7). (See Figure 2 and Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageGeriatric Use: The terminal elimination half-life of dexlansoprazole is significantly increased in geriatric subjects compared to younger subjects (2.23 and 1.5 hours, respectively); this difference is not clinically relevant. Dexlansoprazole exhibited higher systemic exposure (AUC) in geriatric subjects (34.5% higher) than younger subjects. No dosage adjustment is needed in geriatric patients [see Dosage & Administration].
Renal Impairment: Dexlansoprazole is extensively metabolized in the liver to inactive metabolites, and no parent drug is recovered in the urine following an oral dose of dexlansoprazole. Therefore, the pharmacokinetics of dexlansoprazole are not expected to be altered in patients with renal impairment, and no studies were conducted in subjects with renal impairment [see Dosage & Administration]. In addition, the pharmacokinetics of lansoprazole were studied in patients with mild, moderate or severe renal impairment; results demonstrated no need for a dose adjustment for this patient population.
Hepatic Impairment: In a study of 12 patients with moderately impaired hepatic function who received a single oral dose of Dexilant 60 mg, plasma exposure (AUC) of bound and unbound dexlansoprazole in the hepatic impairment group was approximately 2 times greater compared to subjects with normal hepatic function. This difference in exposure was not due to a difference in protein binding between the two liver function groups. No adjustment for Dexilant is necessary for patients with mild hepatic impairment (Child-Pugh Class A). Dexilant 30 mg should be considered for patients with moderate hepatic impairment (Child-Pugh Class B). No studies have been conducted in patients with severe hepatic impairment (Child-Pugh Class C) [see Dosage & Administration].
Gender: In a study of 12 male and 12 female healthy subjects who received a single oral dose of Dexilant 60 mg, females had higher systemic exposure (AUC) (42.8% higher) than males. No dosage adjustment is necessary in patients based on gender.
Drug-Drug Interactions: Warfarin: In a study of 20 healthy subjects, co-administration of Dexilant 90 mg once daily for 11 days with a single 25 mg oral dose of warfarin on day 6 did not result in any significant differences in the pharmacokinetics of warfarin or INR compared to administration of warfarin with placebo. However, there have been reports of increased INR and prothrombin time in patients receiving PPIs and warfarin concomitantly [see Interactions].
Cytochrome P 450 Interactions: Dexlansoprazole is metabolized, in part, by CYP2C19 and CYP3A4 [see Pharmacology: Pharmacokinetics as previously mentioned].
In vitro studies have shown that dexlansoprazole is not likely to inhibit CYP isoforms 1A1, 1A2, 2A6, 2B6, 2C8, 2C9, 2D6, 2E1 or 3A4. As such, no clinically relevant interactions with drugs metabolized by these CYP enzymes would be expected. Furthermore, in vivo studies showed that Dexilant did not have an impact on the pharmacokinetics of coadministered phenytoin (CYP2C9 substrate) or theophylline (CYP1A2 substrate). The subjects' CYP1A2 genotypes in the drug-drug interaction study with theophylline were not determined. Although in vitro studies indicated that Dexilant has the potential to inhibit CYP2C19 in vivo, an in vivo drug-drug interaction study in mainly CYP2C19 extensive and intermediate metabolizers has shown that Dexilant does not affect the pharmacokinetics of diazepam (CYP2C19 substrate).
Clopidogrel: Clopidogrel is metabolized to its active metabolite in part by CYP2C19. A study of healthy subjects who were CYP2C19 extensive metabolizers, receiving once daily administration of clopidogrel 75 mg alone or concomitantly with Dexilant 60 mg (n=40), for 9 days was conducted. The mean AUC of the active metabolite of clopidogrel was reduced by approximately 9% (mean AUC ratio was 91%, with 90% CI of 86-97%) when Dexilant was coadministered compared to administration of clopidogrel alone. Pharmacodynamic parameters were also measured and demonstrated that the change in inhibition of platelet aggregation (induced by 5 mcM ADP) was related to the change in the exposure to clopidogrel active metabolite. The clinical significance of this finding is not clear.
Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: The carcinogenic potential of dexlansoprazole was assessed using lansoprazole studies. In two 24-month carcinogenicity studies, Sprague-Dawley rats were treated orally with lansoprazole at doses of 5 to 150 mg per kg per day, about 1 to 40 times the exposure on a body surface (mg/m2) basis of a 50 kg person of average height [1.46 m2 body surface area (BSA)] given the recommended human dose of lansoprazole 30 mg per day.
Lansoprazole produced dose-related gastric ECL cell hyperplasia and ECL cell carcinoids in both male and female rats [see Pharmacology: Pharmacodynamics as previously mentioned].
In rats, lansoprazole also increased the incidence of intestinal metaplasia of the gastric epithelium in both sexes. In male rats, lansoprazole produced a dose-related increase of testicular interstitial cell adenomas. The incidence of these adenomas in rats receiving doses of 15 to 150 mg per kg per day (4 to 40 times the recommended human lansoprazole dose based on BSA) exceeded the low background incidence (range = 1.4 to 10%) for this strain of rat.
In a 24-month carcinogenicity study, CD-1 mice were treated orally with lansoprazole doses of 15 to 600 mg per kg per day, 2 to 80 times the recommended human lansoprazole dose based on BSA. Lansoprazole produced a dose-related increased incidence of gastric ECL cell hyperplasia. It also produced an increased incidence of liver tumors (hepatocellular adenoma plus carcinoma). The tumor incidences in male mice treated with 300 and 600 mg lansoprazole per kg per day (40 to 80 times the recommended human lansoprazole dose based on BSA) and female mice treated with 150 to 600 mg lansoprazole per kg per day (20 to 80 times the recommended human lansoprazole dose based on BSA) exceeded the ranges of background incidences in historical controls for this strain of mice. Lansoprazole treatment produced adenoma of rete testis in male mice receiving 75 to 600 mg per kg per day (10 to 80 times the recommended human lansoprazole dose based on BSA).
A 26-week p53 (+/-) transgenic mouse carcinogenicity study of lansoprazole was not positive. Lansoprazole was positive in the Ames test and the in vitro human lymphocyte chromosomal aberration assay. Lansoprazole was not genotoxic in the ex vivo rat hepatocyte unscheduled DNA synthesis (UDS) test, the in vivo mouse micronucleus test or the rat bone marrow cell chromosomal aberration test.
Dexlansoprazole was positive in the Ames test and in the in vitro chromosome aberration test using Chinese hamster lung cells. Dexlansoprazole was negative in the in vivo mouse micronucleus test. The potential effects of dexlansoprazole on fertility and reproductive performance were assessed using lansoprazole studies. Lansoprazole at oral doses up to 150 mg per kg per day (40 times the recommended human lansoprazole dose based on BSA) was found to have no effect on fertility and reproductive performance of male and female rats.
Animal Toxicology and/or Pharmacology: Reproductive Toxicology Studies: A reproduction study conducted in rabbits at oral dexlansoprazole doses up to 30 mg per kg per day (approximately 9 times the maximum recommended human dexlansoprazole dose [60 mg per day] based on BSA) revealed no evidence of impaired fertility or harm to the fetus due to dexlansoprazole. In addition, reproduction studies performed in pregnant rats with oral lansoprazole at doses up to 150 mg per kg per day (40 times the recommended human lansoprazole dose based on BSA) and in pregnant rabbits at oral lansoprazole doses up to 30 mg per kg per day (16 times the recommended human lansoprazole dose based on BSA) revealed no evidence of impaired fertility or harm to the fetus due to lansoprazole.