Pharmacotherapeutic group: Lipid modifying substances, HMG-CoA reductase inhibitors in combination with other lipid modifying substances.
ATC code: C10BA04.
Pharmacology: Pharmacodynamics: Mechanism of action: Fenofibrate:
Fenofibrate is a fibric acid derivative whose lipid modifying effects reported in humans are mediated via activation of Peroxisome Proliferator Activated Receptor type alpha (PPARα).
Through activation of PPARα, fenofibrate activates lipoprotein lipase production and reduces production of apoprotein CIII. Activation of PPARα also induces an increase in the synthesis of apoproteins AI and AII.
Simvastatin: Simvastatin, which is an inactive lactone, is hydrolyzed in the liver to the corresponding active betahydroxyacid form which has a potent activity in inhibiting HMG-CoA reductase (3 hydroxy-3 methylglutaryl CoA reductase). This enzyme catalyses the conversion of HMG-CoA to mevalonate, an early and rate-limiting step in the biosynthesis of cholesterol.
Cholib 145 mg/20 mg film-coated tablet contains fenofibrate and simvastatin, which have different modes of action as described previously.
Pharmacodynamic effects: Fenofibrate: Studies with fenofibrate on lipoprotein fractions show decreases in levels of LDL and VLDL cholesterol (VLDL-C). HDL-C levels are frequently increased. LDL and VLDL triglycerides are reduced. The overall effect is a decrease in the ratio of low and very low-density lipoproteins to high-density lipoproteins.
Fenofibrate also has a uricosuric effect leading to reduction in uric acid levels of approximately 25%.
Simvastatin: Simvastatin has been shown to reduce both normal and elevated LDL-C concentrations. LDL is formed from very-low-density protein (VLDL) and is catabolised predominantly by the high affinity LDL receptor. The mechanism of the LDL lowering effect of simvastatin may involve both reduction of VLDL-C concentration and induction of the LDL receptor, leading to reduced production and increased catabolism of LDL-C. Apolipoprotein B also falls substantially during treatment with simvastatin. In addition, simvastatin moderately increases HDL-C and reduces plasma TG.
As a result of these changes the ratios of TC to HDL-C and LDL-C to HDL-C are reduced.
The respective effects of simvastatin and fenofibrate are complementary.
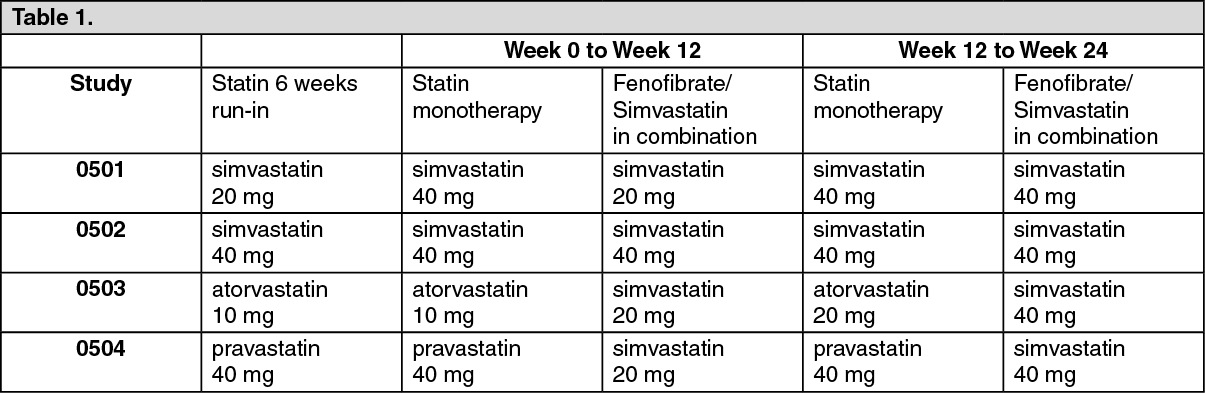
Clinical efficacy and safety: Four pivotal clinical studies were carried out in the clinical program. Overall, 7,583 subjects with mixed dyslipidemia entered a 6 week statin run-in period. Of these, 2,474 subjects were randomized for 24 weeks treatment, 1,237 subjects received fenofibrate and simvastatin co-administration and 1,230 subjects received statin monotherapy all administered in the evening. Statin type and dose used: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Study 0501 evaluated 2 different doses of fenofibrate-simvastatin combination compared to simvastatin 40 mg for a 24 week double-blind period. The primary efficacy criterion was superiority of the combination fenofibrate 145 and simvastatin 20 mg versus simvastatin 40 mg on TG decrease and HDL-C increase and non-inferiority for LDL-C decrease at 12 weeks. (See Table 2.)
Click on icon to see table/diagram/image
After the first 12 weeks of treatment, the combination of fenofibrate 145 mg and simvastatin 20 mg showed superiority over simvastatin 40 mg for TG reduction and HDL-C increase but did not meet the criteria for non-inferiority on LDL-C. The combination of fenofibrate 145 mg with simvastatin 20 mg demonstrated statistically significant superiority on apoA1 increase and fibrinogen decrease compared to simvastatin 40 mg.
Supportive study: The Action to Control Cardiovascular Risk in Diabetes (ACCORD) lipid trial was a randomized placebo-controlled study of 5,518 patients with type 2 diabetes mellitus treated with fenofibrate in addition to simvastatin. Fenofibrate plus simvastatin therapy did not show any significant differences compared to simvastatin monotherapy in the composite primary outcome of non-fatal myocardial infarction, non-fatal stroke, and cardiovascular death (hazard ratio [HR] 0.92, 95% CI 0.79-1.08, p = 0.32; absolute risk reduction: 0.74%). In the pre-specified subgroup of dyslipidaemic patients, defined as those in the lowest tertile of HDL-C (≤ 34 mg/dl or 0.88 mmol/L) and highest tertile of TG (≥ 204 mg/dl or 2.3 mmol/L) at baseline, fenofibrate plus simvastatin therapy demonstrated a 31% relative reduction compared to simvastatin monotherapy for the composite primary outcome (hazard ratio [HR] 0.69, 95% CI 0.49-0.97, p=0.03; absolute risk reduction: 4.95%). Another prespecified subgroup analysis identified a statistically significant treatment-by-gender interaction (p=0.01) indicating a possible treatment benefit of combination therapy in men (p=0.037) but a potentially higher risk for the primary outcome in women treated with combination therapy compared to simvastatin monotherapy (p=0.069). This was not observed in the aforementioned subgroup of patients with dyslipidaemia but there was also no clear evidence of benefit in dyslipidaemic women treated with fenofibrate plus simvastatin, and a possible harmful effect in this subgroup could not be excluded.
Pharmacokinetics: The geometric mean ratios and 90% CIs for the comparison of AUC, AUC(0-t) and Cmax of the active metabolites, fenofibric acid and simvastatin acid, of the fixed dose combination Cholib 145 mg/20 mg film-coated tablets and the co-administration of the separate 145 mg fenofibrate and 20 mg simvastatin tablets as used in the clinical program, were all within the 80-125% bioequivalence interval.
The geomean maximum plasma level (Cmax) of the inactive parent simvastatin was 2.7 ng/mL for the fixed dose combination Cholib 145 mg/20 mg film-coated tablets and 3.9 ng/mL for the co-administration of the separate 145 mg fenofibrate and 20 mg simvastatin tablets as used in the clinical program.
The geometric mean ratios and 90% CIs for the comparison of plasma exposure (AUC and AUC (0-t)) to simvastatin after administration of the fixed dose combination Cholib 145 mg/20 mg film-coated tablet and after co-administration of the separate 145 mg fenofibrate and 20 mg simvastatin tablets as used in the clinical program, were within the 80-125% bioequivalence interval.
Absorption: Maximum plasma concentrations (Cmax) of fenofibrate occur within 2 to 4 hours after oral administration. Plasma concentrations are stable during continuous treatment in any given individual.
Fenofibrate is water-insoluble and must be taken with food to facilitate absorption. The use of micronised fenofibrate and NanoCrystal technology for the formulation of the fenofibrate 145 mg tablet enhances its absorption.
Contrarily to previous fenofibrate formulations, the maximum plasma concentration and overall exposure of this formulation is independent from food intake.
A food-effect study involving administration of this formulation of fenofibrate 145 mg tablets to healthy male and female subjects under fasting conditions and with a high fat meal indicated that exposure (AUC and Cmax) to fenofibric acid is not affected by food.
Therefore, fenofibrate in Cholib 145 mg/20 mg film-coated tablet may be taken without regard to meals.
Kinetic studies following the administration of a single dose and continuous treatment have demonstrated that the drug does not accumulate.
Simvastatin is an inactive lactone which is readily hydrolyzed in vivo to the corresponding betahydroxyacid, a potent inhibitor of HMG-CoA reductase. Hydrolysis takes place mainly in the liver; the rate of hydrolysis in human plasma is very slow.
Simvastatin is well absorbed and undergoes extensive hepatic first-pass extraction. The extraction in the liver is dependent on the hepatic blood flow. The liver is the primary site of action of the active form. The availability of the beta-hydroxyacid to the systemic circulation following an oral dose of simvastatin was found to be less than 5% of the dose. Maximum plasma concentration of active inhibitors is reached approximately 1-2 hours after administration of simvastatin. Concomitant food intake does not affect the absorption.
The pharmacokinetics of single and multiple doses of simvastatin showed that no accumulation of medicinal product occurred after multiple dosing.
Distribution: Fenofibric acid is strongly bound to plasma albumin (more than 99%). The protein binding of simvastatin and its active metabolite is > 95%.
Biotransformation and Elimination: After oral administration, fenofibrate is rapidly hydrolyzed by esterases to the active metabolite fenofibric acid. No unchanged fenofibrate can be detected in the plasma. Fenofibrate is not a substrate for CYP 3A4. No hepatic microsomal metabolism is involved.
The drug is excreted mainly in the urine. Practically all the drug is eliminated within 6 days. Fenofibrate is mainly excreted in the form of fenofibric acid and its glucuronide conjugate. In elderly patients, the fenofibric acid apparent total plasma clearance is not modified.
Kinetic studies following the administration of a single dose and continuous treatment have demonstrated that the drug does not accumulate. Fenofibric acid is not eliminated by hemodialysis.
Mean plasma half-life: the plasma elimination half-life of fenofibric acid is approximately 20 hours.
Simvastatin is a substrate of CYP3A4 and of the efflux transporter BCRP. Simvastatin is taken up actively into the hepatocytes by the transporter OATP1B1. The major metabolites of simvastatin present in human plasma are the betahydroxyacid and four additional active metabolites. Following an oral dose of radioactive simvastatin to man, 13% of the radioactivity was excreted in the urine and 60% in the faeces within 96 hours. The amount recovered in the faeces represents absorbed medicinal product equivalents excreted in bile as well as unabsorbed medicinal product. Following an intravenous injection of the beta-hydroxyacid metabolite, its half-life averaged 1.9 hours. An average of only 0.3% of the intravenous dose was excreted in urine as inhibitors.
Effects of repeated administration of fenofibrate on the pharmacokinetics of single or multiple doses of simvastatin have been investigated in two small studies (n=12) followed by a larger one (n=85) in healthy subjects.
In one study the AUC of the simvastatin acid (SVA), a major active metabolite of simvastatin, was reduced by 42% (90% CI 24%-56%) when a single dose of 40 mg simvastatin was combined with repeated administration of fenofibrate 160 mg. In the other study [Bergman et al, 2004] repeated coadministration of both simvastatin 80 mg and fenofibrate 160 mg led to a reduction in the AUC of the SVA of 36% (90% CI 30%-42%). In the larger study a reduction of 21% (90% CI 14%-27%) in AUC of SVA was observed after repeated co-administration of simvastatin 40 mg and fenofibrate 145 mg in the evening. This was not significantly different from the 29% (90% CI 22%-35%) reduction in AUC of SVA observed when co-administration was 12 hours apart: simvastatin 40 mg in the evening and fenofibrate 145 mg in the morning.
Whether fenofibrate had an effect on other active metabolites of simvastatin was not investigated. The exact mechanism of interaction is not known. In the available clinical data, the effect on LDL-C reduction was not considered to be significantly different to simvastatin monotherapy when LDL-C is controlled at the time of initiating treatment.
The repeated administration of simvastatin 40 or 80 mg, the highest dose registered, did not affect the plasma levels of fenofibric acid at steady state.
Special populations: Carriers of the SLCO1B1 gene c.521T>C allele have lower OATP1B1 activity. The mean exposure (AUC) of the main active metabolite, simvastatin acid is 120% in heterozygote carriers (CT) of the C allele and 221% in homozygote (CC) carriers relative to that of patients who have the most common genotype (TT). The C allele has a frequency of 18% in the European population. In patients with SLCO1B1 polymorphism there is a risk of increased exposure of simvastatin, which may lead to an increased risk of rhabdomyolysis (see Precautions).
Toxicology: Preclinical safety data: No preclinical studies have been performed with the fixed dose combination Cholib 145 mg/20 mg film-coated tablet.
Fenofibrate: Acute toxicity studies have yielded no relevant information about specific toxicity of fenofibrate.
In a three-month oral nonclinical study in the rat species with fenofibric acid, the active metabolite of fenofibrate, toxicity for the skeletal muscles (particularly those rich in type I-slow oxidative-myofibres) and cardiac degeneration, anemia and decreased body weight were seen at exposure levels ≥50-fold the human exposure for the skeletal toxicity and >15 fold for the cardiomyotoxicity.
Reversible ulcers and erosions in the gastro-intestinal tract occurred in dogs treated during 3 months at exposures approximately 7-fold the clinical AUC.
Studies on mutagenicity of fenofibrate have been negative.
In rats and mice, liver tumours have been found in carcinogenicity studies, which are attributable to peroxisome proliferation. These changes are specific to rodents and have not been observed in other species at comparable dose levels. This is of no relevance to therapeutic use in man.
Studies in mice, rats and rabbits did not reveal any teratogenic effect. Embryotoxic effects were observed at doses in the range of maternal toxicity. Prolongation of the gestation period and difficulties during delivery were observed at high doses.
No effects on fertility were detected in non-clinical reproductive toxicity studies conducted with fenofibrate. However reversible hypospermia and testicular vacuolation and immaturity of the ovaries were observed in a repeat-dose toxicity study with fenofibric acid in young dogs.
Simvastatin: Based on conventional animal studies regarding pharmacodynamics, repeated dose toxicity, genotoxicity and carcinogenicity, there are no other risks for the patient than may be expected on account of the pharmacological mechanism. At maximally tolerated doses in both the rat and the rabbit, simvastatin produced no fetal malformations, and had no effects on fertility, reproductive function or neonatal development.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image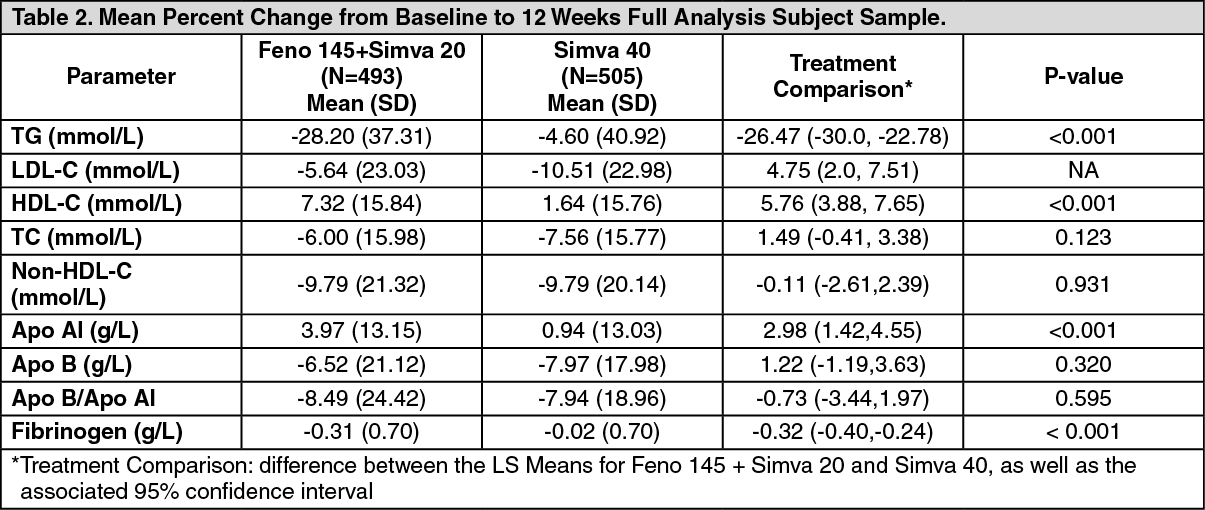 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
