


 Sign Out
Sign Out


Interactions relevant to monotherapies: Inhibitors of CYP 3A4: Simvastatin is a substrate of cytochrome P450 3A4.
Potent inhibitors of cytochrome P450 3A4 increase the risk of myopathy and rhabdomyolysis by increasing the concentration of HMG-CoA reductase inhibitory activity in plasma during simvastatin therapy. Such inhibitors include itraconazole, ketoconazole, posaconazole, erythromycin, clarithromycin, telithromycin, HIV protease inhibitors (e.g. nelfinavir), cobicistat and nefazodone.
Combination with itraconazole, ketoconazole, posaconazole, HIV protease inhibitors (e.g. nelfinavir), cobicistat, erythromycin, clarithromycin, telithromycin and nefazodone is contraindicated (see Contraindications). If treatment with itraconazole, ketoconazole, posaconazole, erythromycin, clarithromycin or telithromycin is unavoidable, therapy with Cholib 145 mg/20 mg film-coated tablet must be suspended during the course of treatment. Caution should be exercised when combining Cholib 145 mg/20 mg film-coated tablet with certain other less potent CYP 3A4 inhibitors: fluconazole, verapamil, or diltiazem (see Contraindications and Precautions).
Danazol: The risk of myopathy and rhabdomyolysis is increased by concomitant administration of danazol with simvastatin. The dose of simvastatin should not exceed 10 mg daily in patients taking danazol.
Therefore, the co-administration of Cholib 145 mg/20 mg film-coated tablets with danazol is contraindicated (see Contraindications).
Ciclosporin: The risk of myopathy/rhabdomyolysis is increased by concomitant administration of ciclosporin with simvastatin. Although the mechanism is not fully understood, ciclosporin has been shown to increase the plasma exposure (AUC) to simvastatin acid, presumably due in part to inhibition of CYP 3A4 and OATP-1B1 transporter. Because the dose of simvastatin should not exceed 10 mg daily in patients taking ciclosporin, the co-administration of Cholib 145 mg/20 mg tablet with ciclosporin is contraindicated (see Contraindications).
Amiodarone, amlodipine, diltiazem and verapamil: The risk of myopathy and rhabdomyolysis is increased by concomitant use of amiodarone, amlodipine, diltiazem or verapamil with simvastatin 40 mg per day.
In a clinical trial, myopathy was reported in 6% of patients receiving simvastatin 80 mg and amiodarone, versus 0.4% in patients on simvastatin 80 mg only.
Concomitant administration of amlodipine and simvastatin caused a 1.6-fold increase in exposure of simvastatin acid.
Concomitant administration of diltiazem and simvastatin caused a 2.7-fold increase in exposure of simvastatin acid, presumable due to inhibition of CYP 3A4.
Concomitant administration of verapamil and simvastatin resulted in a 2.3-fold increase in plasma exposure to simvastatin acid, presumably due, in part, to inhibition of CYP 3A4.
Therefore, the dose of Cholib 145 mg/20 mg film-coated tablet should not exceed 145 mg/20 mg daily in patients taking amiodarone, amlodipine, diltiazem or verapamil.
Inhibitors of Breast Cancer Resistant Protein (BCRP): Concomitant administration of medicinal products that are inhibitors of BCRP, including products containing elbasvir or grazoprevir, may lead to increased plasma concentrations of simvastatin and an increased risk of myopathy (see Precautions).
Other statins and fibrates: Gemfibrozil increases the AUC of simvastatin acid by 1.9-fold, possibly due to inhibition of the glucuronidation pathway. The risk of myopathy and rhabdomyolysis is significantly increased by concomitant use of gemfibrozil with simvastatin. The risk of rhabdomyolysis is also increased in patients concomitantly receiving other fibrates or statins. Therefore, the co-administration of Cholib 145 mg/20 mg tablet with gemfibrozil, other fibrates, or statins is contraindicated (see Contraindications).
Niacin (nicotinic acid): Cases of myopathy/rhabdomyolysis have been associated with concomitant administration of statins and niacin (nicotinic acid) at lipid-modifying doses (≥ 1 g/day), knowing that niacin and statins can cause myopathy when given alone.
Physicians contemplating combined therapy with Cholib 145 mg/20 mg film-coated tablet and lipid-modifying doses (≥ 1 g/day) of niacin (nicotinic acid) or medicinal products containing niacin should carefully weigh the potential benefits and risks and should carefully monitor patients for any signs and symptoms of muscle pain, tenderness, or weakness, particularly during the initial months of therapy and when the dose of either medicinal product is increased.
Fusidic acid: The risk of myopathy including rhabdomyolysis may be increased by the concomitant administration of systemic fusidic acid with statins. Co-administration of this combination may cause increased plasma concentrations of both agents. The mechanism of this interaction (whether it is pharmacodynamics or pharmacokinetic, or both) is yet unknown. There have been reports of rhabdomyolysis (including some fatalities) in patients receiving this combination.
If treatment with fusidic acid is necessary, Cholib 145 mg/20 mg film-coated tablet treatment should be discontinued throughout the duration of the fusidic acid treatment. (Also see Precautions).
Grapefruit juice: Grapefruit juice inhibits CYP 3A4. Concomitant intake of large quantities (over 1 liter daily) of grapefruit juice and simvastatin resulted in a 7-fold increase in plasma exposure to simvastatin acid. Intake of 240 mL of grapefruit juice in the morning and simvastatin in the evening also resulted in a 1.9-fold increase in plasma exposure to simvastatin acid. Intake of grapefruit juice during treatment with Cholib should therefore be avoided.
Colchicine: There have been reports of myopathy and rhabdomyolysis with the concomitant administration of colchicine and simvastatin in patients with renal insufficiency. Therefore, close clinical monitoring of such patients taking colchicine and Cholib 145 mg/20 mg film-coated tablet is advised.
Vitamin K antagonists: Fenofibrate and simvastatin enhance effects of Vitamin K antagonists and may increase the risk of bleeding. It is recommended that the dose of those oral anticoagulants is reduced by about one third at the start of treatment and then gradually adjusted if necessary according to INR (International Normalised Ratio) monitoring. INR should be determined before starting Cholib and frequently enough during early therapy to ensure that no significant alteration of INR occurs. Once a stable INR has been documented, it can be monitored at the intervals usually recommended for patients on those oral anticoagulants. If the dose of Cholib 145 mg/20 mg film-coated tablet is changed or discontinued, the same procedure should be repeated. Cholib 145 mg/20 mg film-coated tablet therapy has not been associated with bleeding in patients not taking anticoagulants.
Glitazones: Some cases of reversible paradoxical reduction of HDL-C have been reported during concomitant administration of fenofibrate and glitazones. Therefore it is recommended to monitor HDL-C if Cholib 145 mg/20 mg tablet is co-administered with a glitazone and stopping either therapy if HDL-C is too low.
Rifampicin: Because rifampicin is a potent CYP 3A4 inducer that interferes with simvastatin metabolism, patients undertaking long-term rifampicin therapy (e.g. treatment of tuberculosis) may experience loss of efficacy of simvastatin. In normal volunteers, the plasma exposure to simvastatin acid was decreased by 93% with concomitant administration of rifampicin.
Effects on the pharmacokinetics of other medicinal products: Fenofibrate and simvastatin are not CYP 3A4 inhibitors or inducers. Therefore, Cholib 145 mg/20 mg film-coated tablet is not expected to affect plasma concentrations of substances metabolised via CYP 3A4.
Fenofibrate and simvastatin are not inhibitors of CYP 2D6, CYP 2E1, or CYP 1A2. Fenofibrate is a mild to moderate inhibitor of CYP 2C9 and a weak inhibitor of CYP 2C19 and CYP 2A6.
Patients receiving co-administration of Cholib 145 mg/20 mg film-coated tablet and drugs metabolised by CYP 2C19, CYP 2A6, or especially CYP 2C9 with a narrow therapeutic index should be carefully monitored and, if necessary, dose adjustment of these drugs is recommended.
Interaction between simvastatin and fenofibrate: Effects of repeated administration of fenofibrate on the pharmacokinetics of single or multiple doses of simvastatin have been investigated in two small studies (n=12) followed by a larger one (n= 85) in healthy subjects.
In one study the AUC of the simvastatin acid (SVA), a major active metabolite of simvastatin, was reduced by 42% (90% CI 24%-56%) when a single dose of 40 mg simvastatin was combined with repeated administration of fenofibrate 160 mg. In the other study [Bergman et al, 2004] repeated coadministration of both simvastatin 80 mg and fenofibrate 160 mg led to a reduction in the AUC of the SVA of 36% (90% CI 30%-42%). In the larger study a reduction of 21% (90% CI 14%-27%) in AUC of SVA was observed after repeated co-administration of simvastatin 40 mg and fenofibrate 145 mg in the evening. This was not significantly different from the 29% (90% CI 22%-35%) reduction in AUC of SVA observed when co-administration was 12 hours apart: simvastatin 40 mg in the evening and fenofibrate 145 mg in the morning.
Whether fenofibrate had an effect on other active metabolites of simvastatin was not investigated. The exact mechanism of interaction is not known. In the available clinical data, the effect on LDL-C reduction was not considered to be significantly different to simvastatin monotherapy when LDL-C is controlled at the time of initiating treatment.
The repeated administration of simvastatin 40 or 80 mg, the highest dose registered, did not affect the plasma levels of fenofibric acid at steady state.
Prescribing recommendations for interacting substances are summarised in the table as follows (see also Dosage & Administration and Contraindications). (See Table 5.)
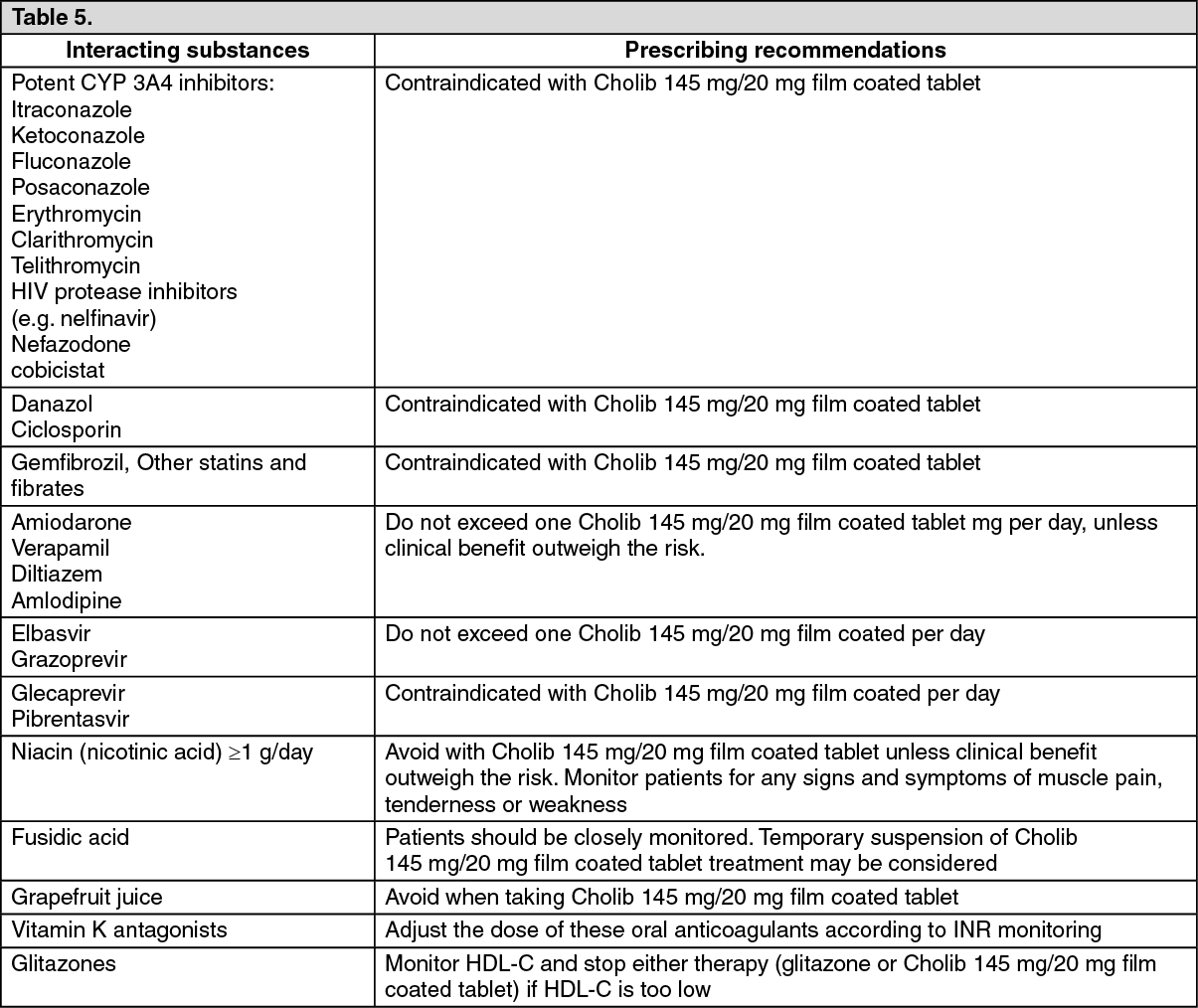 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image