


 Sign Out
Sign Out

The rationale of ALDURAZYME therapy in MPS I is to provide exogenous enzyme for uptake into lysosomes and increase the catabolism of GAG. ALDURAZYME uptake by cells into lysosomes is most likely mediated by the mannose-6-phosphate-terminated oligosaccharide chains of laronidase binding to specific mannose-6-phosphate receptors.
Because many proteins in the blood are restricted from entry into the central nervous system (CNS) by the blood brain barrier, effects of intravenously administered ALDURAZYME on cells within the CNS cannot be inferred from activity in sites outside the CNS. The ability of ALDURAZYME to cross the blood brain barrier has not been evaluated in animal models or in clinical studies.
Pharmacodynamics: The pharmacodynamic effect of ALDURAZYME was assessed by reductions in urinary GAG levels. The responsiveness of urinary GAG to dosage alterations of ALDURAZYME is unknown, and the relationship of urinary GAG to other measures of clinical response has also not been established (see Clinical Studies as follows).
Clinical Studies: Clinical Studies in Patients 6 Years and Older: Study 1 was a randomized, double-blind, placebo-controlled study in 45 patients with MPS I, ages 6 to 43 years old, including 1 patient with the Hurler form, 37 patients with Hurler-Scheie form, and 7 patients with Scheie form of MPS I. All patients had a baseline percent predicted forced vital capacity (FVC) less than or equal to 77%. Patients received ALDURAZYME at 0.58 mg/kg of body weight once weekly or placebo once weekly for 26 weeks. All patients were treated with antipyretics and antihistamines prior to each infusion.
The primary efficacy outcome assessments were percent predicted FVC and distance walked in 6 minutes (6-minute walk test). After 26 weeks, patients treated with ALDURAZYME showed improvement in percent predicted FVC and in 6-minute walk test compared to placebo-treated patients (see Table 1).
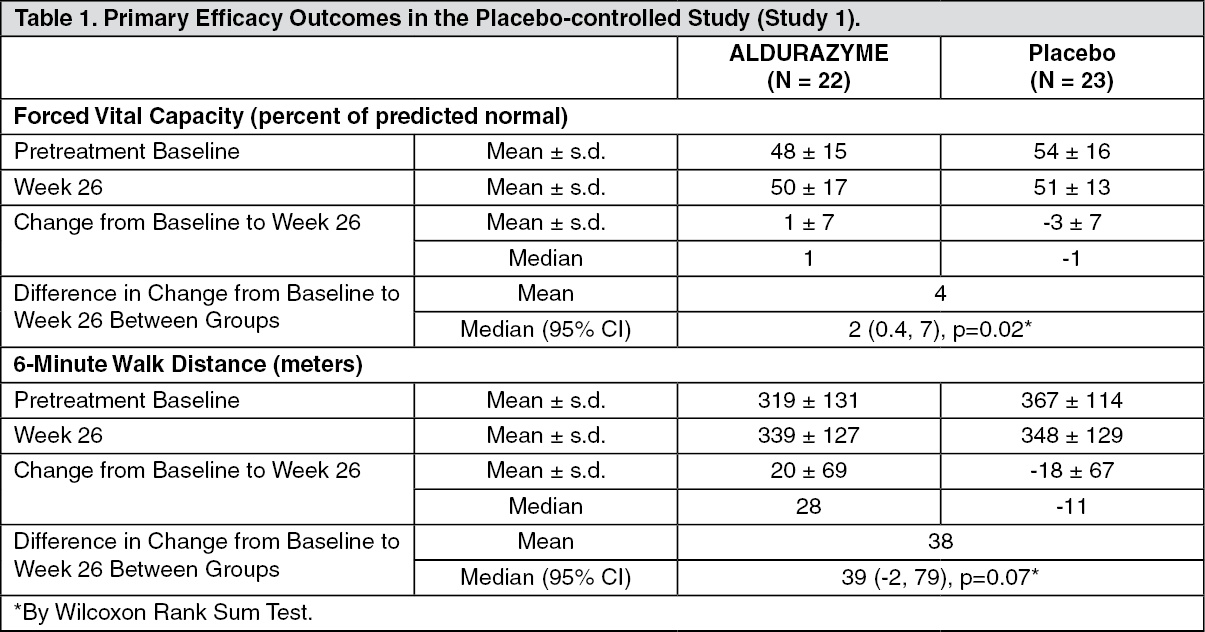 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEvaluations of bioactivity were changes in liver size and urinary GAG levels. Liver size and urinary GAG levels decreased in patients treated with ALDURAZYME compared to patients treated with placebo. No patient in the group receiving ALDURAZYME reached the normal range for urinary GAG levels during this 6-month study.
Study 2 was a 182-week, open-label, uncontrolled extension study of all 45 patients who completed Study 1. Patients received ALDURAZYME at 0.58 mg/kg body weight once weekly. For patients treated with ALDURAZYME, the mean increase in 6-minute walk test distance was maintained for an additional 182 weeks through completion of Study 2.
At the end of Study 2, the decrease in the mean urinary GAG was similar to the decrease in urinary GAG reported in ALDURAZYME treated patients at the end of Study 1. The relationship of urinary GAG to other measures of clinical response has not been established.
Clinical Studies in Patients 6 Years and Younger: Study 3 was a 52-week, open-label, uncontrolled clinical study in 20 patients with MPS I, ages 6 months to 5 years old (at enrollment), including 16 patients (80%) with the Hurler form and 4 patients (20%) with the Hurler-Scheie form. All 20 patients received ALDURAZYME at 0.58 mg/kg of body weight once weekly for 26 weeks. After 26 weeks of treatment, 16 patients continued to receive 0.58 mg/kg of body weight once weekly through Week 52, and 4 patients received 1.16 mg/kg of body weight once weekly from Week 26 through Week 52.
Pharmacokinetics: The pharmacokinetics of laronidase were evaluated in 6-year-old or older patients (N = 10 to 12) with MPS I who received 0.58 mg/kg of body weight once weekly of ALDURAZYME as a 4-hour infusion in the placebo-controlled clinical study (Study 1). After the 1st, 12th and 26th weekly infusions, the mean maximum plasma concentrations (Cmax) ranged from 1.2 to 1.7 mcg/mL for the 3 time points. The mean area under the plasma concentration-time curve (AUC∞) ranged from 4.5 to 6.9 μg·hour/mL. The mean volume of distribution (Vz) ranged from 0.24 to 0.60 L/kg. Mean plasma clearance (CL) ranged from 1.7 to 2.7 mL/min/kg, and the mean elimination half-life (t½) ranged from 1.5 to 3.6 hours.
Most patients who received once-weekly infusions of ALDURAZYME in Study 1 developed antibodies to laronidase by Week 12. Between Weeks 1 and 12, increases in the plasma clearance of laronidase were observed in some patients and appeared to be proportional to the antibody titer. At Week 26, plasma clearance of laronidase was comparable to that at Week 1, in spite of the continued and, in some cases, increased titers of antibodies.
The pharmacokinetics of laronidase were evaluated in 6-year-old or younger patients (N = 7 to 9) with MPS I disease who received 0.58 mg/kg of body weight once weekly of ALDURAZYME as a 4-hour infusion in the open label clinical study (Study 3). After the 26th infusion, the 95% confidence interval of the geometric mean values of PK parameters ranged from 0.6 to 1.6 mcg/mL for the maximum plasma concentrations (Cmax), from 1.3 to 4.4 μg·hour/mL for area under the plasma concentration-time curve (AUC∞), from 0.12 to 0.56 L/kg for volume of distribution (Vz), from 2.2 to 7.7 mL/min/kg for plasma clearance (CL), and from 0.3 to 1.9 hours for elimination half-life (t½).
Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Studies to assess the mutagenic and carcinogenic potential of laronidase have not been conducted.
Laronidase at intravenous doses up to 3.6 mg/kg (6.2 times the recommended human dose) was found to have no effect on the fertility and reproductive performance of male and female rats.