


 Sign Out
Sign Out

Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, the adverse reaction rates observed cannot be directly compared to rates in other trials and may not reflect the rates observed in clinical practice.
Hormone Receptor-Positive, HER2-Negative Breast Cancer: The safety of AFINITOR (10 mg orally once daily) in combination with exemestane (25 mg orally once daily) (n = 485) vs. placebo in combination with exemestane (n = 239) was evaluated in a randomized, controlled trial (BOLERO-2) in patients with advanced or metastatic hormone receptor-positive, HER2-negative breast cancer. The median age of patients was 61 years (28 to 93 years), and 75% were White. The median follow-up was approximately 13 months.
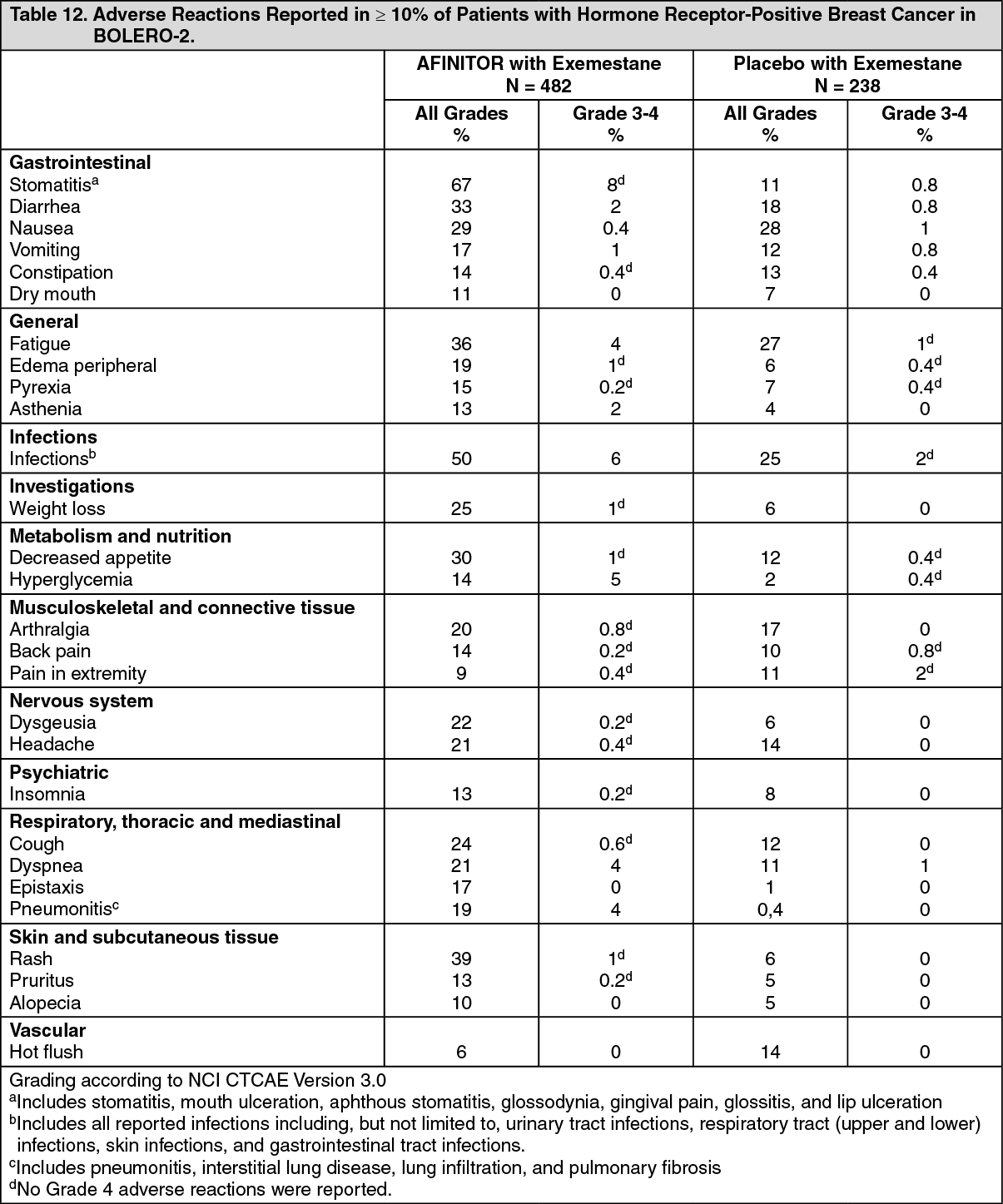
The most common adverse reactions (incidence ≥ 30%) were stomatitis, infections, rash, fatigue, diarrhea, and decreased appetite. The most common Grade 3-4 adverse reactions (incidence ≥ 2%) were stomatitis, infections, hyperglycemia, fatigue, dyspnea, pneumonitis, and diarrhea. The most common laboratory abnormalities (incidence ≥ 50%) were hypercholesterolemia, hyperglycemia, increased aspartate transaminase (AST), anemia, leukopenia, thrombocytopenia, lymphopenia, increased alanine transaminase (ALT), and hypertriglyceridemia. The most common Grade 3-4 laboratory abnormalities (incidence ≥ 3%) were lymphopenia, hyperglycemia, anemia, hypokalemia, increased AST, increased ALT, and thrombocytopenia.
Fatal adverse reactions occurred in 2% of patients who received AFINITOR. The rate of adverse reactions resulting in permanent discontinuation was 24% for the AFINITOR arm. Dose adjustments (interruptions or reductions) occurred in 63% of patients in the AFINITOR arm.
Adverse reactions reported with an incidence of ≥ 10% for patients receiving AFINITOR vs. placebo are presented in Table 12. Laboratory abnormalities are presented in Table 13. The median duration of treatment with AFINITOR was 23.9 weeks; 33% were exposed to AFINITOR for a period of ≥ 32 weeks. (See Tables 12 and 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image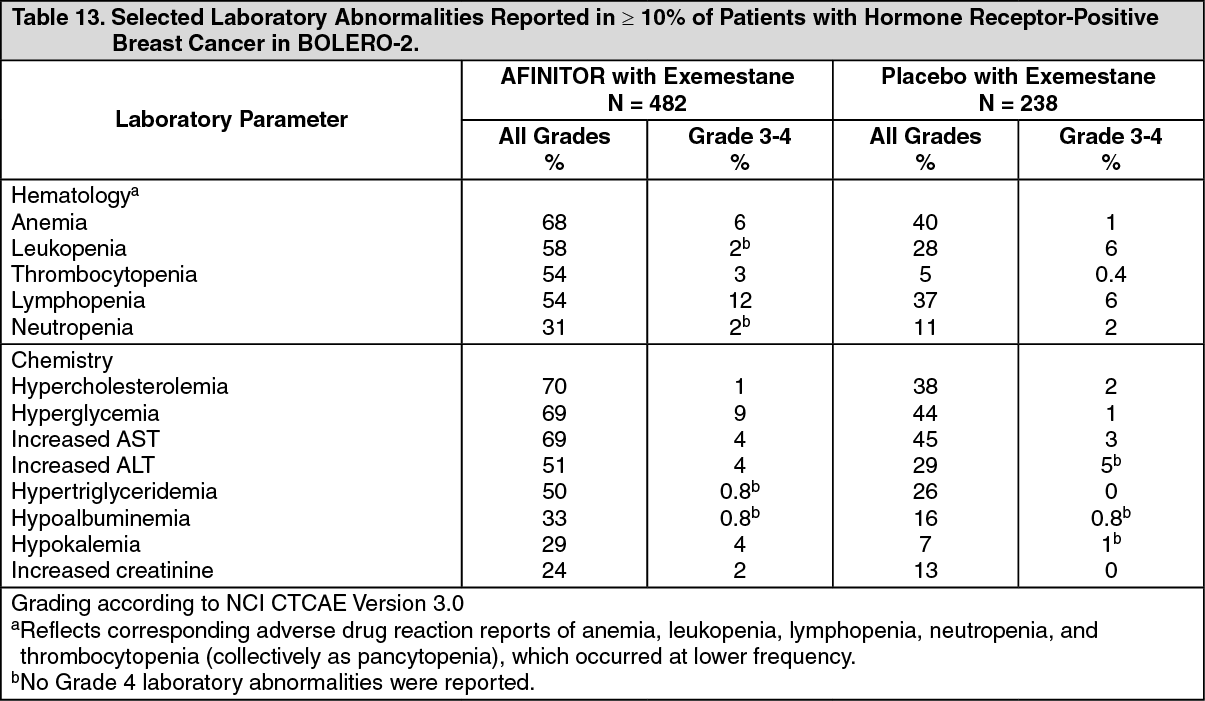 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTopical Prophylaxis for Stomatitis: In a single arm study (SWISH; N = 92) in postmenopausal women with hormone receptor-positive, HER2-negative breast cancer beginning AFINITOR (10 mg orally once daily) in combination with exemestane (25 mg orally once daily), patients started dexamethasone 0.5 mg/5 mL alcohol-free mouthwash (10 mL swished for 2 minutes and spat, 4 times daily for 8 weeks) concurrently with AFINITOR and exemestane. No food or drink was to be consumed for at least 1 hour after swishing and spitting the dexamethasone mouthwash. The primary objective of this study was to assess the incidence of Grade 2 to 4 stomatitis within 8 weeks. The incidence of Grade 2 to 4 stomatitis within 8 weeks was 2%, which was lower than the 33% reported in the BOLERO-2 trial. The incidence of Grade 1 stomatitis was 19%. No cases of Grade 3 or 4 stomatitis were reported. Oral candidiasis was reported in 2% of patients in this study compared to 0.2% in the BOLERO-2 trial.
Coadministration of AFINITOR and dexamethasone alcohol-free oral solution has not been studied in pediatric patients.
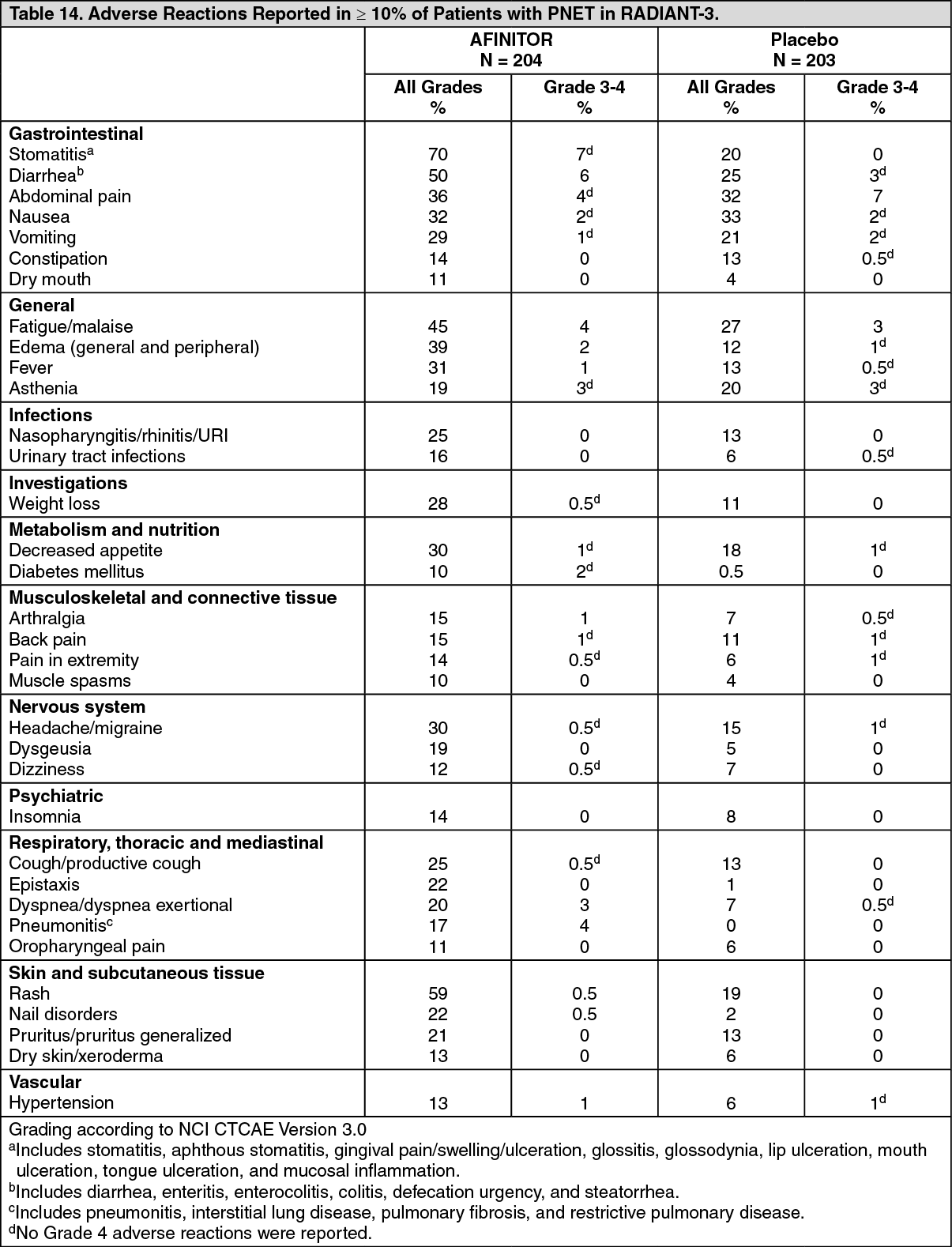
Pancreatic Neuroendocrine Tumors (PNET): In a randomized, controlled trial (RADIANT-3) of AFINITOR (n = 204) vs. placebo (n = 203) in patients with advanced PNET the median age of patients was 58 years (20 to 87 years), 79% were White, and 55% were male. Patients on the placebo arm could cross over to open-label AFINITOR upon disease progression.
The most common adverse reactions (incidence ≥ 30%) were stomatitis, rash, diarrhea, fatigue, edema, abdominal pain, nausea, fever, and headache. The most common Grade 3-4 adverse reactions (incidence ≥ 5%) were stomatitis and diarrhea. The most common laboratory abnormalities (incidence ≥ 50%) were anemia, hyperglycemia, increased alkaline phosphatase, hypercholesterolemia, decreased bicarbonate, and increased AST. The most common Grade 3-4 laboratory abnormalities (incidence ≥ 3%) were hyperglycemia, lymphopenia, anemia, hypophosphatemia, increased alkaline phosphatase, neutropenia, increased AST, hypokalemia, and thrombocytopenia.
Deaths during double-blind treatment where an adverse reaction was the primary cause occurred in seven patients on AFINITOR. Causes of death on the AFINITOR arm included one case of each of the following: acute renal failure, acute respiratory distress, cardiac arrest, death (cause unknown), hepatic failure, pneumonia, and sepsis. After cross-over to open-label AFINITOR, there were three additional deaths, one due to hypoglycemia and cardiac arrest in a patient with insulinoma, one due to myocardial infarction with congestive heart failure, and the other due to sudden death. The rate of adverse reactions resulting in permanent discontinuation was 20% for the AFINITOR group. Dose delay or reduction was necessary in 61% of AFINITOR patients. Grade 3-4 renal failure occurred in six patients in the AFINITOR arm. Thrombotic events included five patients with pulmonary embolus in the AFINITOR arm as well as three patients with thrombosis in the AFINITOR arm.
Table 14 compares the incidence of adverse reactions reported with an incidence of ≥ 10% for patients receiving AFINITOR vs. placebo. Laboratory abnormalities are summarized in Table 15. The median duration of treatment in patients who received AFINITOR was 37 weeks.
In female patients aged 18 to 55 years, irregular menstruation occurred in 5 of 46 (11%) AFINITOR-treated females. (See Tables 14 and 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image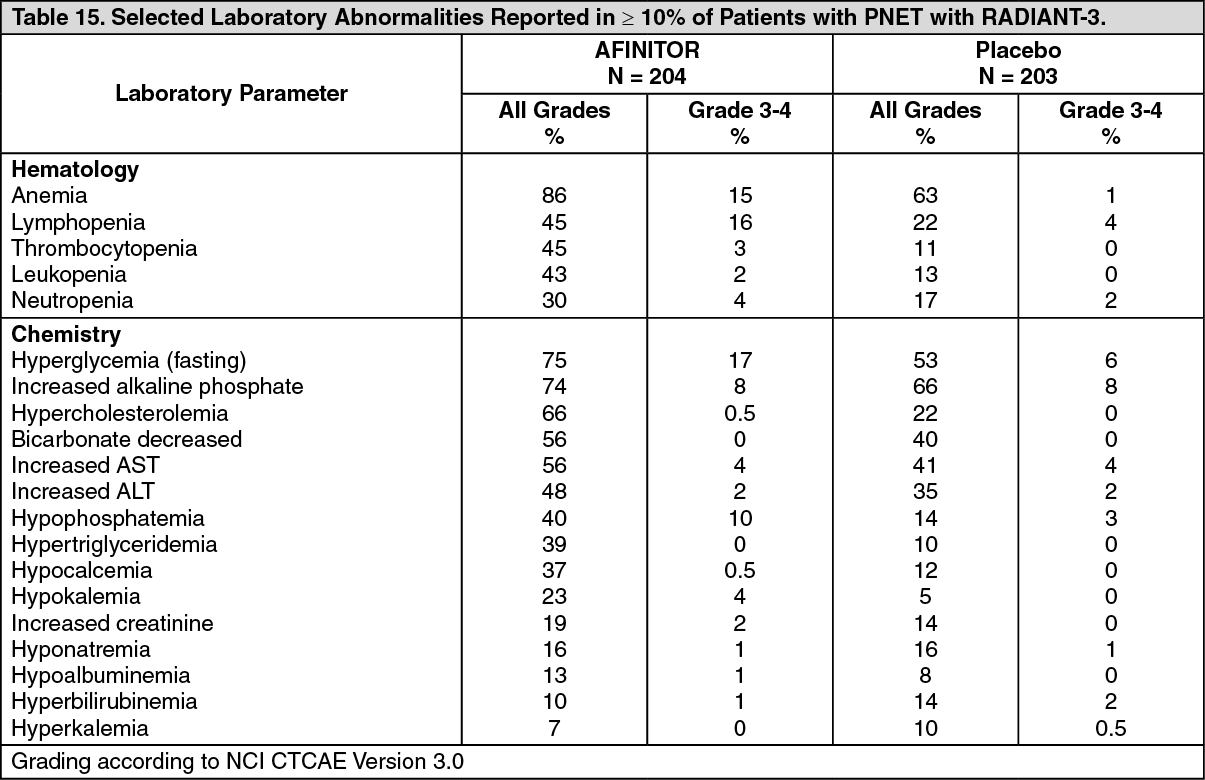 Click on icon to see table/diagram/image
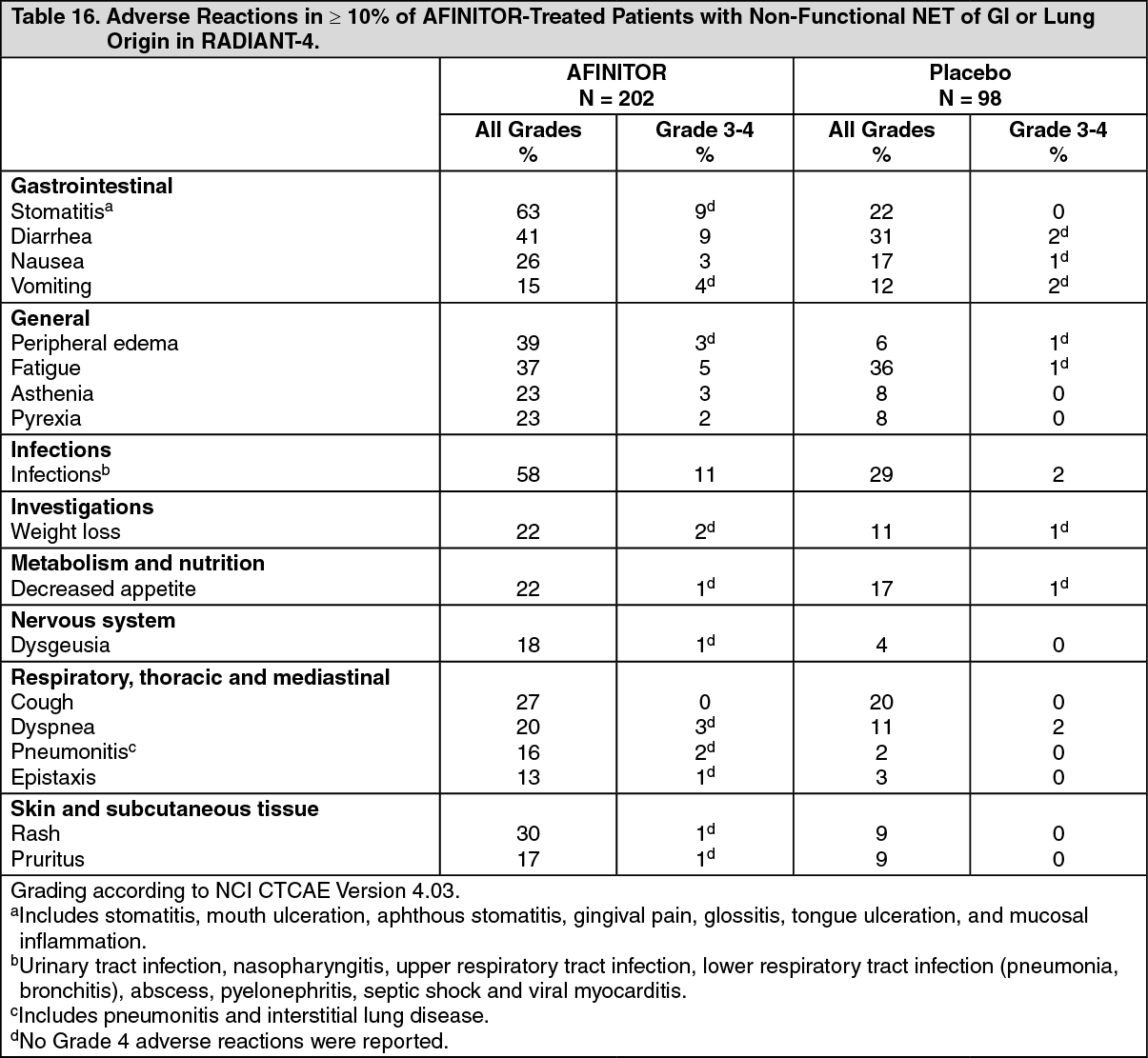
Click on icon to see table/diagram/imageNeuroendocrine Tumors (NET) of Gastrointestinal (GI) or Lung Origin: In a randomized, controlled trial (RADIANT-4) of AFINITOR (n = 202 treated) vs. placebo (n = 98 treated) in patients with advanced non-functional NET of GI or lung origin, the median age of patients was 63 years (22-86 years), 76% were White, and 53% were female. The median duration of exposure to AFINITOR was 9.3 months; 64% of patients were treated for > 6 months and 39% were treated for > 12 months. AFINITOR was discontinued for adverse reactions in 29% of patients, dose reduction or delay was required in 70% of AFINITOR-treated patients.
Serious adverse reactions occurred in 42% of AFINITOR-treated patients and included 3 fatal events (cardiac failure, respiratory failure, and septic shock). Adverse reactions occurring at an incidence of ≥ 10% and at ≥ 5% absolute incidence over placebo (all Grades) or ≥ 2% higher incidence over placebo (Grade 3 and 4) are presented in Table 16. Laboratory abnormalities are presented in Table 17. (See Tables 16 and 17.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image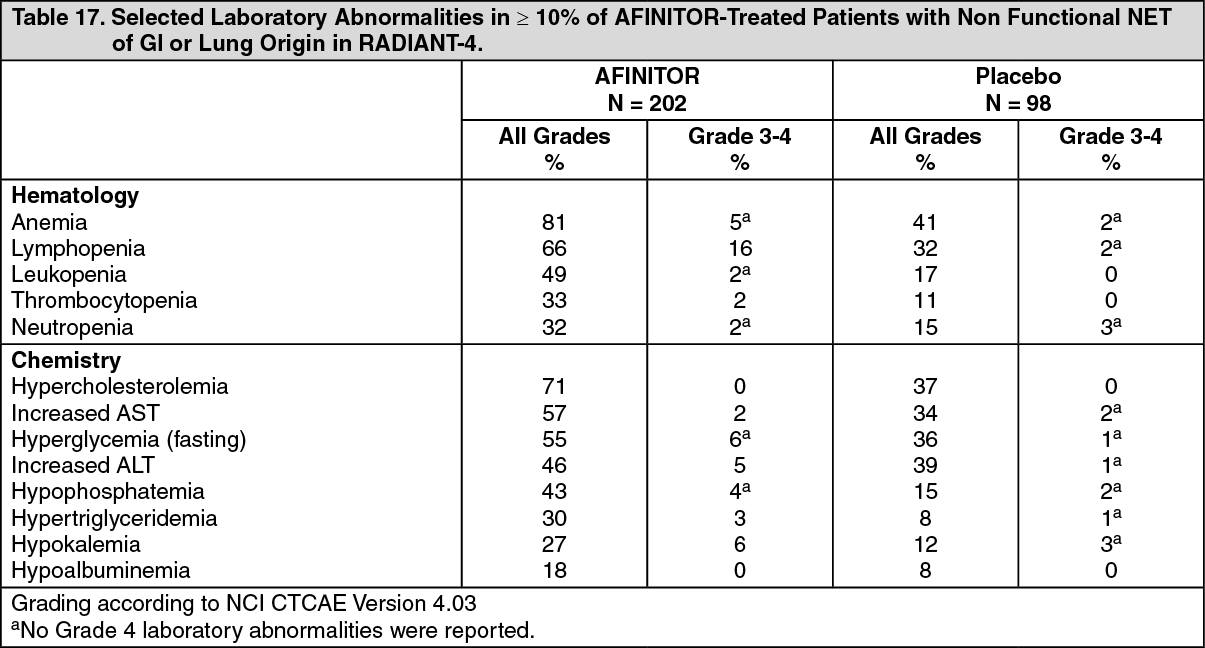 Click on icon to see table/diagram/image
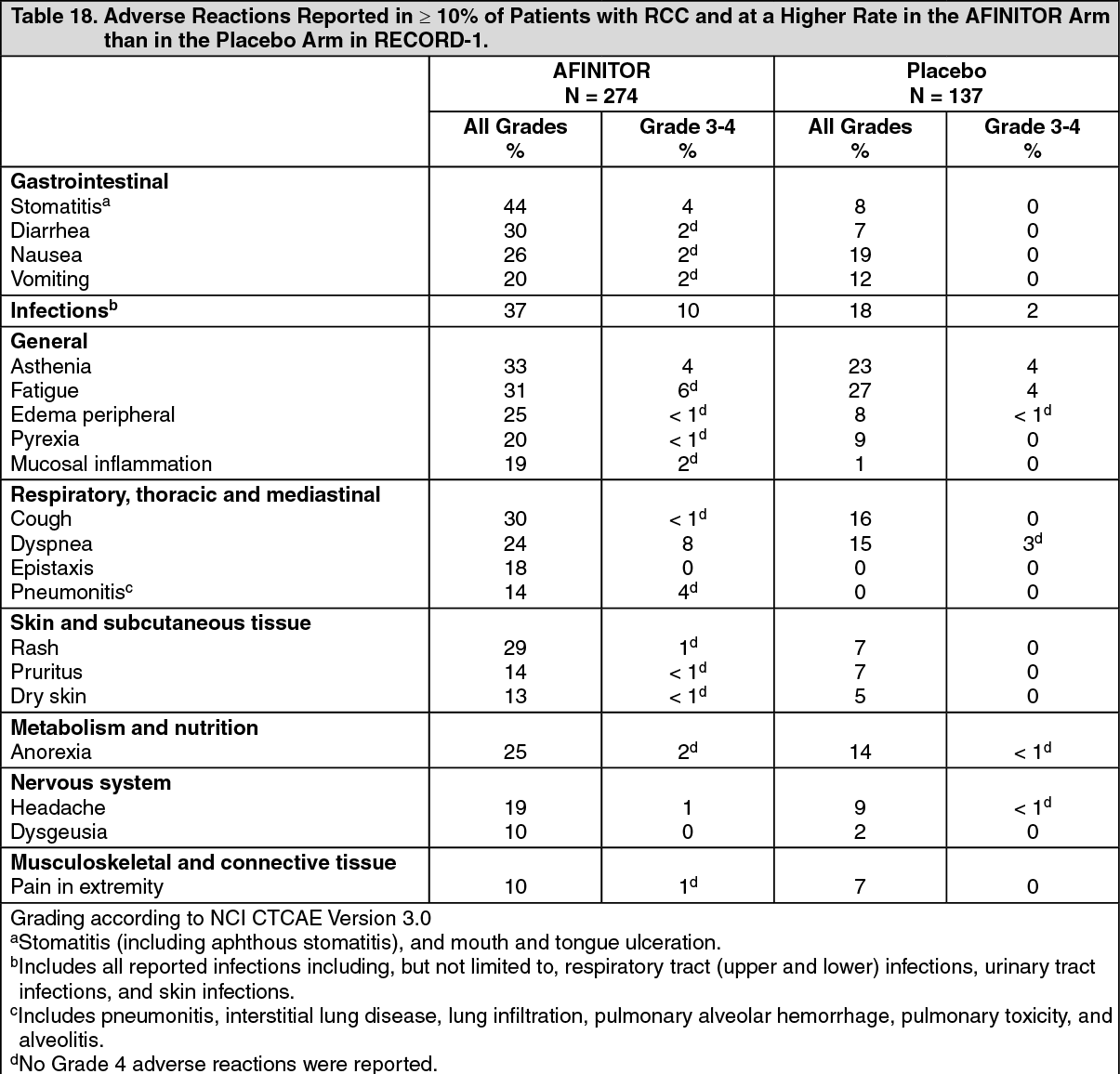
Click on icon to see table/diagram/imageRenal Cell Carcinoma (RCC): The data described as follows reflect exposure to AFINITOR (n = 274) and placebo (n = 137) in a randomized, controlled trial (RECORD-1) in patients with metastatic RCC who received prior treatment with sunitinib and/or sorafenib. The median age of patients was 61 years (27 to 85 years), 88% were White, and 78% were male. The median duration of blinded study treatment was 141 days (19 to 451 days) for patients receiving AFINITOR.
The most common adverse reactions (incidence ≥ 30%) were stomatitis, infections, asthenia, fatigue, cough, and diarrhea. The most common Grade 3-4 adverse reactions (incidence ≥ 3%) were infections, dyspnea, fatigue, stomatitis, dehydration, pneumonitis, abdominal pain, and asthenia. The most common laboratory abnormalities (incidence ≥ 50%) were anemia, hypercholesterolemia, hypertriglyceridemia, hyperglycemia, lymphopenia, and increased creatinine. The most common Grade 3-4 laboratory abnormalities (incidence ≥ 3%) were lymphopenia, hyperglycemia, anemia, hypophosphatemia, and hypercholesterolemia.
Deaths due to acute respiratory failure (0.7%), infection (0.7%), and acute renal failure (0.4%) were observed on the AFINITOR arm. The rate of adverse reactions resulting in permanent discontinuation was 14% for the AFINITOR group. The most common adverse reactions leading to treatment discontinuation were pneumonitis and dyspnea. Infections, stomatitis, and pneumonitis were the most common reasons for treatment delay or dose reduction. The most common medical interventions required during AFINITOR treatment were for infections, anemia, and stomatitis.
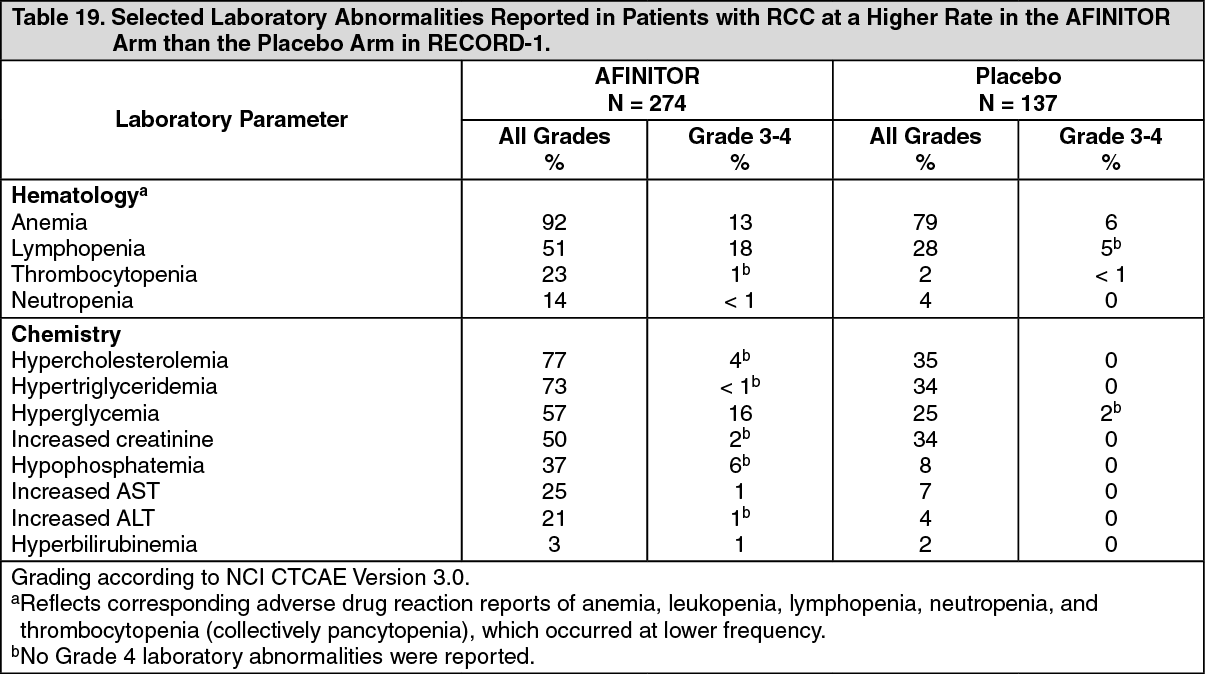
Adverse reactions reported with an incidence of ≥ 10% for patients receiving AFINITOR vs. placebo are presented in Table 18. Laboratory abnormalities are presented in Table 19. (See Table 18.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOther notable adverse reactions occurring more frequently with AFINITOR than with placebo, but with an incidence of < 10% include: Gastrointestinal: Abdominal pain (9%), dry mouth (8%), hemorrhoids (5%), dysphagia (4%).
General: Weight loss (9%), chest pain (5%), chills (4%), impaired wound healing (< 1%).
Respiratory, thoracic and mediastinal: Pleural effusion (7%), pharyngolaryngeal pain (4%), rhinorrhea (3%).
Skin and subcutaneous tissue: Hand-foot syndrome (reported as palmar-plantar erythrodysesthesia syndrome) (5%), nail disorder (5%), erythema (4%), onychoclasis (4%), skin lesion (4%), acneiform dermatitis (3%), angioedema (< 1%).
Metabolism and nutrition: Exacerbation of pre-existing diabetes mellitus (2%), new onset of diabetes mellitus (< 1%).
Psychiatric: Insomnia (9%).
Nervous system: Dizziness (7%), paresthesia (5%).
Ocular: Eyelid edema (4%), conjunctivitis (2%).
Vascular: Hypertension (4%), deep vein thrombosis (< 1%).
Renal and urinary: Renal failure (3%).
Cardiac: Tachycardia (3%), congestive cardiac failure (1%).
Musculoskeletal and connective tissue: Jaw pain (3%).
Hematologic: Hemorrhage (3%). (See Table 19.)
 Click on icon to see table/diagram/image
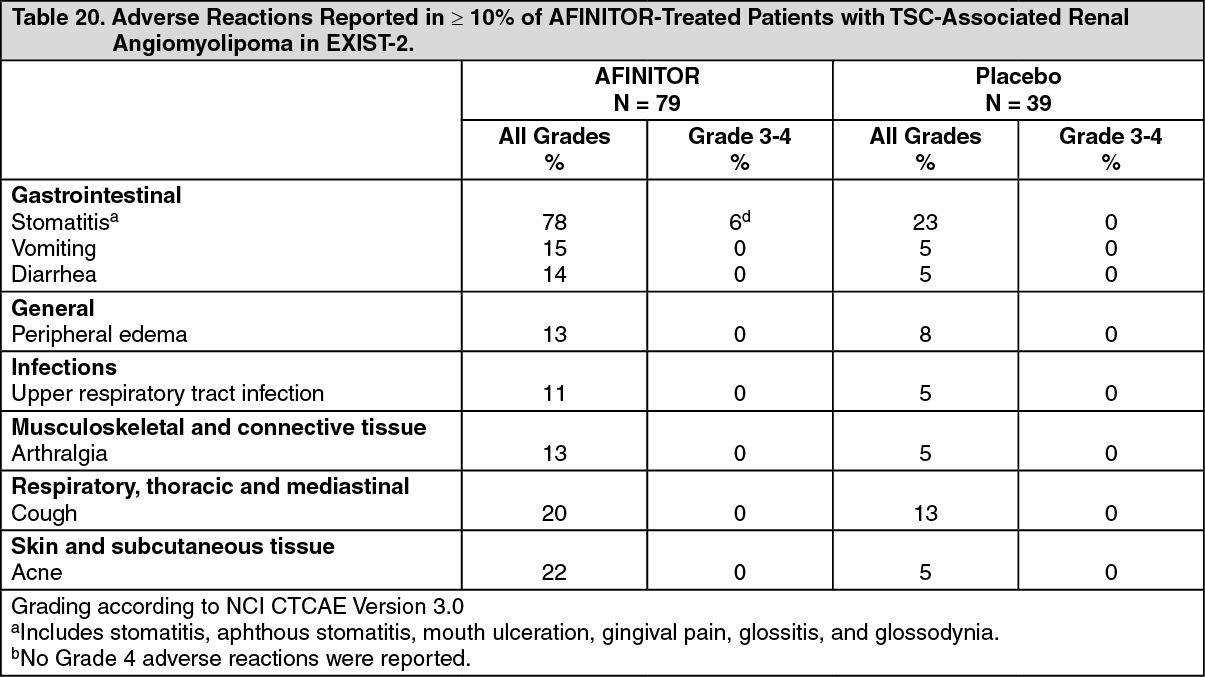
Click on icon to see table/diagram/imageTuberous Sclerosis Complex (TSC)-Associated Renal Angiomyolipoma: The data described as follows are based on a randomized (2:1), double-blind, placebo-controlled trial (EXIST-2) of AFINITOR in 118 patients with renal angiomyolipoma as a feature of TSC (n = 113) or sporadic lymphangioleiomyomatosis (n = 5). The median age of patients was 31 years (18 to 61 years), 89% were White, and 34% were male. The median duration of blinded study treatment was 48 weeks (2 to 115 weeks) for patients receiving AFINITOR.
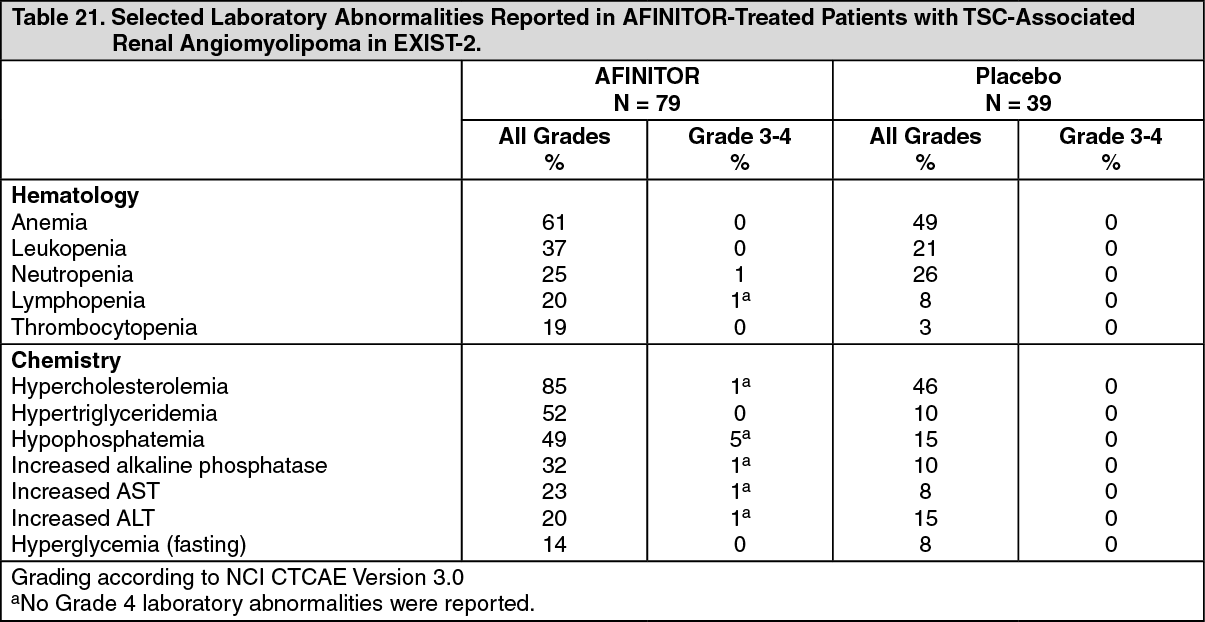
The most common adverse reaction reported for AFINITOR (incidence ≥ 30%) was stomatitis. The most common Grade 3-4 adverse reactions (incidence ≥ 2%) were stomatitis and amenorrhea. The most common laboratory abnormalities (incidence ≥ 50%) were hypercholesterolemia, hypertriglyceridemia, and anemia. The most common Grade 3-4 laboratory abnormality (incidence ≥ 3%) was hypophosphatemia.
The rate of adverse reactions resulting in permanent discontinuation was 3.8% in the AFINITOR-treated patients. Adverse reactions leading to permanent discontinuation in the AFINITOR arm were hypersensitivity/angioedema/bronchospasm, convulsion, and hypophosphatemia. Dose adjustments (interruptions or reductions) due to adverse reactions occurred in 52% of AFINITOR-treated patients. The most common adverse reaction leading to AFINITOR dose adjustment was stomatitis.
Adverse reactions reported with an incidence of ≥ 10% for patients receiving AFINITOR and occurring more frequently with AFINITOR than with placebo are presented in Table 20. Laboratory abnormalities are presented in Table 21. (See Table 20.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAmenorrhea occurred in 15% of AFINITOR-treated females (8 of 52). Other adverse reactions involving the female reproductive system were menorrhagia (10%), menstrual irregularities (10%), and vaginal hemorrhage (8%).
The following additional adverse reactions occurred in less than 10% of AFINITOR-treated patients: epistaxis (9%), decreased appetite (6%), otitis media (6%), depression (5%), abnormal taste (5%), increased blood luteinizing hormone (LH) levels (4%), increased blood follicle stimulating hormone (FSH) levels (3%), hypersensitivity (3%), ovarian cyst (3%), pneumonitis (1%), and angioedema (1%). (See Table 21.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageUpdated safety information from 112 patients treated with AFINITOR for a median duration of 3.9 years identified the following additional adverse reactions and selected laboratory abnormalities: increased partial thromboplastin time (63%), increased prothrombin time (40%), decreased fibrinogen (38%), urinary tract infection (31%), proteinuria (18%), abdominal pain (16%), pruritus (12%), gastroenteritis (12%), myalgia (11%), and pneumonia (10%).
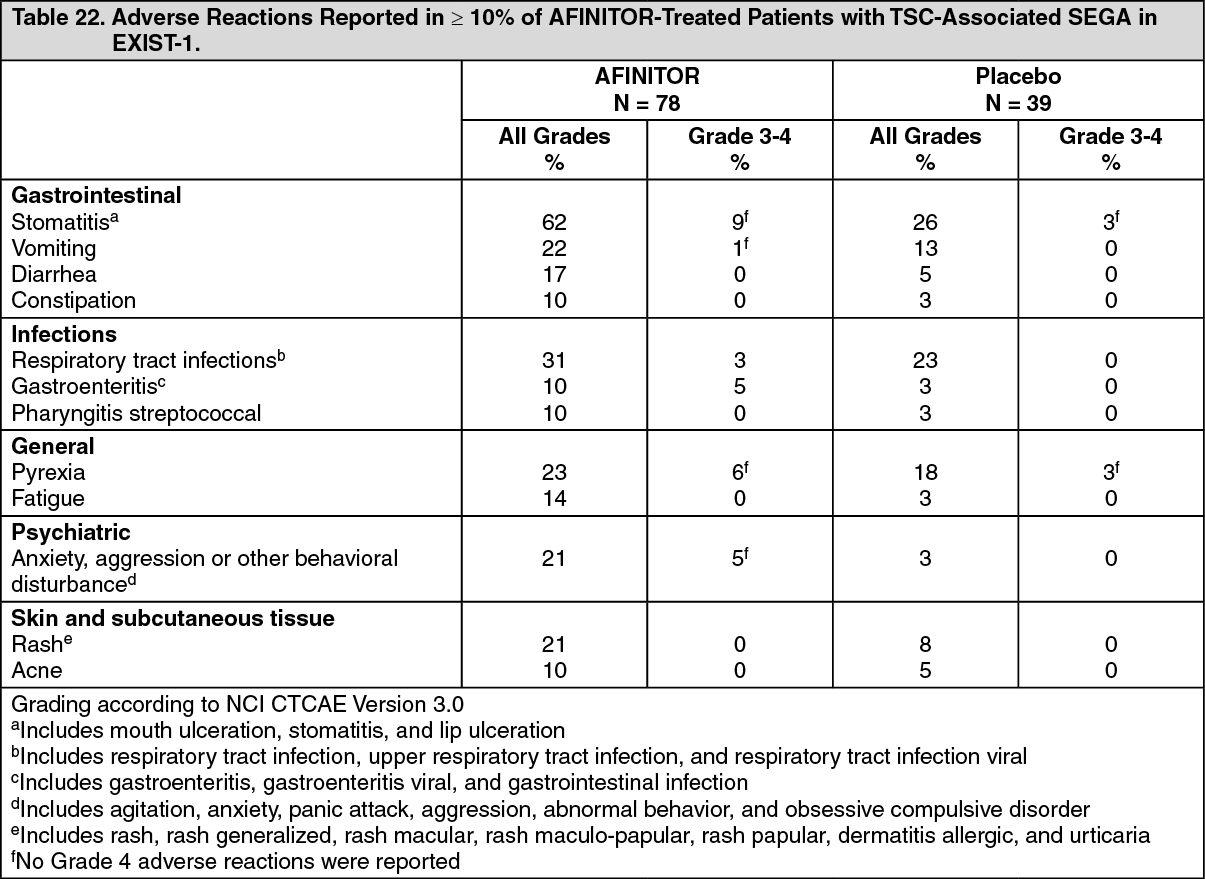
TSC-Associated Subependymal Giant Cell Astrocytoma (SEGA): The data described as follows are based on a randomized (2:1), double-blind, placebo-controlled trial (EXIST-1) of AFINITOR in 117 patients with SEGA and TSC. The median age of patients was 9.5 years (0.8 to 26 years), 93% were White, and 57% were male. The median duration of blinded study treatment was 52 weeks (24 to 89 weeks) for patients receiving AFINITOR.
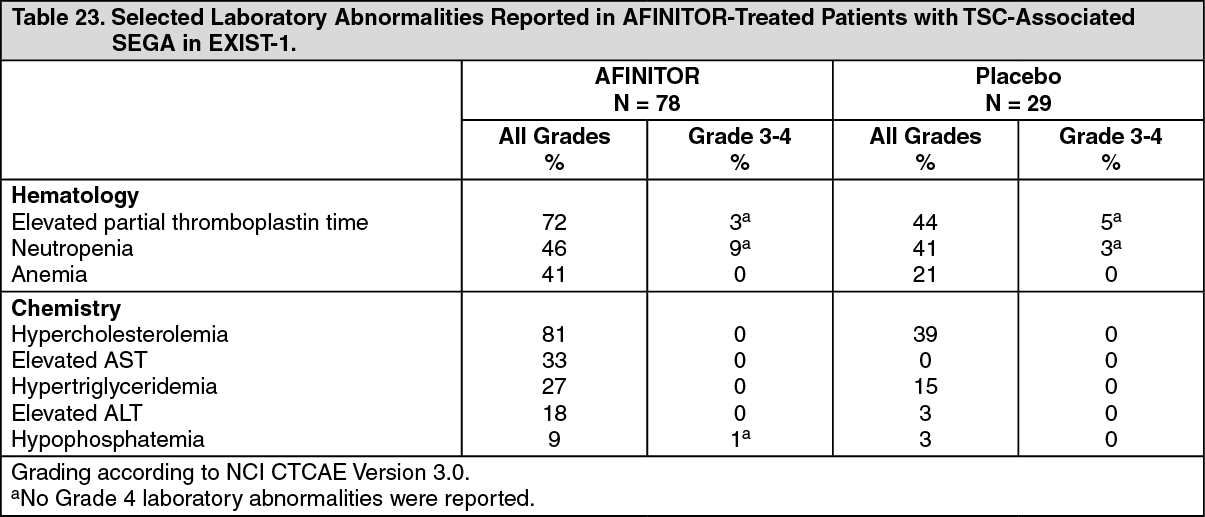
The most common adverse reactions reported for AFINITOR (incidence ≥ 30%) were stomatitis and respiratory tract infection. The most common Grade 3-4 adverse reactions (incidence ≥ 2%) were stomatitis, pyrexia, pneumonia, gastroenteritis, aggression, agitation, and amenorrhea. The most common laboratory abnormalities (incidence ≥ 50%) were hypercholesterolemia and elevated partial thromboplastin time. The most common Grade 3-4 laboratory abnormality (incidence ≥ 3%) was neutropenia.
There were no adverse reactions resulting in permanent discontinuation. Dose adjustments (interruptions or reductions) due to adverse reactions occurred in 55% of AFINITOR-treated patients. The most common adverse reaction leading to AFINITOR dose adjustment was stomatitis.
Adverse reactions reported with an incidence of ≥ 10% for patients receiving AFINITOR and occurring more frequently with AFINITOR than with placebo are reported in Table 22. Laboratory abnormalities are presented in Table 23. (See Table 22.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAmenorrhea occurred in 17% of AFINITOR-treated females aged 10 to 55 years (3 of 18). For this same group of AFINITOR-treated females, the following menstrual abnormalities were reported: dysmenorrhea (6%), menorrhagia (6%), metrorrhagia (6%), and unspecified menstrual irregularity (6%).
The following additional adverse reactions occurred in less than 10% of AFINITOR-treated patients: nausea (8%), pain in extremity (8%), insomnia (6%), pneumonia (6%), epistaxis (5%), hypersensitivity (3%), increased blood luteinizing hormone (LH) levels (1%), and pneumonitis (1%). (See Table 23.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageUpdated safety information from 111 patients treated with AFINITOR for a median duration of 47 months identified the following additional notable adverse reactions and selected laboratory abnormalities: decreased appetite (14%), hyperglycemia (13%), hypertension (11%), urinary tract infection (9%), decreased fibrinogen (8%), cellulitis (6%), abdominal pain (5%), decreased weight (5%), elevated creatinine (5%), and azoospermia (1%).
Postmarketing Experience: The following adverse reactions have been identified during post approval use of AFINITOR. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate frequency or establish a causal relationship to drug exposure: Blood and lymphatic disorders: Thrombotic microangiopathy.
Cardiac: Cardiac failure with some cases reported with pulmonary hypertension (including pulmonary arterial hypertension) as a secondary event.
Gastrointestinal: Acute pancreatitis.
Hepatobiliary: Cholecystitis and cholelithiasis.
Infections: Sepsis and septic shock.
Nervous system: Reflex sympathetic dystrophy.
Vascular: Arterial thrombotic events, lymphedema.
Injury, poisoning and procedural complications: Radiation sensitization and radiation recall.
View ADR Monitoring Form