The information highlighted (if any) are the most recent updates for this brand.
Live, attenuated varicella virus (Oka/Merck strain).
VARIVAX (Refrigerated) is a live, attenuated virus vaccine (a lyophilized preparation of the Oka/Merck strain of varicella).
Pharmacology: Varicella: Varicella is a highly communicable disease in children, adolescents, and adults caused by the varicella-zoster virus. The disease usually consists of 300 to 500 maculopapular and/or vesicular lesions accompanied by a fever (oral temperature-100°F) in up to 70% of individuals. Approximately 3.5 million cases of varicella occurred annually from 1980 to 1994 in the United States with the peak incidence occurring in children five to nine years of age. The incidence rate of chickenpox was 8.3 to 9.1% per year in children 1 to 9 years of age. The attack rate of wild-type varicella following household exposure among healthy susceptible children was shown to be 87%. Although it is generally a benign, self-limiting disease, varicella may be associated with serious complications (e.g., bacterial superinfection, pneumonia, encephalitis, Reye syndrome), and/or death.
Clinical Studies: Evaluation of Clinical Efficacy Afforded by VARIVAX (Refrigerated): Clinical Data in Children: In combined clinical trials of varicella virus vaccine live (Oka/Merck) [hereafter referred to as varicella vaccine (Oka/Merck)] at doses ranging from 1,000 to 17,000 PFU, the majority of subjects who received varicella vaccine (Oka/Merck) and were exposed to wild-type virus were either completely protected from chickenpox or developed a milder form (for clinical description see as follows) of the disease.
The protective efficacy of varicella vaccine (Oka/Merck) was evaluated in three different ways: by a placebo-controlled, double-blind clinical trial over 2 years (efficacy 95 to 100%); by comparing chickenpox rates over 7 to 9 years in vaccinees versus historical controls (efficacy 83 to 94%); and by assessment of protection from disease following household exposure over 7 to 9 years (efficacy 81 to 88%).
Although no placebo-controlled trial was carried out with VARIVAX (Refrigerated) using the current formulation of the vaccine, a placebo-controlled trial was conducted using a formulation containing 17,000 PFU per dose. In this trial, a single dose of varicella vaccine (Oka/Merck) protected 95 to 100% of children against chickenpox over a two-year period.
The study enrolled healthy individuals 1 to 14 years of age (n=491 vaccine, n=465 placebo). In the first year, 8.5% of placebo recipients contracted chickenpox, while no vaccine recipient did, for a calculated protection rate of 100% during the first varicella season. In the second year, when only a subset of individuals agreed to remain in the blinded study (n=169 vaccine, n=163 placebo), 95% protective efficacy was calculated for the vaccine group as compared with placebo.
In early clinical trials, a total of 4240 children 1 to 12 years of age received 1000 to 1625 PFU of attenuated virus per dose of varicella vaccine (Oka/Merck) and have been followed for up to 9 years post single-dose vaccination. In this group, there was considerable variation in chickenpox rates among studies and study sites, and much of the reported data was acquired by passive follow-up. It was observed that 0.3 to 3.8% of vaccines per year reported chickenpox (called breakthrough cases). This represents an approximate 83% (95% confidence interval [Cl], 82%, 84%) decrease from the age-adjusted expected incidence rates in susceptible subjects over this same period. In those who developed breakthrough chickenpox postvaccination, the majority experienced mild disease (median of the maximum number of lesions <50). In one study, a total of 47% (27/58) of breakthrough cases had <50 lesions compared with 8% (7/92) in unvaccinated individuals, and 7% (4/58) of breakthrough cases had ≥300 lesions compared with 50% (46/92) in unvaccinated individuals.
Among a subset of vaccinees who were actively followed in these early trials for up to 9 years postvaccination, 179 individuals had household exposure to chickenpox. There were no reports of breakthrough chickenpox in 84% (150/179) of exposed children, while 16% (29/179) reported a mild form of chickenpox (38% (11/29) of the cases with a maximum total number of <50 lesions; no individuals with ≥300 lesions). This represents an 81% reduction in the expected number of varicella cases utilizing the historical attack rate of 87% following household exposure to chickenpox in unvaccinated individuals in the calculation of efficacy.
In later clinical trials, a total of 1164 children 1 to 12 years of age received 2900 to 9000 PFU of attenuated virus per dose of varicella vaccine (Oka/Merck) and have been actively followed for up to 7 years post single-dose vaccination. It was observed that 0.2 to 2.3% of vaccinees per year reported breakthrough chickenpox for up to 7 years post single-dose vaccination. This represents an approximate 94% (95% Cl, 92%, 95%) decrease from the age-adjusted expected incidence rates in susceptible subjects over the same period. In those who developed breakthrough chickenpox postvaccination, the majority experienced mild disease with the median of the maximum total number of lesions <50. The severity of reported breakthrough chickenpox, as measured by number of lesions and maximum temperature, appeared not to increase with time since vaccination.
Among a subset of vaccinees who were actively followed in these later trials for up to 7 years postvaccination, 80 individuals were exposed to an unvaccinated individual with wild-type chickenpox in a household setting. There were no reports of breakthrough chickenpox in 90% (72/80) of exposed children, while 10% (8/80) reported varicella after household exposure. This represents an 88% reduction in the expected number of varicella cases utilizing the historical attack rate of 87% following household exposure to chickenpox in unvaccinated individuals in the calculation of efficacy. The reported cases of varicella were mild, with annual median number of lesions (maximum daily total) ranging from 10 to 34.
Among 9202 children ≤12 years of age who received 1 injection of varicella vaccine (Oka/Merck), there were 1149 cases of breakthrough varicella (occurring more than 6 weeks postvaccination) of which 20 (1.7%) were classified as severe (≥300 lesions and a temperature ≥37.8°C oral). Compared with the proportion of severe cases (36%) from wild-type varicella infection in unvaccinated historical controls, this represents a 95% relative reduction in the proportion of severe cases among recipients of varicella vaccine who developed breakthrough varicella.
There are an insufficient number of breakthrough chickenpox cases in vaccinated children to assess the rate of protection of varicella vaccine (Oka/Merck) against the serious complications of chickenpox (e.g., encephalitis, hepatitis, pneumonia).
Clinical Data in Adolescents and Adults: Although no placebo-controlled trial was carried out in adolescents and adults, the protective efficacy of varicella vaccine (Oka/Merck) was calculated by evaluation of protection when vaccinees received 2 doses of varicella vaccine (Oka/Merck) 4 or 8 weeks apart and were subsequently exposed to chickenpox in a household setting over 6 to 7 years. In earlier clinical trials with up to 6 years of follow-up, 13 of the 76 individuals (17%) who had household exposure to chickenpox, developed varicella. All of the varicella cases that were reported were generally mild with a median of 37 lesions (range 8 to 75). In later clinical trials with up to 7 years of follow-up, none of 19 individuals (0%) who had household exposure to chickenpox, developed varicella.
The attack rate of unvaccinated adults exposed to a single contact in a household has not been previously studied. If the attack rate of 87% following household exposure in susceptible children holds true for susceptible adolescents and adults, the estimated efficacy of the vaccine in the prevention of any varicella disease would range from 80 to 100%.
There are an insufficient number of breakthrough chickenpox cases among vaccinated adolescents and adults to assess the rate of protection of varicella vaccine (Oka/Merck) against the serious complications of chickenpox (e.g., encephalitis, hepatitis, pneumonia) and during pregnancy (congenital varicella syndrome).
Immunogenicity of Varicella Vaccine (Oka/Merck): Clinical trials with several formulations of the vaccine containing attenuated virus ranging from 1000 to 50,000 PFU per dose have demonstrated that varicella vaccine (Oka/Merck) induces detectable humeral immune responses in a high proportion of individuals and is generally well tolerated in healthy individuals ranging from 12 months to 55 years of age.
Seroconversion as defined by the acquisition of any detectable varicella antibodies based on assay cutoff that generally corresponds to 0.6 units in the gpELISA, a highly sensitive assay which is not commercially available), was observed in 98% of vaccinees at approximately 4 to 6 weeks postvaccination in 9610 susceptible children 12 months to 12 years of age who received doses ranging from 1000 to 50,000 PFU. Rates of breakthrough disease were significantly lower among children with varicella antibody titers ≥5 gpELISA units compared to children with titers <5 gpELISA units. Titers ≥5 gpELISA units were induced in approximately 83% of children vaccinated with a single dose of vaccine at 1000 to 50,000 PFU per dose. The immune response rate to varicella vaccine (Oka/Merck) (as determined by the percentage of subjects with varicella antibody titers ≥5 gpEUSA units at 6 weeks postvaccination, an approximate correlation of protection) in subjects participating in follow-up studies ranged from 72 to 98%.
In a multicenter study involving susceptible adolescents and adults 13 years of age and older, two doses of varicella vaccine (Oka/Merck) administered four to eight weeks apart induced a seroconversion rate (gpELISA ≥0.6 units) of approximately 75% in 539 individuals four weeks after the first dose and of 99% in 479 individuals four weeks after the second dose. The average antibody response in vaccinees who received the second dose eight weeks after the first dose was higher than that in those who received the second dose four weeks after the first dose. In another multicenter study involving adolescents and adults, two doses of varicella vaccine (Oka/Merck) administered eight weeks apart induced a seroconversion rate (gpELISA ≥0.6 units) of 94% in 142 individuals six weeks after the first dose and 99% in 122 individuals six weeks after the second dose.
Varicella vaccine (Oka/Merck) also induces cell-mediated immune responses in vaccinees. The relative contributions of humoral immunity and cell-mediated immunity to protection from chickenpox are unknown.
Persistence of Immune Response: In those clinical studies involving healthy children who have been followed long-term post single-dose vaccination, detectable varicella antibodies (gpELISA ≥0.6 units) were present in 99.1% (3092/3120) at 1 year, 99.4% (1382/1391) at 2 years, 98.7% (1032/1046) at 3 years, 99.3% (997/1004) at 4 years, 99.2% (727/733) at 5 years, and 100% (432/432) at 6 years postvaccination.
In clinical studies involving healthy adolescents and adults who received 2 doses of vaccine, detectable varicella antibodies (gpELISA ≥0.6 units) were present in 97.9% (568/580) at 1 year, 97.1% (34/35) at 2 years, 100% (144/144) at 3 years, 97.0% (98/101) at 4 years, 97.5% (78/80) at 5 years, and 100% (45/45) at 6 years postvaccination.
A boost in antibody levels has been observed in vaccinees following exposure to wild-type varicella which could account for the apparent long-term persistence of antibody levels after vaccination in these studies. The duration of protection from varicella obtained using varicella vaccine (Oka/Merck) in the absence of wild-type boosting is unknown. Varicella vaccine (Oka/Merck) also induces cell-mediated immune responses in vaccinees. The relative contributions of humoral immunity and cell-mediated immunity to protection from chickenpox are unknown.
Transmission: In the placebo-controlled trial, transmission of vaccine virus was assessed in household settings (during the 8-week postvaccination period) in 416 susceptible placebo recipients who were household contacts of 445 vaccine recipients. Of the 416 placebo recipients, three developed chickenpox and seroconverted, nine reported a varicella-like rash and did not seroconvert, and six had no rash but seroconverted. If vaccine virus transmission occurred, it did so at a very low rate and possibly without recognizable clinical disease in contacts. These cases may represent either wild-type varicella from community contacts or a low incidence of transmission of vaccine virus from vaccinated contacts (see Precautions: Transmission). Post-marketing experience suggests that transmission of vaccine virus may occur rarely between healthy vaccinees who develop a varicella-like rash and healthy susceptible contacts. Transmission of vaccine virus from vaccinees who do not develop a varicella-like rash has also been reported.
Herpes Zoster: Overall, 9543 healthy children (12 months to 12 years of age) and 1652 adolescents and adults (13 years of age and older) have been vaccinated with Oka/Merck live attenuated varicella vaccine in clinical trials. Twelve cases of herpes zoster have been reported in children during 84,414 person years of follow-up in clinical trials, resulting in a calculated incidence of at least 14 cases per 100,000 person years. The completeness of this reporting has not been determined. Two cases of herpes zoster have been reported in the adolescent and adult age group during 12,372 person years of follow-up in clinical trials resulting in a calculated incidence of 16 cases per 100,000 person years.
All 14 cases of herpes zoster were mild and no sequelae were reported. Two cultures (one child and one adult) obtained from vesicles were positive for wild-type varicella zoster virus as confirmed by restriction endonuclease analysis. The long-term effect of varicella vaccine (Oka/Merck) on the incidence of herpes zoster, particularly in those vaccinees exposed to wild-type varicella, is unknown at present.
In children, the reported rate of zoster in vaccine recipients appears not to exceed that previously determined in a population-based study of healthy children who had experienced wild-type varicella. The incidence of zoster in adults who have had wild-type varicella infection is higher than that in children.
Reye Syndrome: Reye syndrome has occurred in children and adolescents following wild-type varicella infection, the majority of whom had received salicylates. In clinical studies in healthy children and adolescents in the United States, physicians advised varicella vaccine recipients not to use salicylates for six weeks after vaccination. There were no reports of Reye syndrome in varicella vaccine recipients during these studies.
Studies with Other Vaccines: In combined clinical studies involving 1107 children 12 to 36 months of age, 680 received varicella vaccine (Oka/Merck) and M-M-R II* (Measles, Mumps, and Rubella Virus Vaccine Live) concomitantly at separate sites and 427 received the vaccines six weeks apart. Seroconversion rates and antibody levels were comparable between the two groups at approximately six weeks postvaccination to each of the virus vaccine components. No differences were noted in adverse reactions reported in those who received varicella vaccine (Oka/Merck) concomitantly with M-M-R II at separate sites and those who received varicella vaccine (Oka/Merck) and M-M-R II at different times (see Interactions).
In a clinical study involving 316 children 12 months to 42 months of age, 160 received an investigational vaccine (a formulation combining measles, mumps, rubella, and varicella in one syringe) concomitantly with booster doses of DTaP (diphtheria, tetanus, acellular pertussis) and OPV (oral poliovirus vaccine) while 156 received M-M-R II concomitantly with booster doses of DTaP and OPV followed by varicella vaccine (Oka/Merck) 6 weeks later. At six weeks postvaccination, seroconversion rates for measles, mumps, rubella, and varicella and the percentage of vaccinees whose titers were boosted for diphtheria, tetanus, pertussis, and polio were comparable between the two groups, but anti-varicella levels were decreased when the investigational vaccine containing varicella was administered concomitantly with DTaP. No clinically significant differences were noted in adverse reactions between the two groups.
In another clinical study involving 306 children 12 to 18 months of age, 151 received an investigational vaccine (a formulation combining measles, mumps, rubella, and varicella in one syringe) concomitantly with a booster dose of PedvaxHIB* [Haemophilus b Conjugate Vaccine (Meningococcal Protein Conjugate)] while 155 received M-M-R II concomitantly with a booster dose of PedvaxHIB followed by varicella vaccine (Oka/Merck) 6 weeks later. At six weeks postvaccination, seroconversion rates for measles, mumps, rubella, and varicella, and geometric mean titers for PedvaxHIB were comparable between the two groups, but anti-varicella levels were decreased when the investigational vaccine containing varicella was administered concomitantly with PedvaxHIB. No clinically significant differences in adverse reactions were seen between the two groups.
In a clinical study involving 609 children 12 months to 23 months of age, 305 received varicella vaccine (Oka/Merck), M-M-R II, and TETRAMUNE** (Haemophilus influenzae type b, diphtheria, tetanus, and pertussis vaccines) concomitantly at separate sites and 304 received M-M-R II and TETRAMUNE given concomitantly followed by varicella vaccine (Oka/Merck) 6 weeks later. At six weeks postvaccination, seroconversion rates for measles, mumps, rubella, and varicella were similar between the two groups. Compared to prevaccination GMTs, the six-week postvaccination boost in GMTs for Haemophilus influenzae type b, diphtheria, tetanus and pertussis was similar between the two groups. GMTs for all antigens were similar except for varicella which was lower when varicella vaccine (Oka/Merck) was administered concomitantly with M-M-R II and TETRAMUNE but within the range of GMTs seen in previous clinical experience when varicella vaccine (Oka/Merck) was administered alone. At 1 year postvaccination, GMTs for measles, mumps, rubella, varicella and Haemophilus influenzae type b were similar between the two groups. All three vaccines were well tolerated regardless of whether they were administered concomitantly at separate sites or 6 weeks apart. There were no clinically important differences in reaction rates when the three vaccines were administered concomitantly versus 6 weeks apart.
In a clinical study involving 822 children 12 to 15 months of age, 410 received COMVAX* [Haemophilus b Conjugate (Meningococcal Protein Conjugate) and Hepatitis B (Recombinant) vaccine], M-M-R II, and varicella vaccine (Oka/Merck) concomitantly at separate sites, and 412 received COMVAX followed by M-M-R II and varicella vaccine (Oka/Merck) given concomitantly at separate sites, 6 weeks later. At 6 weeks postvaccination, the immune responses for the subjects who received the concomitant injections of COMVAX, M-M-R II, and varicella vaccine (Oka/Merck) were similar to those of the subjects who received COMVAX followed 6 weeks later by M-M-R II and varicella vaccine (Oka/Merck) with respect to all antigens administered. All 3 vaccines were generally well tolerated regardless of whether they were administered concomitantly at separate sites or 6 weeks apart. There were no clinically important differences in reaction rates when the 3 vaccines were administered concomitantly versus 6 weeks apart.
VARIVAX (Refrigerated) is recommended for subcutaneous administration. However, during clinical trials, some children received varicella vaccine (Oka/Merck) intramuscularly resulting in seroconversion rates similar to those in children who received the vaccine by the subcutaneous route. Persistence of antibody and efficacy in those receiving intramuscular injections have not been defined.
Toxicology: Carcinogenesis, Mutagenesis, Reproduction: VARIVAX (Refrigerated) has not been evaluated for its carcinogenic or mutagenic potential, or its potential to impair fertility.
VARIVAX (Refrigerated) is indicated for vaccination against varicella in individuals 12 months of age and older.
FOR SUBCUTANEOUS ADMINISTRATION. Do not inject intravenously.
Children 12 months to 12 years of age should receive a single 0.5 mL dose administered subcutaneously.
Adolescents and adults 13 years of age and older should receive a 0.5 mL dose administered subcutaneously at elected date and a second 0.5 mL dose 4 to 8 weeks later.
The outer aspect of the upper arm (deltoid region) is the preferred site of injection.
Methods of administration: Prefilled syringe of diluent: To reconstitute the vaccine, inject all of the diluent (0.7 mL) in the prefilled syringe into the vial of lyophilized vaccine and gently agitate to mix thoroughly. Withdraw the entire contents into the syringe and inject the total volume (about 0.5 mL) of reconstituted vaccine subcutaneously, preferably into the outer aspect of the upper arm (deltoid region) or the anterolateral thigh. IT IS RECOMMENDED THAT THE VACCINE BE ADMINISTERED IMMEDIATELY AFTER RECONSTITUTION, TO MINIMIZE LOSS OF POTENCY. DISCARD IF RECONSTITUTED VACCINE IS NOT USED WITHIN 30 MINUTES.
Do not freeze reconstituted vaccine.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. VARIVAX (Refrigerated) when reconstituted is a clear, colorless to pale yellow liquid.
CAUTION: A sterile syringe free of preservatives, antiseptics, and detergents should be used for each injection and/or reconstitution of VARIVAX (Refrigerated) because these substances may inactivate the vaccine virus.
It is important to use a separate sterile syringe and needle for each patient to prevent transmission of infectious agents from one individual to another.
To reconstitute the vaccine, use only the diluent supplied (Sterile Diluent for Merck, Sharp, & Dohme Live Virus Vaccines), since it is free of preservatives or other anti-viral substances which might inactivate the vaccine virus.
Accidental administration of more than the recommended dose of varicella vaccine (live) (Oka/Merck strain) has been reported (either a larger dose than recommended was injected, more than one injection was given, or the interval between injections was shorter than that recommended). Of these cases, the following adverse events were reported: injection-site redness, soreness, inflammation; irritability; gastrointestinal complaints (i.e., hematemesis, fecal emesis, gastroenteritis with vomiting and diarrhea); cough and viral infection. None of the cases had long-term sequelae.
History of hypersensitivity to any component of the vaccine, including gelatin.
History of anaphylactoid reaction to neomycin (each dose of reconstituted vaccine contains trace quantities of neomycin).
Blood dyscrasias, leukemia, lymphomas of any type, or other malignant neoplasms affecting the bone marrow or lymphatic systems.
Immunosuppressive therapy (including high-dose corticosteroids); however, VARIVAX (Refrigerated) is not contraindicated for use with topical corticosteroids or low-dose corticosteroids, as are commonly used for asthma prophylaxis. Individuals who are on immunosuppressant drugs are more susceptible to infections than healthy individuals. Vaccination with live attenuated varicella vaccine can result in a more extensive vaccine-associated rash or disseminated disease in individuals on immunosuppressant doses of corticosteroids.
Primary and acquired immunodeficiency states, including immunosuppression in association with AIDS or other clinical manifestations of infection with human immunodeficiency virus, except immunosuppression in asymptomatic children with CD4 T-lymphocyte percentages ≥25%.
Family history of congenital or hereditary immunodeficiency, unless the immune competence of the potential vaccine recipient is demonstrated.
Active untreated tuberculosis.
Any active febrile illness with fever >38.5°C (>101.3°F); however, low-grade fever itself is not a contraindication to vaccination.
Pregnancy: the possible effects of the vaccine on fetal development are unknown at this time. However, wild-type varicella is known to sometimes cause fetal harm. If vaccination of postpubertal females is undertaken, pregnancy should be avoided for three months following vaccination (see Use in Pregnancy & Lactation).
Adequate treatment provisions, including epinephrine injection (1:1000), should be available for immediate use should an anaphylactoid reaction occur.
The duration of protection from varicella infection after vaccination with VARIVAX (Refrigerated) is unknown.
The safety and efficacy of VARIVAX (Refrigerated) have not been established in children and young adults who are known to be infected with human immunodeficiency virus with and without evidence of immunosuppression (see also Contraindications).
Transmission: Post-marketing experience suggests that transmission of vaccine virus may occur rarely between healthy vaccinees who develop a varicella-like rash and healthy susceptible contacts. Transmission of vaccine virus from vaccinees who do not develop a varicella-like rash has also been reported.
Therefore, vaccine recipients should attempt to avoid, whenever possible, close association with susceptible high-risk individuals for up to six weeks. In circumstances where contact with high-risk individuals is unavoidable, the potential risk of transmission of vaccine virus should be weighed against the risk of acquiring and transmitting wild-type varicella virus. Susceptible high-risk individuals include: immunocompromised individuals; pregnant women without documented history of chickenpox or laboratory evidence of prior infection; newborn infants of mothers without documented history of chickenpox or laboratory evidence of prior infection.
Pediatric Use: No clinical data are available on safety or efficacy of VARIVAX (Refrigerated) in children less than one year of age. Administration to infants under twelve months of age is not recommended.
Effects on Ability to Drive and Use Machines:There are no data to suggest that VARIVAX (Refrigerated) affects the ability to drive or operate machinery.
Pregnancy: There are no adequate and well-controlled studies in pregnant women. It is not known whether VARIVAX (Refrigerated) can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. Therefore, VARIVAX (Refrigerated) should not be administered to pregnant females; furthermore, pregnancy should be avoided for three months following vaccination (see Contraindications).
Nursing Mothers: It is not known whether varicella vaccine virus is secreted in human milk. Therefore, because some viruses are secreted in human milk, caution should be exercised if VARIVAX (Refrigerated) is administered to a nursing woman.
Clinical Studies: In clinical trials, varicella virus vaccine live (Oka/Merck) [hereafter called, varicella vaccine (Oka/Merck)] was administered to approximately 17,000 healthy children, adolescents, and adults. Varicella vaccine (Oka/Merck) was generally well tolerated.
In a double-blind placebo-controlled study among 956 healthy children and adolescents, 914 of whom were serologically confirmed to be susceptible to varicella, the only adverse reactions that occurred at a significantly greater rate in vaccine recipients than in placebo recipients were pain and redness at the injection site and varicella-like rash.
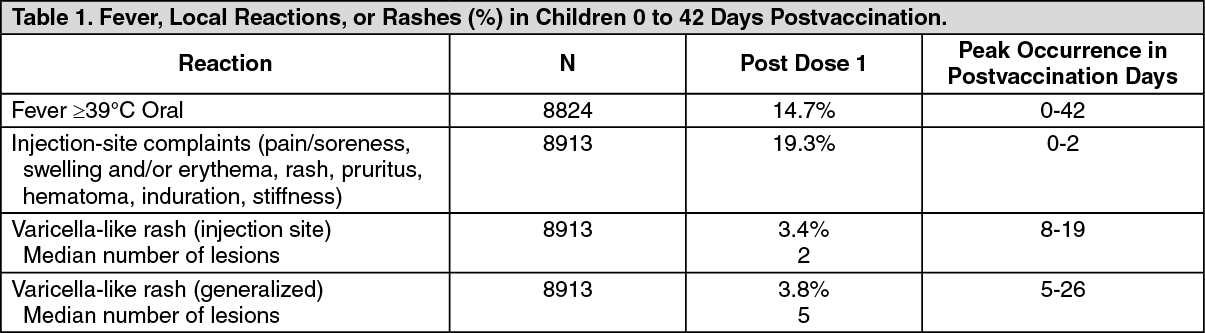
Children 1 to 12 Years of Age: In clinical trials involving approximately 8900 healthy children monitored for up to 42 days after a single dose of varicella vaccine (Oka/Merck), fever, injection-site complaints, or rashes were reported in decreasing order of frequency as follows: injection-site complaints (pain/soreness, swelling and/or erythema, rash, pruritus, hematoma, induration, stiffness); fever-102°F (38.9°C) oral; varicella-like rash (generalized, median 5 lesions); varicella-like rash (injection site, median 2 lesions).
Adolescents and Adults 13 Years of Age and Older: In clinical trials involving approximately 1600 healthy adolescents and adults, the majority of whom received two doses of varicella vaccine (Oka/Merck) and were monitored for up to 42 days after any dose, fever, injection-site complaints, or rashes were reported in decreasing order of frequency as follows: injection-site complaints (soreness, erythema, swelling, rash, pruritus, pyrexia, hematoma, induration, numbness); fever-100°F (37.8°C) oral; varicella-like rash (generalized, median 5 lesions); varicella-like rash (injection site, median 2 lesions).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The following additional side effects have been reported regardless of causality since the vaccine has been marketed:
Body As A Whole: Anaphylaxis (including anaphylactic shock) and related phenomena such as angioneurotic edema, facial edema, and peripheral edema; anaphylaxis in individuals with or without an allergic history.
Eye Disorders: Necrotizing retinitis (reported only in immunocompromised individuals).
Gastrointestinal Disorders: Nausea; vomiting.
Hemic and Lymphatic System: Aplastic anemia; thrombocytopenia (including idiopathic thrombocytopenic purpura (ITP)), lymphadenopathy.
Infections and Infestations: Varicella (vaccine strain).
Nervous/Psychiatric: Encephalitis; cerebrovascular accident; transverse myelitis; Guillain- Barre syndrome; Bell's palsy; ataxia; febrile and non-febrile seizures; aseptic meningitis, dizziness; paresthesia; irritability.
Respiratory: Pharyngitis; pneumonia/pneumonitis, upper respiratory tract infection.
Skin: Stevens-Johnson syndrome; erythema multiforme; Henoch-Schonlein purpura; secondary bacterial infections of skin and soft tissue, including impetigo and cellulitis; herpes zoster.
Vaccination should be deferred for at least 5 months following blood or plasma transfusions, or administration of immune globulin or varicella zoster immune globulin (VZIG).
Following administration of VARIVAX (Refrigerated), any immune globulin including VZIG should not be given for 2 months thereafter unless its use outweighs the benefits of vaccination.
Vaccine recipients should avoid use of salicylates for 6 weeks after vaccination with VARIVAX (Refrigerated) as Reye syndrome has been reported following the use of salicylates during wild-type varicella infection.
Results from clinical studies indicate that VARIVAX (Refrigerated) can be administered concomitantly with M-M-R* II (Measles, Mumps, and Rubella Virus Vaccine Live), TETRAMUNE** (diphtheria and tetanus toxoids and pertussis vaccine adsorbed and Haemophilus b conjugate vaccine), or COMVAX* (Haemophilus influenzae type b conjugate and hepatitis B vaccine). If VARIVAX (Refrigerated) is not given concomitantly with M-M-R II, a 1-month interval between the 2 live virus vaccines should be observed.
Limited data from an experimental product containing varicella vaccine suggest that VARIVAX (Refrigerated) can be administered concomitantly with DTaP (diphtheria, tetanus, acellular pertussis) and PedvaxHIB* [Haemophilus b Conjugate Vaccine (Meningococcal Protein Conjugate)] using separate sites and syringes and with OPV (oral poliovirus vaccine).
Tuberculin skin testing, with tuberculin purified protein derivative (PPD), may be performed before VARIVAX is administered or on the same day, or at least 4 weeks following vaccination with VARIVAX, as other live virus vaccines may cause a temporary depression of tuberculin skin test sensitivity leading to false negative results.
Stability: VARIVAX (Refrigerated) has a minimum potency level of approximately 1350 PFU 30 minutes after reconstitution at room temperature (20 to 25°C, 68 to 77°F).
Storage: Vaccine Vial: During shipment, to ensure that there is no loss of potency, the vaccine must be maintained at a temperature of 2 to 8°C or colder (36 to 46°F or colder).
Before reconstitution, VARIVAX (Refrigerated) has a shelf-life of 24 months when refrigerated at 2 to 8°C or colder (36 to 46°F or colder). The vaccine may also be stored in a freezer; if subsequently transferred to a refrigerator, THE VACCINE SHOULD NOT BE REFROZEN.
Before reconstitution, protect from light.
DISCARD IF RECONSTITUTED VACCINE IS NOT USED WITHIN 30 MINUTES.
Combination pack with vaccine vial and diluent: For combination packs with vaccine vial and diluent packaged together, store in the refrigerator at 2 to 8°C (36 to 46°F). DO NOT STORE THE COMBINATION PACK IN THE FREEZER.
J07BK01 - varicella, live attenuated ; Belongs to the class of varicella viral vaccines.
Varivax vaccine (inj)
((vial) 0.5 mL single-dose + 0.7 mL diluent) 1's





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image7db929c6-226d-45de-8db8-aa81006ff290.GIF)

 Sign Out
Sign Out
