Each mL contains: Acetylcysteine 200 mg.
Pharmacology: After oral administration of 100 mg/kg, N-Acetylcysteine (NAC) is completely absorbed and undergoes rapid and extensive metabolism in the intestinal wall and liver. The elimination half-life was 5-6 hours after intravenous administration. NAC is mainly excreted in the urine. The main urinary metabolite of NAC is the inorganic sulphate. However, during the acute paracetamol intoxication, the urinary metabolite of NAC may differ, being at least partially represented by complexation products of NAC or its derivatives with the toxic. In toxic pathology, NAC exerts its effects on multiple mechanisms. The best known effect regards its action as precursor of glutathione. NAC acts as precursor of cysteine needed for GSH synthesis (by deacetylation with formulation of free cysteine and by reduction of plasma cystine to cysteine with formation of oxidized NAC); increase the total amount of glutathione (GSH+GSSG), if depleted; and facilitates conversion of glutathione from the oxidized form (GSSG) to the biologically active, reduced form (GSH).
Furthermore, in paracetamol poisoning, NAC acts by reducing the reactive metabolites (e.g. NAPQI) to atoxic compounds; conjugating itself directly with said metabolites; in a specific manner as antioxidant agent; and as precursor of sulfates necessary for the metabolization of paracetamol by sulfation.
These mechanisms justify the need of early treatment (within 10 hours) in paracetamol poisoning, to prevent or minimize with maximum efficacy the occurrence of hepatic damage. Likewise important is the capacity of NAC to improve peripheral utilization of O2, increasing delivery and peripheral extraction. In intoxications with severe hepatic insufficiency this makes its possible to prevent or correct tissutal hypoxia which represents one of the main factors responsible for the genesis of multiple organ insufficiency: this effect is evident even in the event of delayed treatment.
Voluntary or accidental paracetamol poisoning.
Acetylcysteine must be administered as
loading dose, early after paracetamol intake. Treatment must be continued for at least 72 hours.
In order to avoid the hypersensitive reaction described in the "adverse events", it is advisable to use slow infusion rate. For this purpose the drug is previously diluted with 5% Glucose or with physiological solution.
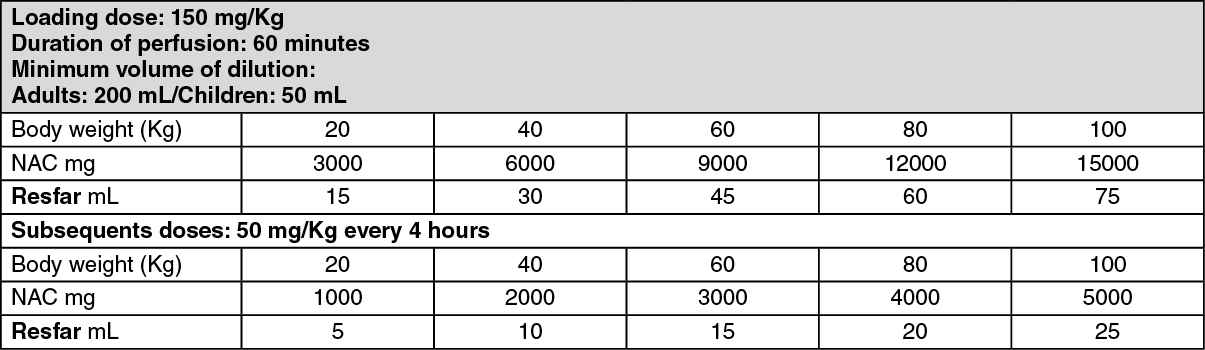
Loading dose: Bolus dose-NAC 150 mg/Kg in 60 minutes (at least 200 mL in the adult and 50 mL in the child in 5% glucose or physiological solution).
Subsequence doses: Treatment must be continued with 50 mg/Kg doses, at slow infusion rate, every 4 hours for a total of 72 hours of treatment.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Cases of overdose were characterized by similar symptomatology than those observed in the case of side effects. In case of overdose, treatment must be suspended. Overdose treatment is based on symptomatic treatment and/or resuscitation.
Known hypersensitivity to the drug or to other chemically correlated substances.
The possible presence of sulphurous odour dose not indicate an alternation of the products but is characteristic of the active ingredient contained in this preparation. The administration of NAC at high doses may reduce the prothrombin time. However, it is not established whether this is due to biological action of NAC or the result of an analytical interference. In any way the monitoring of coagulation factors is advisable particularly in case of liver transplantation. NAC may interfere with the determination of salycilates (colorimetric method) and with the determination of plasma and urinary ketones (nitroprusside test). Evaluation of experimental animal studies does not indicate teratogenic effects. The decision to use NAC at antidotal doses during pregnancy and lactation should be based on assessment of the risk-to-benefit ratio taking into consideration the particular characteristic of each case and in particular the risk for the mother and fetus induced by toxicant in the absence of specific treatment. In any case lactation must be suspended in case of poisoning.
Keep out the reach of children.
Anaphylactic reactions may occur when I.V. Acetylcysteine is directly administered at high doses as well as when too fast rate is used. Treatments of those reactions must be symptomatic. Therefore, the product must be administered according to the 'Dosage & Administration' described hereby. Patients suffering from bronchial asthma or with a history of asthma, must be closely controlled since bronchospasm may occur during treatment. In such event the treatment must be immediately suspended. Intravenous administration must be done in a hospital under strict medical surveillance.
The decision to use NAC at antidotal doses during pregnancy and lactation should be based on assessment of the risk-to-benefit ratio taking into consideration the particular characteristic of each case and in particular the risk for the mother and fetus induced by toxicant in the absence of specific treatment. In any case lactation must be suspended in case of poisoning.
After I.V. administration of acetylcysteine the following anaphylactic reactions have been seldomly reported: urticaria, angiodema, bronchospasm, nausea, vomiting, hypertension, tachycardia, dizziness and fever.
Probably, these are pseduo-allergic reactions due to the histamine release. These symptoms may require an urgent therapy.
Interaction between acetylcysteine and antibiotics were reported. However, these are not remarkable when NAC is administered as treatment for paracetamol poisoning.
V03AB23 - acetylcysteine ; Belongs to the class of antidotes. Used to neutralize paracetamol overdose.
Resfar infusion 200 mg/mL
25 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
