


 Sign Out
Sign Out

The prescribed dose should be administered orally with a meal and a large glass of water to minimize the risk of gastrointestinal disturbances. Doses of 400 mg or 600 mg should be administered once daily, whereas a daily dose of 800 mg should be administered as 400 mg twice a day, in the morning and in the evening.
For patients unable to swallow the film-coated tablets, the tablets may be dispersed in a glass of water or apple juice. The required number of tablets should be placed in the appropriate volume of beverage (approximately 50 mL for a 100 mg tablet, and 200 mL for a 400 mg tablet) and stirred with a spoon. The suspension should be administered immediately after complete disintegration of the tablet(s).
Treatment should be continued as long as the patient continues to benefit.
Monitoring of response to IMATERO therapy in Ph+ CML patients should be performed routinely and when therapy is modified, to identity suboptimal response, loss of response to therapy, poor patient compliance, or possible drug-drug interaction. Results of monitoring should guide appropriate CML management.
General target population: Dosage in CML: The recommended dosage of IMATERO is 400 mg/day for adult patients in chronic phase CML and 600 mg/day for patients in accelerated phase or blast crisis.
Dose increases from 400 mg to 600 mg or 800 mg in patients with chronic phase disease, or form 600 mg to a maximum of 800 mg daily in patients in accelerated phase or blast crisis may be considered in the absence of severe adverse drug reaction and severe non-leukaemia-related neutropenia or thrombocytopenia in the following circumstances: Disease progression (at any time); failure to achieve a satisfactory haematological response after at least 3 months of treatment; failure to achieve a cytogenetic response after 12 months of treatment; or loss of a previously achieved haematological and/or cytogenetic response.
Patients should be monitored closely following dose escalation given the potential for an increased incidence of adverse reactions at higher dosages.
Dosage in Ph+ ALL: The recommended dose of IMATERO is 600 mg/day for adult patients with Ph+ ALL.
Dosage in MDS/MPD: The recommended dose of IMATERO is 400 mg/day for adult patients with MDS/MPD.
Dosage in SM: The recommended dose of IMATERO is 400 mg/day for adult patients with SM without the D816V c-Kit mutation or mutational status unknown or not responding satisfactorily to other therapies.
For patients with SM associated with eosinophilia, a clonal haematological disease related to the fusion kinase FIP1L1-PDGFR-alpha, a starting dose of 100 mg/day is recommended. A dose increase from 100 mg to 400 mg for these patients may be considered in the absence of adverse drug reactions if assessments demonstrate an insufficient response to therapy.
Dosage in HES/CEL: The recommended dose of IMATERO is 400 mg/day for patients with HES/CEL.
For HES/CEL patients with demonstrated FIP1L1-PDGFR-alpha fusion kinase, a starting dose of 100 mg/day is recommended. A dose increase from 100 mg to 400 mg for these patients may be considered in the absence of adverse drug reactions if assessments demonstrate an insufficient response to therapy.
Dosage in DFSP: The recommended dose of IMATERO is 800 mg/day for adult patients with DFSP.
Dose adjustments for adverse drug reactions: Non haematological adverse reactions: If a severe non-haematological adverse reaction develops with IMATERO use, treatment must be withheld until the event has resolved. Thereafter, treatment can be resumed as appropriate depending on the initial severity of the event.
If elevations in bilirubin > 3 x institutional upper limit of normal (IULN) or in liver transaminases > 5 x IULN occur, IMATERO should withheld until bilirubin levels have returned to a < 1.5 x IULN and transaminase levels to < 2.5 x IULN. Treatment with IMATERO may then be continued at a reduced daily dose. In adults the dose should be reduced from 400 mg to 300 mg or from 600 mg to 400 mg, or from 800 mg to 600 mg.
Haematological adverse reactions: Dose reduction or treatment interruption for severe neutropenia and thrombocytopenia are recommended as indicated in the table as follows. (See table.)
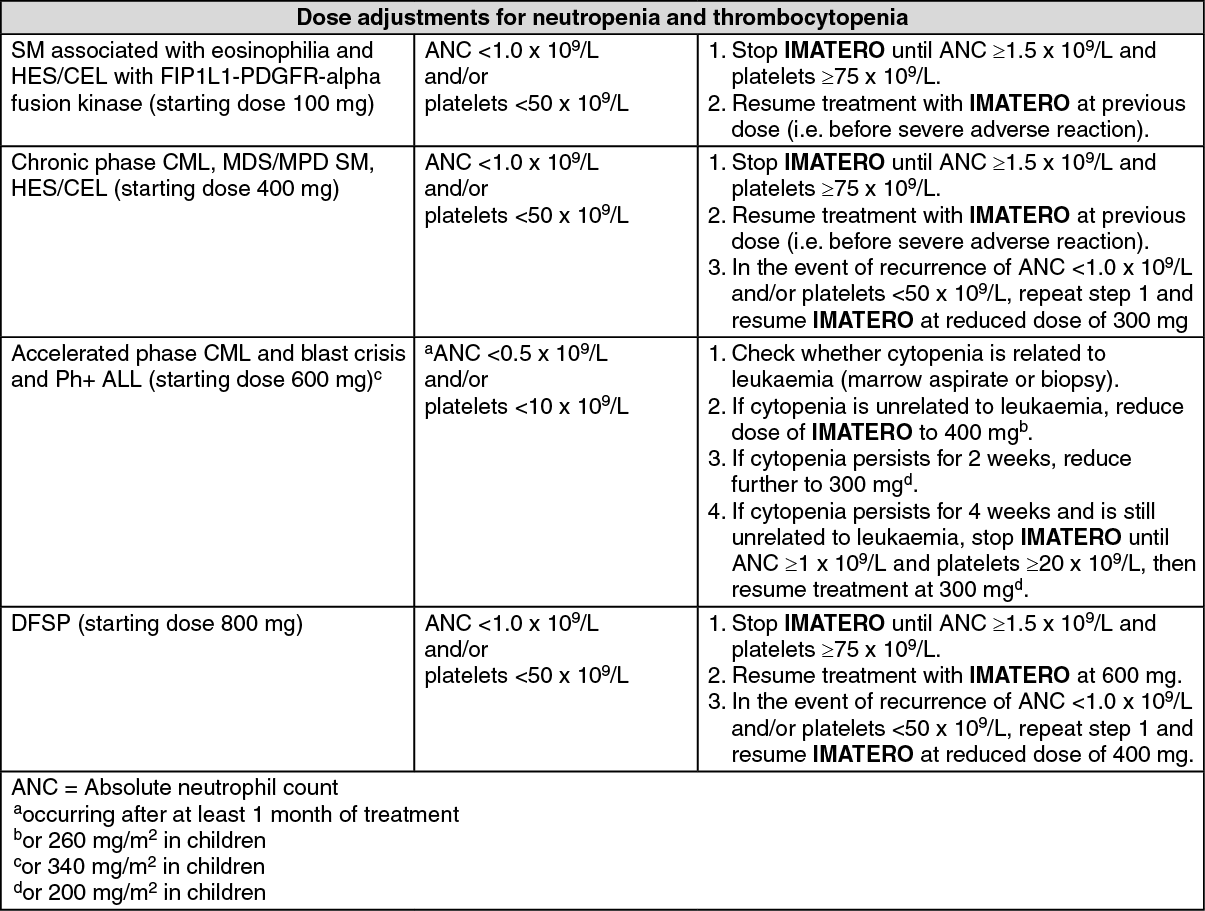 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSpecial populations: Children: There is no experience with the use of IMATERO in children with Ph+ ALL below 1 year of age. There is very limited to no experience with the use of IMATERO in children in other indications.
Dosing in children should be on the basis of body surface area (mg/m2). The dose of 340 mg/m2 daily is recommended for children with chronic phase and advanced phase Ph+ ALL (not to exceed the total dose of 600 mg daily). Treatment can be given as a once daily dose in Ph+ ALL.
Hepatic insufficiency: Imatinib is mainly metabolised through the liver. Patients with mild, moderate or severe liver dysfunction should be given the minimum recommended dose of 400 mg daily. The dose can be reduced if not tolerated (see PRECAUTIONS).
Renal insufficiency: Imatinib and its metabolites are not significantly excreted via the kidney. Since the renal clearance of Imatinib is negligible, a decrease in free drug clearance is not expected in patients with renal insufficiency. Patients with mild or moderate renal dysfunction should be given the minimum recommended dose of 400 mg daily as starting dose. Patients with severe renal dysfunction or on dialysis could also start at the same dose of 400 mg. However, in these patients caution is recommended. The dose can be reduced if not tolerated, or increased for lack of efficacy (see PRECAUTIONS).
Elderly patients: No specific dose recommendation is necessary in older people.