


 Sign Out
Sign Out

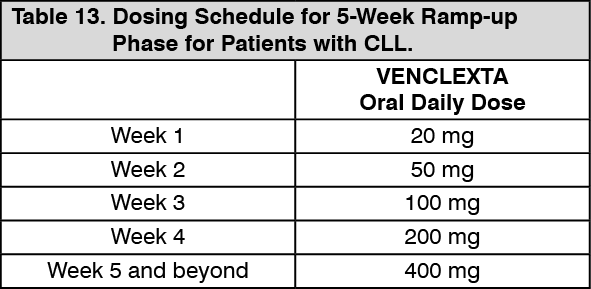
Recommended Dosage for Chronic Lymphocytic Leukemia: VENCLEXTA dosing begins with a 5-week ramp-up. The 5-week ramp-up dosing schedule is designed to gradually reduce tumor burden (debulk) and decrease the risk of TLS.
VENCLEXTA 5-week Dose Ramp-Up Schedule: Administer VENCLEXTA according to the 5-week ramp-up dosing schedule to the recommended dosage of 400 mg orally once daily as shown in Table 13. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe blister pack provides the first 4 weeks of VENCLEXTA according to the ramp-up schedule. The 400 mg dose is achieved using 100 mg tablets supplied in bottles [see Presentation].
In Combination with Obinutuzumab: Start obinutuzumab administration at 100 mg on Cycle 1 Day 1, followed by 900 mg on Cycle 1 Day 2. Administer 1000 mg on Days 8 and 15 of Cycle 1 and on Day 1 of each subsequent 28-day cycle for a total of 6 cycles. Refer to the obinutuzumab prescribing information for additional dosing information.
On Cycle 1 Day 22, start VENCLEXTA according to the 5-week ramp-up dosing schedule (see Table 13). After completing the ramp-up phase on Cycle 2 Day 28, continue VENCLEXTA at a dose of 400 mg orally once daily from Cycle 3 Day 1 until the last day of Cycle 12.
In Combination with Rituximab: Start rituximab administration after the patient has completed the 5-week ramp-up dosing schedule for VENCLEXTA (see Table 13) and has received VENCLEXTA at the recommended dosage of 400 mg orally once daily for 7 days. Administer rituximab on Day 1 of each 28-day cycle for 6 cycles, at a dose of 375 mg/m2 intravenously for Cycle 1 and 500 mg/m2 intravenously for Cycles 2-6. Continue VENCLEXTA 400 mg orally once daily for 24 months from Cycle 1 Day 1 of rituximab.
Refer to the rituximab prescribing information for additional dosing information.
Monotherapy: The recommended dosage of VENCLEXTA is 400 mg once daily after completion of the 5-week ramp-up dosing schedule (see Table 13). Continue VENCLEXTA until disease progression or unacceptable toxicity.
Recommended Dosage for Acute Myeloid Leukemia: The recommended dosage and ramp-up of VENCLEXTA depends upon the combination agent. Follow the dosing schedule, including the 3-day or 4-day dose ramp-up, as shown in Table 14. Start VENCLEXTA administration on Cycle 1 Day 1 in combination with: Azacitidine 75 mg/m2 intravenously or subcutaneously once daily on Days 1-7 of each 28-day cycle; OR Decitabine 20 mg/m2 intravenously once daily on Days 1-5 of each 28-day cycle; OR Cytarabine 20 mg/m2 subcutaneously once daily on Days 1-10 of each 28-day cycle. (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageContinue VENCLEXTA, in combination with azacitidine or decitabine or low-dose cytarabine, until disease progression or unacceptable toxicity.
Refer to Pharmacology: Pharmacodynamics: Clinical Studies: Acute Myeloid Leukemia under Actions and Prescribing Information for azacitidine, decitabine, or cytarabine for additional dosing information.
Risk Assessment and Prophylaxis for Tumor Lysis Syndrome: Patients treated with VENCLEXTA may develop tumor lysis syndrome (TLS). Refer to the appropriate section as follows for specific details on management. Assess patient-specific factors for level of risk of TLS and provide prophylactic hydration and anti-hyperuricemics to patients prior to first dose of VENCLEXTA to reduce risk of TLS.
Chronic Lymphocytic Leukemia: VENCLEXTA can cause rapid reduction in tumor and thus poses a risk for TLS in the initial 5-week ramp-up phase. Changes in blood chemistries consistent with TLS that require prompt management can occur as early as 6 to 8 hours following the first dose of VENCLEXTA and at each dose increase. TLS can also occur upon resumption of VENCLEXTA following a dosage interruption. See Table 16 and Table 17 for dose modifications of VENCLEXTA after interruption.
The risk of TLS is a continuum based on multiple factors, particularly reduced renal function (creatinine clearance [CLcr] <80 mL/min) and tumor burden; splenomegaly may also increase the risk of TLS.
Perform tumor burden assessments, including radiographic evaluation (e.g., CT scan), assess blood chemistry (potassium, uric acid, phosphorus, calcium, and creatinine) in all patients and correct pre-existing abnormalities prior to initiation of treatment with VENCLEXTA. The risk may decrease as tumor burden decreases [see Tumor Lysis Syndrome and Renal Impairment under Precautions].
Table 15 as follows describes the recommended TLS prophylaxis and monitoring during VENCLEXTA treatment based on tumor burden determination from clinical trial data. Consider all patient comorbidities before final determination of prophylaxis and monitoring schedule. Reassess the risk of TLS when reinitiating VENCLEXTA after a dosage interruption lasting more than 1 week during the ramp-up phase, or more than 2 weeks after completion of ramp-up. Institute prophylaxis and monitoring as needed. (See Table 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAcute Myeloid Leukemia: All patients should have white blood cell count less than 25 × 109/L prior to initiation of VENCLEXTA. Cytoreduction prior to treatment may be required.
Prior to first VENCLEXTA dose, provide all patients with prophylactic measures including adequate hydration and anti-hyperuricemic agents and continue during ramp-up phase.
Assess blood chemistry (potassium, uric acid, phosphorus, calcium, and creatinine) and correct pre-existing abnormalities prior to initiation of treatment with VENCLEXTA.
Monitor blood chemistries for TLS at pre-dose, 6 to 8 hours after each new dose during ramp-up, and 24 hours after reaching final dose.
For patients with risk factors for TLS (e.g., circulating blasts, high burden of leukemia involvement in bone marrow, elevated pretreatment lactate dehydrogenase [LDH] levels, or reduced renal function), consider additional measures, including increased laboratory monitoring and reducing VENCLEXTA starting dose.
Dosage Modifications for Adverse Reactions: Chronic Lymphocytic Leukemia: The recommended dosage modifications for VENCLEXTA for adverse reactions are provided in Table 16 and the recommended dose reductions for VENCLEXTA for adverse reactions are provided in Table 17.
For patients having a dosage interruption lasting more than 1 week during the ramp-up phase, or more than 2 weeks after completion of ramp-up, reassess for risk of TLS to determine if reinitiation with a reduced dose is necessary (e.g., all or some levels of the dose ramp-up schedule) [see Recommended Dosage for Chronic Lymphocytic Leukemia and Risk Assessment and Prophylaxis for Tumor Lysis Syndrome as previously mentioned]. (See Tables 16 and 17.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image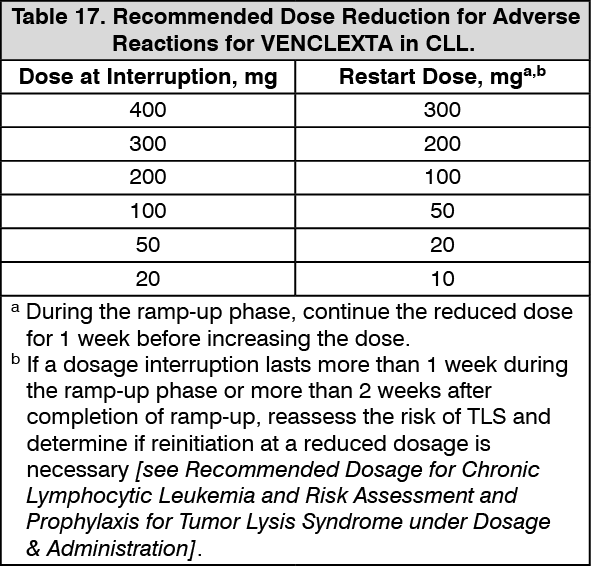 Click on icon to see table/diagram/image
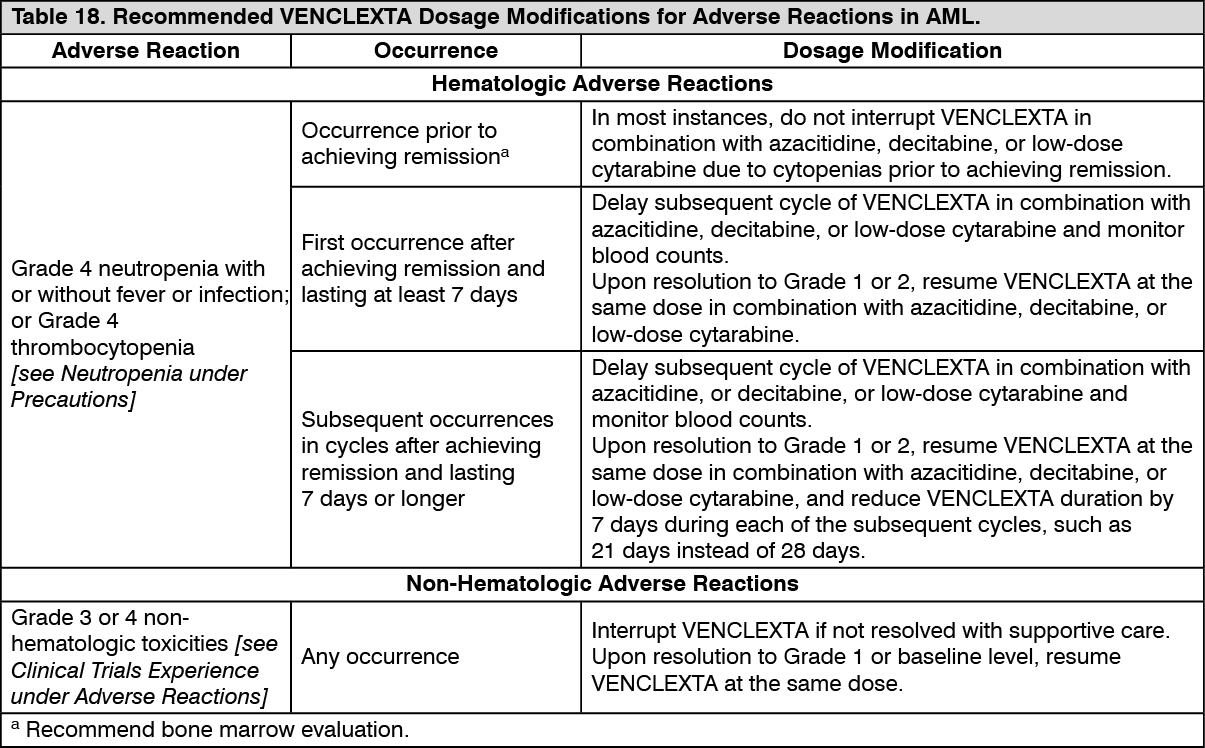
Click on icon to see table/diagram/imageAcute Myeloid Leukemia: Monitor blood counts frequently through resolution of cytopenias. Dose modification and interruptions for cytopenias are dependent on remission status. Dose modifications of VENCLEXTA for adverse reactions are provided in Table 18. (See Table 18.)
 Click on icon to see table/diagram/image
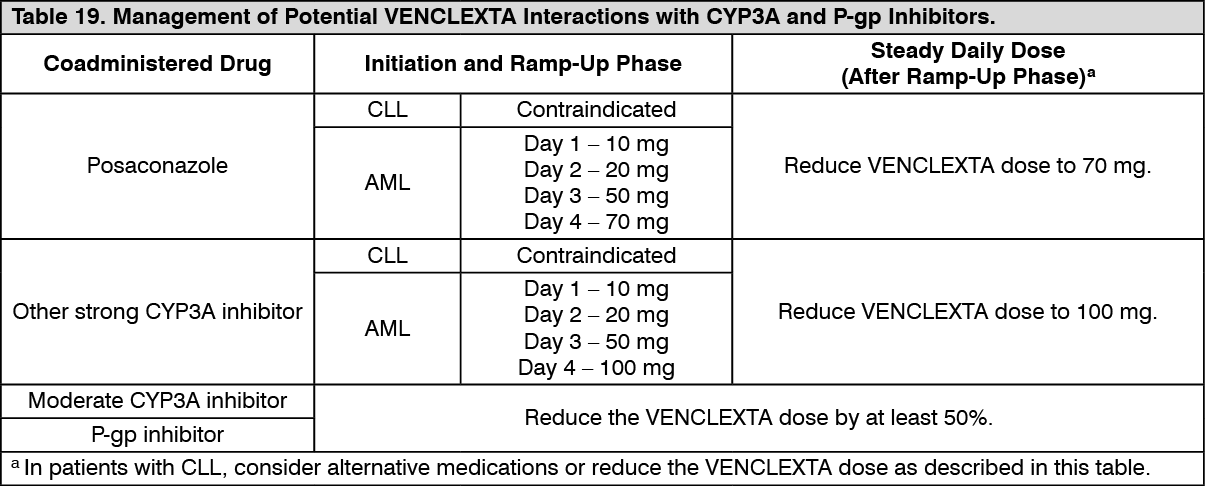
Click on icon to see table/diagram/imageDosage Modifications for Drug Interactions: Strong or Moderate CYP3A Inhibitors or P-gp Inhibitors: Table 19 describes VENCLEXTA contraindication or dosage modification based on concomitant use with a strong or moderate CYP3A inhibitor or a P-gp inhibitor [see Effects of Other Drugs on VENCLEXTA under Interactions] at initiation, during, or after the ramp-up phase.
Resume the VENCLEXTA dosage that was used prior to concomitant use of a strong or moderate CYP3A inhibitor or a P-gp inhibitor 2 to 3 days after discontinuation of the inhibitor [see Effects of Other Drugs on VENCLEXTA under Interactions]. (See Table 19.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDosage Modifications for Patients with Severe Hepatic Impairment: Reduce the VENCLEXTA once daily dose by 50% for patients with severe hepatic impairment (Child-Pugh C); monitor these patients more closely for adverse reactions [see Hepatic Impairment under Precautions].
Administration: Instruct patients of the following: Take VENCLEXTA with a meal and water.
Take VENCLEXTA at approximately the same time each day.
Swallow VENCLEXTA tablets whole. Do not chew, crush, or break tablets prior to swallowing.
If the patient misses a dose of VENCLEXTA within 8 hours of the time it is usually taken, instruct the patient to take the missed dose as soon as possible and resume the normal daily dosing schedule. If a patient misses a dose by more than 8 hours, instruct the patient not to take the missed dose and resume the usual dosing schedule the next day.
If the patient vomits following dosing, instruct the patient to not take an additional dose that day and to take the next prescribed dose at the usual time.