Simulect has been tested in four randomised, double-blind, placebo-controlled studies in renal transplant recipients: in two studies patients were concomitantly treated with ciclosporin for microemulsion and corticosteroids (346 and 380 patients), in one study patients were concomitantly treated with ciclosporin for microemulsion, azathioprine and corticosteroids (340 patients), in one study patients were concomitantly treated with ciclosporin for microemulsion, mycophenolate mofetil and corticosteroids (123 patients).
Simulect has also been compared to a polyclonal anti-T-lymphocyte immunoglobulin preparation (ATG/ALG) in one active-controlled study in renal transplant recipients; all patients were concomitantly treated with ciclosporin for microemulsion, mycophenolate mofetil and corticosteroids (135 patients). Safety data in paediatric patients have been obtained from one open-label pharmacokinetic and pharmacodynamic study in renal transplant recipients (41 patients).
Incidence of Adverse Events: Simulect did not appear to add to the background of adverse events seen in organ transplantation patients as a consequence of their underlying disease and the concurrent administration of immunosuppressants and other medications. In the four placebo-controlled trials, the pattern of adverse events in 590 patients treated with the recommended dose of Simulect was indistinguishable from that in 595 patients treated with placebo. Simulect did not increase the incidence of serious adverse events observed when compared to placebo. The overall incidence of treatment-related adverse events among all patients in the individual studies was not significantly different between the Simulect (7.1% - 40%) and the placebo (7.6% - 39%) treatment groups. In the active-controlled study, fewer Simulect (11.4%) than ATG/ALG (41.5%) patients experienced treatment-related adverse events.
Adult experience: The most commonly reported (> 20%) events following dual or triple therapy in both treatment groups (Simulect vs. Placebo or ATG/ALG) were constipation, urinary tract infection, pain, nausea, peripheral oedema, hypertension, anaemia, headache, hyperkalaemia, hypercholesterolaemia, postoperative wound complication, weight increase, increase in blood creatinine, hypophosphataemia, diarrhoea, upper respiratory tract infection.
Paediatric experience: The most commonly reported (> 20%) events following dual therapy in both (< 35 kg vs. ≥ 35 kg weight) cohorts were urinary tract infection, hypertrichosis, rhinitis, pyrexia, hypertension, upper respiratory tract infection and viral infection, sepsis and constipation.
Incidence of Malignant Neoplasms: The overall incidence of malignancies among all patients in the individual studies was similar between the Simulect and the comparator treatment groups. Overall, lymphoma/lymphoproliferative disease occurred in 0.1% (1/701) of patients in the Simulect group compared with 0.3% (2/595) of placebo and 0% of ATG/ALG patients.
Other malignancies were reported among 1.0% (7/701) of patients in the Simulect group compared with 1.2% (7/595) of placebo and 4.6% (3/65) of ATG/ALG patients.
No differences were found in the incidence of malignancies and LPDs between Simulect 7% (21/295) and placebo 7% (21/291) in a pooled analysis of two five-years extension studies.
Incidence of Infectious Episodes: The overall incidence and profile of infectious episodes among dual and triple therapy patients was similar between the Simulect and the placebo treatment groups (Simulect = 75.9%, Placebo or ATG/ALG = 75.6%). The incidence of serious infections was similar in the Simulect and comparator groups (26.1% vs. 24.8%). The incidence of CMV-infections was similar in both groups (14.6% vs. 17.3%), following either dual or triple therapy regimen.
The incidence and causes of deaths following dual or triple therapy were similar in Simulect (2.9%) and placebo or ATG/ALG groups (2.6%), with the most common cause of deaths in both treatment groups being infections (Simulect = 1.3%, placebo or ATG/ALG = 1.4%). In a pooled analysis of two five-year extension studies the incidence and cause of death remained similar in both treatment groups (Simulect 15%, placebo 11%), the primary cause of death being cardiac-related disorders (Simulect 5%, placebo 4%).
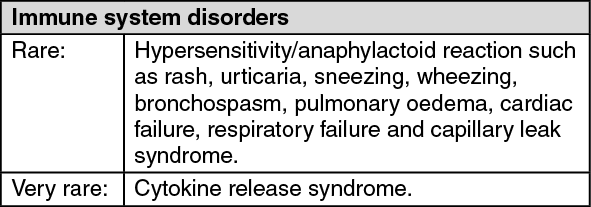
Post-marketing adverse reactions: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
