


 Sign Out
Sign Out



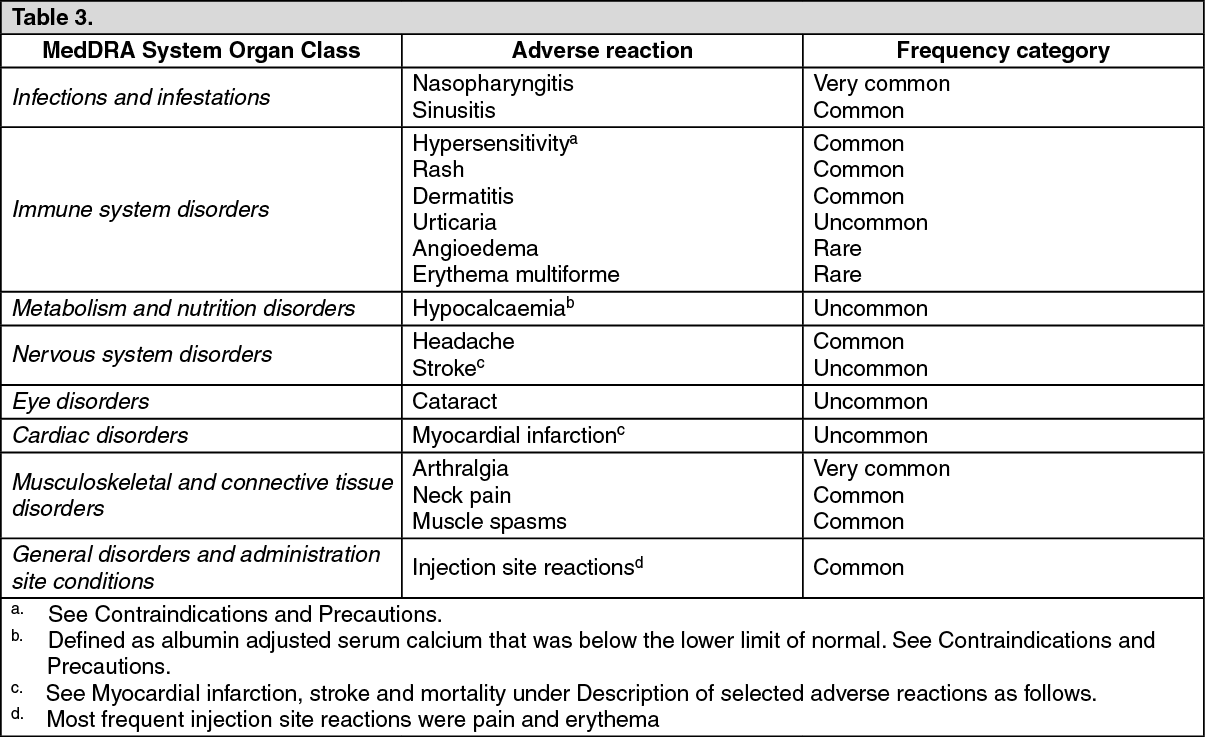
Tabulated list of adverse reactions: The following convention has been used for the classification of the adverse reactions: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000) and very rare (< 1/10,000). Within each frequency grouping and system organ class, adverse reactions are presented in order of decreasing seriousness. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Immunogenicity: In postmenopausal women dosed with monthly romosozumab, the incidence of anti-romosozumab antibodies was 18.6% (1162 of 6244) for binding antibodies and 0.9% (58 of 6244) for neutralizing antibodies. The earliest onset of anti-romosozumab antibodies was 3 months after first dosing. The majority of antibody responses were transient.
The presence of anti-romosozumab binding antibodies decreased romosozumab exposure by up to 25%. No impact on the efficacy of romosozumab was observed in the presence of antiromosozumab antibodies. Limited safety data show that the incidence of injection site reactions was numerically higher in female patients with neutralizing antibodies.
Myocardial infarction, stroke and mortality: In the active-controlled trial of romosozumab for the treatment of severe osteoporosis in postmenopausal women during the 12-month double-blind romosozumab treatment phase, 16 women (0.8%) had myocardial infarction in the romosozumab arm versus 5 women (0.2%) in the alendronate arm and 13 women (0.6%) had stroke in the romosozumab arm versus 7 women (0.3%) in the alendronate arm. These events occurred in patients with and without a history of myocardial infarction or stroke. Cardiovascular death occurred in 17 women (0.8%) in the romosozumab group and 12 (0.6%) women in the alendronate group. The number of women with major adverse cardiac events (MACE = positively adjudicated cardiovascular death, myocardial infarction or stroke) was 41 (2.0%) in the romosozumab group and 22 (1.1%) in the alendronate group, yielding a hazard ratio of 1.87 (95% confidence interval [1.11, 3.14]) for romosozumab compared to alendronate. All-cause death occurred in 30 women (1.5%) in the romosozumab group and 22 (1.1%) women in the alendronate group.
In the placebo-controlled trial of romosozumab for the treatment of osteoporosis in postmenopausal women (including women with severe and less severe osteoporosis) during the 12-month double-blind romosozumab treatment phase, there was no difference in positively adjudicated MACE; 30 (0.8%) occurred in the romosozumab group and 29 (0.8%) in the placebo group. All-cause death occurred in 29 women (0.8%) in the romosozumab group and 24 (0.7%) women in the placebo group.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions as per local regulations.
View ADR Monitoring Form