Gemigliptin tartrate sesquihydrate.
Each tablet contains gemigliptin tartrate sesquihydrate, equivalent to 50 mg gemigliptin.
Excipients/Inactive Ingredients: Tablet core: Microcrystalline cellulose (Type 102), Microcrystalline Cellulose (Type 101), Croscarmellose Sodium, Stearyl Fumarate Sodium, Opadry II 85F43172.
Film coating: Polyvinyl Alcohol, Titanium Dioxide, Polyethylene Glycol 3350, Talc, FD&C Yellow #6/Sunset Yellow FCF Aluminum Lake, Red Iron Oxide.
Pharmacotherapeutic group: Medicines used in diabetes, Dipeptidyl peptidase 4 (DPP-4) inhibitors, ATC code: A10BH06.
Pharmacology: Pharmacodynamics: Mechanism of Action: Zemiglo is a member of a class of oral anti-hyperglycemic agents called dipeptidyl peptidase 4 (DPP-4) inhibitors, which enhances the level of active incretin hormones, including GLP-1 and GIP, thereby reducing blood glucose levels. Active GLP-1 and GIP promote insulin production and release from pancreatic beta cells. GLP-1 also lowers the secretion of glucagon from pancreatic alpha cells, thereby resulting in a decreased hepatic glucose production. However these incretins are rapidly degraded by the DPP-4. Gemigliptin selectively inhibits DPP-4 activity, enhancing prolonged activation of incretin hormones. Gemigliptin demonstrates >3,400-fold and >9,500-fold selectivity versus DPP-9 and DPP-8, respectively.
Clinical Efficacy and Safety: Over 1,500 patients with type 2 diabetes have been included in randomized, controlled clinical trials. Overall, gemigliptin improved glycemic control when used as monotherapy or in combination treatment.
Gemigliptin dose finding: The efficacy and safety of gemigliptin monotherapy was evaluated in a placebo-controlled Phase II study of 12 weeks duration. The mean change in HbA1c from baseline at Week 12 was -0.98%, -0.74% and -0.78% (when adjusted with placebo data, -0.92%, -0.68% and -0.72%) at dosage levels of 50 mg, 100 mg and 200 mg, respectively.
Gemigliptin as monotherapy: The efficacy and safety of gemigliptin monotherapy was evaluated in a placebo-controlled Phase III study of 24 weeks duration. The analysis of covariance (ANCOVA) for HbA1c change from baseline at Week 24 (W24 - W0) showed that placebo-subtracted mean HbA1c change from baseline was -0.705% [95% confidence interval (CI) -1.041% to -0.368%]. Therefore, the clinical efficacy of gemigliptin was demonstrated to be superior to that of the placebo group. The study was extended through Week 52. In the extended part of the study, an analysis of HbA1c change from baseline revealed consistent glycemic control effect of gemigliptin over a period of 52 weeks. Further decrease in HbA1c was observed with continued treatment of gemigliptin 50 mg in the latter 28 weeks and the degree of change from baseline at Week 52 (-0.87%) was still clinically and statistically significant (p<0.0001).
Gemigliptin as add-on to metformin therapy: The efficacy and safety of gemigliptin add-on combination therapy were evaluated in an active-controlled Phase III study of 24 week duration. The ANCOVA for HbA1c change from baseline at Week 24 (W24 - W0) showed that the between–group difference (each regimen group of gemigliptin-sitagliptin group) in the least square (LS) mean change from baseline was 0.056% [90% CI -0.117% to 0.23%] for 50 mg qd group and 0.04% [90% CI -0.121% to 0.2%] for 25 mg bid group. Therefore, the clinical efficacy of gemigliptin was demonstrated to be at least comparable with that of the comparator, sitagliptin. The study was extended through Week 52. In the extended part of the study, the change in HbA1c from baseline was clinically and statistically significant (p<0.0001) throughout the duration of 52 weeks in all treatment groups. The decrease in HbA1c was most prominent at Week 6 followed by further gradual decrease thereafter. Decreased HbA1c level was well maintained in all three groups during the extended 28 weeks.
Gemigliptin as add-on to a combination of metformin and sulphonylurea therapy: The efficacy and safety of gemigliptin triple combination therapy with metformin and sulfonylurea were evaluated in a placebo-controlled Phase III study of 24 weeks duration. An ANCOVA was conducted using the HbA1c value at baseline as a covariate and including the glimepiride reduction as a factor in relation to the change in HbA1c at Week 24. In the main population for analysis, the LS mean of the HbA1c change at Week 24 after study treatment was -0.877±0.166% (p<0.0001) in gemigliptin group and -0.012±0.179% (p=0.9476) in the placebo group, showing a significant reduction compared to the baseline in the gemigliptin group. As the 95% CI for the difference in change between the treatment groups was (-1.092%, -0.638%), i.e., its upper limit was less than 0, the superiority of the gemigliptin was demonstrated.
Gemigliptin and metformin as initial therapy: The efficacy and safety of gemigliptin initial combination therapy with metformin were evaluated in an active-controlled Phase III study of 24 weeks duration. For the change of HbA1c from baseline at Week 24, analysis of covariance was performed. As a result, the 95% CI for between group difference in LS means of HbA1c changes in combination therapy group and each monotherapy group were (-1.02%, -0.63%) in combination therapy group compared with gemigliptin group and (-0.82%, -0.41%) in combination therapy group compared with metformin group, respectively. This showed that the upper limits of both CIs were less than zero (p<0.001), confirming superiority of the combination therapy.
Glycemic variability of gemigliptin versus sitagliptin or glimepiride: The efficacy of gemigliptin on MAGE (mean amplitude of glycemic excursions) and safety of initial combination therapy of gemigliptin versus sitagliptin or glimepiride with metformin in patients with type 2 diabetes were evaluated in a multicenter, randomized, active-controlled, parallel group, open-label, exploratory study. The change in MAGE at Week 12 was -43.11 mg/dL, -38.27 mg/dL and -21.74 mg/dL in the gemigliptin and metformin group, sitagliptin and metformin group and glimepiride and metformin group, respectively. As a result of testing the differences between the groups, DPP-4 inhibitors, i.e., the gemigliptin and metformin group and sitagliptin and metformin group, reduced the MAGE compared to sulfonylurea, i.e., glimepiride and metformin group (gemigliptin: p=0.0306, sitagliptin: p=0.0292).
Gemigliptin therapy in patients with renal impairment: The efficacy and safety of gemigliptin monotherapy or its combination therapy with insulin and sulfonylurea in type 2 diabetes patients with moderate or severe renal impairment were evaluated in a double-blind study for 52 weeks duration. The change in HbA1c at Week 12 was -0.96% and 0.21% in the gemigliptin and placebo groups, respectively, showing significant difference between the groups (p<0.0001). Adjusted mean difference between the groups was -1.20% with two sided 95% CI of -1.53 to -0.87%. The upper limit of the 95% CI for the difference in HbA1c change (HbA1c at week 12 - HbA1c at week 0) between groups was lower than 0, which demonstrates the superiority of the gemigliptin over the placebo. The efficacy of gemigliptin was maintained for 52 weeks.
Gemigliptin as add-on to insulin (+/- metformin) therapy: The efficacy and safety of gemigliptin added-on to insulin alone or insulin in combination with metformin in patients with type 2 diabetes were evaluated in a randomized, placebo-controlled, parallel-group, double-blind, phase III study of 24 weeks duration. The primary efficacy endpoint was analysed using an ANCOVA model, with metformin use and country as fixed factors and baseline value as a covariate. In the full analysis set, the LS mean (SE) change from baseline HbA1c after 24 weeks was -0.816% (0.1150%) with gemigliptin and -0.131% (0.1357%) with placebo. The between group difference was -0.685%, and its 95% CI was (-0.941%, -0.429%). The upper limit of the 95% CI for the between group difference in HbA1c changes was less than 0, suggesting superior glycemic control of the gemigliptin compared to the placebo.
The data collected in clinical studies demonstrated that gemigliptin was well tolerated and displayed an overall safety profile that is at least comparable with that of the comparator.
Geriatric: Of the total number of subjects (N=1,473) in Phase II and III clinical studies of gemigliptin, 243 patients (16.5%) were 65 years and over. The efficacy and safety of gemigliptin were not different between young and elderly patients. However, Zemiglo should be used with caution in elderly patient because physiological functions including liver and kidney are usually decreased in this population.
Pharmacokinetics: Absorption: Following a single oral administration of gemigliptin to healthy subjects, gemigliptin was rapidly absorbed, with Tmax occurring 1 to 5 hours post-dose. At the recommended dose of 50 mg, Cmax and AUC were 62.7 ng/mL and 743.1 ng·hr/mL, respectively. The system exposure was increased in a dose-proportional manner in the range of 50~400 mg.
Distribution: In vitro human plasma protein binding is 29% for gemigliptin and 35%~48% for the metabolites including major active metabolite.
Biotransformation: The responsible enzyme for the metabolism of gemigliptin is CYP3A4. In plasma, gemigliptin and the major metabolite (LC15-0636) accounted for 65%~100% and 0%~17.5% of the sample radioactivity. LC15-0636, a hydroxylated metabolite of gemigliptin, is pharmacologically active and two times more potent than gemigliptin. In vitro studies indicated that gemigliptin is not an inhibitor of CYP1A2, 2A6, 2B6, 2C9, 2C19, 2D6, 2E1 or 3A4 and is not an inducer CYP1A2, 2C8, 2C9, 2C19, or 3A4. Therefore, gemigliptin is considered unlikely to cause interactions with other drugs that utilize these metabolic pathways.
Elimination: Following oral administration of [14C] gemigliptin to healthy subjects, the administered radioactivity was recovered in feces (27%) or urine (63%). The elimination half-life after oral administration is approximately 17 hr and 24 hr for gemigliptin and LC15-0636, respectively.
Renal Impairment: The influence of renal impairment on the pharmacokinetics of gemigliptin has been evaluated. In patients with mild (CrCl: 50~80 mL/min), moderate (CrCl: 30~50 mL/min), severe (CrCl: <30 mL/min) and end stage renal disease (on hemodialysis), AUCinf increased 1.20-, 2.04-, 1.50- and 1.69-fold for gemigliptin and 0.91-, 2.17-, 3.07- and 2.66-fold for LC15-0636, when compared with the normal kidney function group. Overall active moiety, the sum of gemigliptin and LC15-0636, was increased less than or approximately 2-fold in patients with moderate and severe renal impairment.
Hepatic Impairment: The influence of hepatic impairment on the pharmacokinetics of gemigliptin has been evaluated. In mild and moderate hepatic impairment, exposure to gemigliptin (AUC) after single dosing was 50% and 80% higher than in healthy subjects. Formation of LC15-0636, a metabolite of gemigliptin, was only slightly affected by mild hepatic impairment (5% to 10% lower), while in moderate hepatic impairment, formation of LC15-0636 was about 30% lower compared to healthy subjects. Urinary excretion parameters were not markedly influenced by hepatic impairment, so the decrease in total clearance of gemigliptin observed in hepatic impairment is due a decreased metabolization rate of gemigliptin. Half-lives of gemigliptin and of LC15-0636 were slightly increased in hepatic impairment.
In mild and moderate hepatic impairment, inhibition of DPP-4 was slightly decreased compared to healthy subjects (5% to 10%), however, neither the effect on AUEC nor on Emax of DPP-4 inhibition was statistically significant. It is expected that dose adjustment would not be required in mild and moderate hepatic impairment based on the efficacy and safety profile of gemigliptin in clinical and non-clinical studies.
Gender: No dose adjustment is necessary based on gender. The differences in Cmax and AUCinf were not clinically significant.
Race: Caucasian subjects demonstrated 28% decrease in Cmax and 5% decrease in AUCinf when compared with Korean subjects.
Toxicology: Preclinical safety data: A two-year carcinogenicity study was conducted in male and female rats given oral doses of gemigliptin of 50, 150, and 450 mg/kg/day. No evidence of carcinogenicity with gemigliptin was found in either male or female rats. This dose results in exposures approximately 129~170 times the human exposure at the maximum recommended daily adult human dose (MRHD) of 50 mg/day based on AUC comparisons. A 6-month carcinogenicity study has been performed in TgrasH2 transgenic mice at doses of 200, 400, and 800 mg/kg/day in males and 200, 600, 1200 mg/kg/day in females. There was no evidence of carcinogenicity with gemigliptin at a dose of 1200 mg/kg/day, approximately 87 times the human exposure at the maximum recommended daily dose.
Genotoxicity assessments in the Ames test, chromosomal aberrations test and in vivo micronucleus tests in mice and rats were negative.
The fertility of gemigliptin was not affected at dose of 800 mg/kg/day in rat. Gemigliptin was not teratogenic up to 200 mg/kg/day in rats and 300 mg/kg/day in rabbits, which are respectively 83 and 153 times human exposure at the MRHD of 50 mg/day.
Gemigliptin at dose of 800 mg/kg/day in rat, approximately 264 times human exposure at the MRHD of 50 mg/day, increased the incidence of fetus cleft palate malformation, dilated renal pelvis, misshapen thymus and sternoschisis, with increasing dose.
Zemiglo 50 mg is a dipeptidyl peptidase-4 (DPP-4) inhibitor indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.
Zemiglo 50 mg can be administered as monotherapy or in combination with metformin as initial therapy in treatment of naive patients with inadequate glycemic control by diet and exercise; metformin as patients with inadequate glycemic control with maximal tolerated dose of metformin alone; metformin and sulfonylurea in patients with inadequate glycemic control with the maximal tolerated dose of metformin and sulfonylurea dual therapy; insulin (with or without metformin) in patients with inadequate glycemic control with the stable dose of insulin.
Posology: Adults: The maximum daily recommended dose of Zemiglo is 50 mg once daily. If a dose is missed, it should be taken as soon as the patient remembers. A double dose should not be taken on the same day.
When used in combination with a sulfonylurea or insulin, a lower dose of the sulfonylurea or insulin may be required to reduce the risk of hypoglycaemia (see Precautions).
Additional information on special populations: Renal impairment: For patients with renal impairment, no dose adjustment is required (see Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions).
Hepatic Impairment: No dose adjustment is necessary for patients with mild or moderate hepatic impairment. There is no clinical experience in patients with severe hepatic impairment. Therefore, caution should be exercised in this population (see Pharmacology: Pharmacokinetics under Actions).
Elderly: The efficacy and safety of gemigliptin were not different between young and elderly patients. However, Zemiglo should be used with caution in elderly patient because physiological functions including liver and kidney are usually decreased in this population (see Pharmacology: Pharmacodynamics under Actions).
Pediatric Population: Safety and effectiveness in children and adolescents less than 18 years of age have not been established.
Method of Administration: Zemiglo can be taken with or without food.
During clinical trials in healthy subjects, multiple doses of up to 600 mg gemigliptin were administered for duration of 10 days. One case of increased heartbeat was observed at a single dose of 600 mg gemigliptin. There is no experience with daily doses above 600 mg in clinical studies. In the event of an overdose, it is reasonable to employ the usual supportive measures, e.g., remove unabsorbed material from the gastrointestinal tract, employ clinical monitoring (including obtaining an electrocardiogram), and institute supportive therapy as indicated by the patient's clinical status.
Zemiglo is contraindicated in patients with a history of serious hypersensitivity reactions, i.e., angioedema or anaphylaxis, to another dipeptidyl peptidase-4 (DPP-4) inhibitor (see Adverse Reactions); Type 1 diabetes or diabetic ketoacidosis.
Do not use in patient with history of hypersensitivity to gemigliptin.
Do not use in patient type 1 diabetes mellitus, diabetic ketoacidosis, severe infection or accident-related severe injury.
Patient should avoid taking gemigliptin with alcohol beverage.
Gemigliptin may possible cause of severe joint pain.
Renal Impairment: No adjustment is required (see Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions).
Cardiac Impairment: There is limited clinical experience in patients with New York Heart Association (NYHA) Class I cardiac status. Therefore, gemigliptin should be used with caution in this population. Zemiglo is not recommended in patients with NYHA Class II~IV cardiac status.
Hepatic Impairment: No dose adjustment is necessary for patients with mild or moderate hepatic impairment. There is no clinical experience in patients with severe hepatic impairment. Therefore, caution should be exercised in this population.
Hypersensitive Reaction: Care should be taken when administering in patients with allergic and hypersensitive reactions to any of the ingredients in Zemiglo (see Adverse Reactions).
Acute Pancreatitis: Pancreatitis has been reported in patients taking Zemiglo. Therefore, patients should be informed of the characteristic symptoms of acute pancreatitis: persistent, severe abdominal pain. If pancreatitis is suspected, gemigliptin should be discontinued and should not be restarted. Caution should be exercised in patients with a history of pancreatitis.
Use with Medicinal Products Known to Cause Hypoglycemia: Sulfonylurea or insulin is known to cause hypoglycemia. Therefore, a lower dose of sulfonylurea or insulin may be required to reduce the risk of hypoglycemia when used in combination with Zemiglo.
Severe and Disabling Arthralgia: There have been postmarketing reports of severe and disabling arthralgia in patients taking other DPP-4 inhibitors. The time to onset of symptoms following initiation of drug therapy varied from one day to years. Patients experienced relief of symptoms upon discontinuation of the medication. A subset of patients experienced a recurrence of symptoms when restarting the same drug or a different DPP-4 inhibitor. Consider DPP-4 inhibitors as a possible cause for severe joint pain and discontinue drug if appropriate.
Excipient warnings: Gemigliptin tablet contains sunset yellow FCF which may cause allergic reactions.
Effects on ability to drive and use machines: Zemiglo has no known influence on the ability to drive and use machines. However, when driving or using machines, it should be taken into account that dizziness has been reported. In addition, patients should be alerted to the risk of hypoglycemia when Zemiglo is used in combination with other antidiabetic medicinal products known to cause hypoglycemia (e.g. sulfonylureas, insulin).
Use in Pregnancy & Lactation: Pregnant women should avoid using gemigliptin and breastfeeding women should use with caution.
Pregnancy: There are no adequate and well-controlled studies in pregnant women with gemigliptin; therefore, use of gemigliptin is not recommended during pregnancy.
Lactation: There is no information on excretion of gemigliptin into human milk. Animal studies have shown excretion of gemigliptin in breast milk. Zemiglo should not be used during breast-feeding.
Summary of the safety profile: There were 1,468 patients with type 2 diabetes, including 1,080 patients treated with gemigliptin, randomized in 5 double-blind and 1 open-label controlled clinical safety and efficacy studies conducted to evaluate the effects of gemigliptin on glycemic control.
The overall incidence of adverse events in patients treated with gemigliptin was similar to placebo and active-control group.
Discontinuation of therapy due to adverse events was similar in patients who received gemigliptin as compared to placebo (1.4% as compared to 0.8%).
Across all the clinical studies, there was no serious adverse event (SAE) related to gemigliptin.
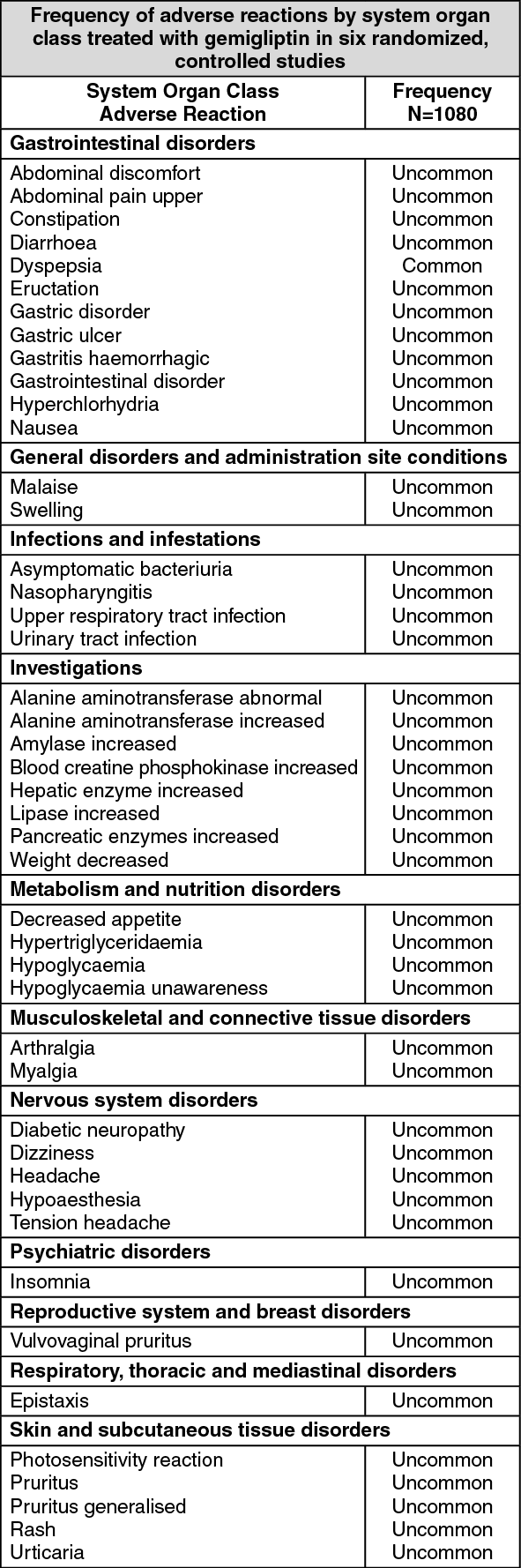
Tabulated list of adverse reactions: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The table presents adverse reactions which have been reported during 6 randomized, controlled clinical studies. The adverse reactions are listed by SOC (system organ class) and PT (Preferred Term) with frequency. Frequencies are defined as Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1,000), not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions: Hypoglycemia:
Click on icon to see table/diagram/image
Description of selected adverse reactions: Hypoglycemia: In six randomized controlled studies of gemigliptin, 15 patients (1.4%) reported hypoglycemia. The hypoglycemia experienced by patients in clinical trials was considered mostly of mild in intensity and patients fully recovered.
Hypersensitivity: In the active-controlled add-on combination study (gemigliptin as add-on to metformin therapy), two patients (1.71%) receiving 25 mg gemigliptin twice daily on a stable dose of metformin in the first 24-weeks and 50 mg once daily in the latter 28 weeks reported anaphylactic reactions, which was not related to gemigliptin (see Contraindications and Precautions).
In vitro assessment of interactions: The responsible enzyme for the metabolism of gemigliptin is CYP3A4. In vitro studies indicated that gemigliptin and its active metabolite are not an inhibitor of CYP1A2, 2A6, 2B6, 2C9, 2C19, 2D6, 2E1 or 3A4 and are not an inducer of CYP1A2, 2C8, 2C9, 2C19, or 3A4. Therefore, gemigliptin is unlikely to cause interactions with other drugs that utilize these metabolic pathways. In vitro studies further indicated that gemigliptin did not induce P-glycoprotein (P-gp) while mildly inhibited P-gp mediated transport at high concentration. Therefore, gemigliptin is unlikely to cause interactions with other P-gp substrates at therapeutic concentrations.
In vivo assessment of interactions: Effects of gemigliptin on other medicinal products: In clinical studies, gemigliptin did not meaningfully alter the pharmacokinetics of metformin, pioglitazone, glimepiride, rosuvastatin, dapagliflozin, and empagliflozin providing in vivo evidence of a low propensity for causing drug interactions with substrates of CYP2C8, CYP2C9, CYP3A4 and organic cation transporter (OCT), and UDP-glucuronosyltransferase (UGT).
Metformin: Repeated co-administration of 50 mg gemigliptin with 2000 mg metformin, a substrate of OCT1 and OCT2, decreased the Cmax of metformin by 13% but did not affect the AUC of metformin at steady state.
Pioglitazone: Repeated co-administration of 200 mg gemigliptin with 30 mg pioglitazone, a substrate of CYP2C8 and 3A4, decreased the AUC and Cmax of pioglitazone by 15% and 17%, respectively. However, those of the active metabolites of pioglitazone were not changed at steady state.
Glimepiride: Co-administration of multiple doses of 50 mg gemigliptin with a single dose of 4 mg glimepiride, a substrate of CYP2C9, did not meaningfully alter the pharmacokinetics of glimepiride at steady state.
Rosuvastatin: Repeated co-administration of 50 mg gemigliptin with 20 mg rosuvastatin, a substrate of CYP2C9 and 3A4, did not meaningfully alter the pharmacokinetics of rosuvastatin at steady state.
Dapagliflozin: Repeated co-administration of 50 mg gemigliptin with 10 mg of dapagliflozin, substrate of UGT1A9, did not meaningfully alter the pharmacokinetics of dapagliflozin at steady state.
Empagliflozin: Repeated co-administration of 50 mg gemigliptin with 25 mg of empagliflozin, substrate of UGT2B7, UGT1A3, UGT1A8, and UGT1A9, did not meaningfully alter the pharmacokinetics of empagliflozin at steady state.
Effects of other medical products on gemigliptin: In clinical studies, metformin, pioglitazone, rosuvastatin, dapagliflozin, and empagliflozin did not meaningfully alter the pharmacokinetics of gemigliptin. Ketoconazole did not meaningfully alter the pharmacokinetics of gemigliptin and its active metabolite. Therefore, strong and moderate CYP3A4 inhibitors would not cause clinically meaningful drug interactions. Rifampicin (rifampin), on the other hand, significantly decreased exposure of gemigliptin. Therefore, co-administration with other strong CYP3A4 inducers, including rifampicin (rifampin), dexamethasone, phenytoin, carbamazepine, rifabutin and phenobarbital, is not recommended.
Metformin: Repeated co-administration of 50 mg gemigliptin with 2000 mg metformin did not meaningfully alter the pharmacokinetics of gemigliptin at steady state.
Pioglitazone: Repeated co-administration of 200 mg gemigliptin with 30 mg of pioglitazone did not meaningfully alter the pharmacokinetics of gemigliptin and its active metabolite at steady state.
Ketoconazole: Co-administration of multiple doses of 400 mg ketoconazole once daily, a strong inhibitor of CYP3A4, with a single dose of 50 mg gemigliptin increased the AUC of active moiety, the sum of gemigliptin and its active metabolite, by 1.9-fold at steady state.
Rifampicin: Co-administration of multiple doses of 600 mg rifampicin once daily, a strong inducer of CYP3A4, with a single dose of 50 mg gemigliptin, decreased the AUC and Cmax of gemigliptin by 80% and 59%, respectively. The Cmax of active metabolite of gemigliptin was not significantly affected while the AUC was decreased by 36% at steady state.
Rosuvastatin: Repeated co-administration of 50 mg gemigliptin with 20 mg rosuvastatin did not meaningfully alter the pharmacokinetics of gemigliptin at steady state.
Dapagliflozin: Repeated co-administration of 50 mg gemigliptin with 10 mg of dapagliflozin did not meaningfully alter the pharmacokinetics of gemigliptin at steady state.
Empagliflozin: Repeated co-administration of 50 mg gemigliptin with 25 mg of empagliflozin did not meaningfully alter the pharmacokinetics of gemigliptin at steady state.
Incompatibilities: Not applicable.
Special precautions for disposal and other handling: Any unused product or waste material should be disposed of in accordance with local requirements.
Store below 30°C in tight container.
Shelf-life: 48 months.
A10BH06 - gemigliptin ; Belongs to the class of dipeptidyl peptidase 4 (DPP-4) inhibitors. Used in the treatment of diabetes.
Zemiglo FC tab 50 mg
28's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
