The following adverse reactions are discussed in greater detail in other sections of the labeling: Immune-mediated enterocolitis/colitis [see Immune-mediated Enterocolitis/Colitis under Precautions].
Immune-mediated hepatitis [see Immune-mediated Hepatitis under Precautions].
Immune-mediated dermatitis/skin adverse reactions [see Immune-mediated Dermatitis/Skin Adverse Reactions under Precautions].
Immune-mediated neuropathies [see Immune-mediated Neuropathies under Precautions].
Immune-mediated endocrinopathies [see Immune-mediated Endocrinopathies under Precautions].
Immune-mediated pneumonitis [see Immune-Mediated Pneumonitis under Precautions].
Immune-mediated nephritis and renal dysfunction [see Immune-Mediated Nephritis and Renal Dysfunction under Precautions].
Immune-mediated encephalitis [see Immune-Mediated Encephalitis under Precautions].
Infusion reactions [see Infusion-Related Reactions under Precautions].
Other immune-mediated adverse reactions, including ocular manifestations [see Other Immune-mediated Adverse Reactions, Including Ocular Manifestations under Precautions].
Embryo-fetal toxicity [see Use in Pregnancy: Embryo-fetal Toxicity under Precautions].
Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, the adverse reaction rates observed cannot be directly compared with rates in other clinical trials or experience with therapeutics in the same class and may not reflect the rates observed in clinical practice.
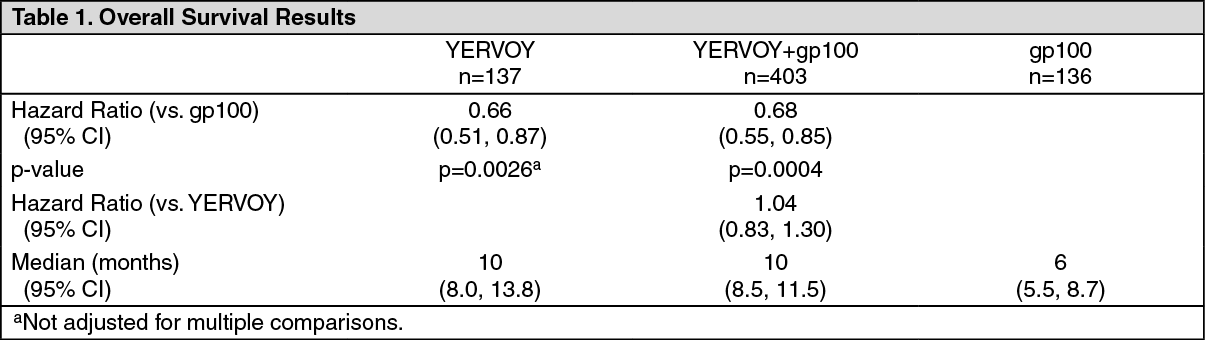
Unresectable or Metastatic Melanoma: The clinical development program excluded patients with active autoimmune disease or those receiving systemic immunosuppression for organ transplantation. Exposure to YERVOY 3 mg/kg for 4 doses given by intravenous infusion in previously treated patients with unresectable or metastatic melanoma was assessed in a randomized, double-blind clinical study (Study MDX010-20). [See PHARMACOLOGY: CLINICAL STUDIES under Actions.] One hundred thirty-one patients (median age 57 years, 60% male) received YERVOY as a single agent, 380 patients (median age 56 years, 61% male) received YERVOY with an investigational gp100 peptide vaccine (gp100), and 132 patients (median age 57 years, 54% male) received gp100 peptide vaccine alone. Patients in the study received a median of 4 doses (range: 1-4 doses). YERVOY was discontinued for adverse reactions in 10% of patients.
The most common adverse reactions (≥5%) in patients who received YERVOY at 3 mg/kg were fatigue, diarrhea, pruritus, rash, and colitis.
Table 7 presents selected adverse reactions from Study MDX010-20, which occurred in at least 5% of patients in the YERVOY-containing arms and with at least 5% increased incidence over the control gp100 arm for all-grade events and at least 1% incidence over the control group for Grade 3-5 events. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Table 8 presents the per-patient incidence of severe, life-threatening or fatal immune-mediated adverse reactions from Study MDX010-20. (See Table 8.)
Click on icon to see table/diagram/image
Based on the experience in the entire clinical program for melanoma, the incidence and severity of enterocolitis and hepatitis appear to be dose dependent.
Adverse reactions reported in patients treated with YERVOY 3 mg/kg in clinical trials are presented in Table 9.
These reactions are presented by system organ class and by frequency. Frequencies are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). Rates of immune-related adverse reactions in HLA-A2*0201-positive patients who received YERVOY in MDX010-20 were similar to those observed in the overall clinical program.
The safety profile of YERVOY 3 mg/kg in chemotherapy-naïve patients pooled across Phase 2 and 3 clinical trials (N=75; treated) and in treatment-naïve patients in a retrospective observational study (N=120) was similar to that in previously-treated advanced melanoma. (See Table 9.)
Click on icon to see table/diagram/image
Additional adverse reactions not listed in Table 9 have been reported in patients who received other doses (either < or > 3 mg/kg) of YERVOY in clinical trials of melanoma. These additional reactions occurred at a frequency of <1%: meningism, myocarditis, pericardial effusion (pericarditis), cardiomyopathy, autoimmune hepatitis, erythema multiforme, autoimmune nephritis, autoimmune thyroiditis, hyperpituitarism, secondary adrenocortical insufficiency, hypoparathyroidism, thyroiditis, episcleritis, blepharitis, eye oedema, scleritis, temporal arteritis, Raynaud's phenomenon, proctitis, palmar-plantar erythrodysaesthesia syndrome, psoriasis, hematuria, proteinuria, decreased blood thyroid stimulating hormone, decreased blood gonadotrophin, decreased thyroxine, leukopenia, polycythaemia, myasthenia gravis-like symptoms, cytokine release syndrome, sarcoidosis, neurosensory hypoacusis, autoimmune central neuropathy (encephalitis), myositis, polymyositis, and ocular myositis.
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) has been very rarely reported with YERVOY in post-marketing use.
Previously Untreated Renal Cell Carcinoma: The safety of nivolumab 3 mg/kg, administered with YERVOY 1 mg/kg was evaluated in CHECKMATE-214, a randomized open-label trial in which 1082 patients with previously untreated advanced RCC received nivolumab 3 mg/kg in combination with YERVOY 1 mg/kg every 3 weeks for 4 doses followed by nivolumab monotherapy at the 3 mg/kg dose (n=547) every 2 weeks or sunitinib administered orally 50 mg daily for 4 weeks followed by 2 weeks off, every cycle (n=535) [see PHARMACOLOGY: CLINICAL STUDIES under Actions]. The median duration of treatment was 7.9 months (range: 1 day to 21.4+ months) in nivolumab plus YERVOY-treated patients and 7.8 months (range: 1 day to 20.2+ months) in sunitinib-treated patients. In this trial, 57% of patients in the nivolumab plus YERVOY arm were exposed to treatment for greater than 6 months, and 38% of patients were exposed to treatment for greater than 1 year.
Study therapy was discontinued for adverse reactions in 31% of nivolumab plus YERVOY patients and in 21% of sunitinib patients. Fifty-four percent (54%) of patients receiving nivolumab plus YERVOY and 43% of patients receiving sunitinib had a drug delay for an adverse reaction. In the sunitinib group, 53% of patients required a dose reduction; dose reductions were not permitted in the nivolumab plus YERVOY treatment group. Serious adverse reactions occurred in 59% of patients receiving nivolumab plus YERVOY and in 43% of patients receiving sunitinib. The most frequent serious adverse reactions reported in at least 2% of patients treated with nivolumab plus YERVOY were diarrhea, pyrexia, pneumonia, pneumonitis, hypophysitis, acute kidney injury, dyspnea, adrenal insufficiency, and colitis; in patients treated with sunitinib, they were pneumonia, pleural effusion, and dyspnea.
The most common adverse reactions (reported in at least 20% of nivolumab plus YERVOY-treated patients) were fatigue, rash, diarrhea, musculoskeletal pain, pruritus, nausea, cough, pyrexia, arthralgia, and decreased appetite. Table 10 summarizes adverse reactions that occurred in greater than 15% of nivolumab plus YERVOY-treated patients. (See Table 10.)
Click on icon to see table/diagram/image
The most common laboratory abnormalities which have worsened compared to baseline in ≥30% of nivolumab plus YERVOY-treated patients include increased lipase, anemia, increased creatinine, increased ALT, increased AST, hyponatremia, increased amylase, and lymphopenia. Table 11 summarizes the laboratory abnormalities that occurred in greater than 15% of nivolumab plus YERVOY-treated patients. (See Table 11.)
Click on icon to see table/diagram/image
First-line Treatment of Unresectable Malignant Pleural Mesothelioma:
In Combination with Nivolumab: The safety of YERVOY in combination with nivolumab was evaluated in CHECKMATE-743, a randomized, open-label trial in patients with previously untreated unresectable malignant pleural mesothelioma [see PHARMACOLOGY: CLINICAL STUDIES under Actions]. Patients received either YERVOY 1 mg/kg over 30 minutes by intravenous infusion every 6 weeks and nivolumab 3 mg/kg over 30 minutes by intravenous infusion every 2 weeks for up to 2 years; or platinum-doublet chemotherapy for up to 6 cycles. The median duration of therapy in YERVOY and nivolumab-treated patients was 5.6 months (range: 0 to 26.2 months); 48% of patients received YERVOY and nivolumab for >6 months and 24% of patients received YERVOY and nivolumab for >1 year.
Serious adverse reactions occurred in 54% of patients who were treated with YERVOY in combination with nivolumab. The most frequent (≥2%) serious adverse reactions were pneumonia, pyrexia, diarrhea, pneumonitis, pleural effusion, dyspnea, acute kidney injury, infusion-related reaction, musculoskeletal pain, and pulmonary embolism. Fatal adverse reactions occurred in 4 (1.3%) patients and included pneumonitis, acute heart failure, sepsis, and encephalitis.
Both YERVOY and nivolumab were permanently discontinued due to adverse reactions in 23% of patients and 52% had at least one dose withheld due to an adverse reaction. An additional 4.7% of patients permanently discontinued YERVOY alone due to adverse reactions.
The most common (≥20%) adverse reactions were fatigue, musculoskeletal pain, rash, diarrhea, dyspnea, nausea, decreased appetite, cough, and pruritus.
Tables 12 and 13 summarize adverse reactions and laboratory abnormalities, respectively, in CHECKMATE-743. (See Tables 12 and 13.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Postmarketing Experience: The following adverse reactions have been identified during post approval use of YERVOY. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Blood and lymphatic system disorders: hemophagocytic lymphohistiocytosis (HLH).
Immune system disorders: graft-versus-host disease, solid organ transplant rejection.
Skin and Subcutaneous Tissue Disorders: Drug reaction with eosinophilia and systemic symptoms (DRESS syndrome).
Immunogenicity: As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to ipilimumab in the studies described as follows with the incidences of antibodies in other studies or to other products may be misleading.
In clinical studies, 1.1% of 1024 evaluable patients tested positive for binding antibodies against ipilimumab in an electrochemiluminescent (ECL) based assay. This assay has substantial limitations in detecting anti-ipilimumab antibodies in the presence of ipilimumab. Infusion-related or peri-infusional reactions consistent with hypersensitivity or anaphylaxis were not reported in these 11 patients nor were neutralizing antibodies against ipilimumab detected.
Because trough levels of ipilimumab interfere with the ECL assay results, a subset analysis was performed in the dose cohort with the lowest trough levels. In this analysis, 6.9% of 58 evaluable patients, who were treated with 0.3 mg/kg dose, tested positive for binding antibodies against ipilimumab.
Of the patients who were treated with ipilimumab and nivolumab and evaluable for the presence of anti-ipilimumab antibodies, the incidence of anti-ipilimumab antibodies was 6.3% and there were no patients with neutralizing antibodies against ipilimumab with nivolumab 3 mg/kg followed by ipilimumab 1 mg/kg every 3 weeks. There was no evidence of increased incidence of infusion reactions in the presence of anti-ipilimumab antibodies. Of patients evaluable for the presence of anti-nivolumab antibodies, the incidence of anti-nivolumab antibodies was 26.0% and the incidence of neutralizing antibodies against nivolumab was 0.5% with nivolumab 3 mg/kg followed by ipilimumab 1 mg/kg every 3 weeks.
Of 271 patients evaluable for anti-ipilimumab antibodies in CHECKMATE-743, 13.7% were positive for anti-ipilimumab antibodies and 0.4% were positive for anti-ipilimumab neutralizing antibodies. Of 269 patients evaluable for anti-nivolumab antibodies in CHECKMATE-743, 25.7% were positive for anti-nivolumab antibodies and 0.7% had neutralizing antibodies against nivolumab.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image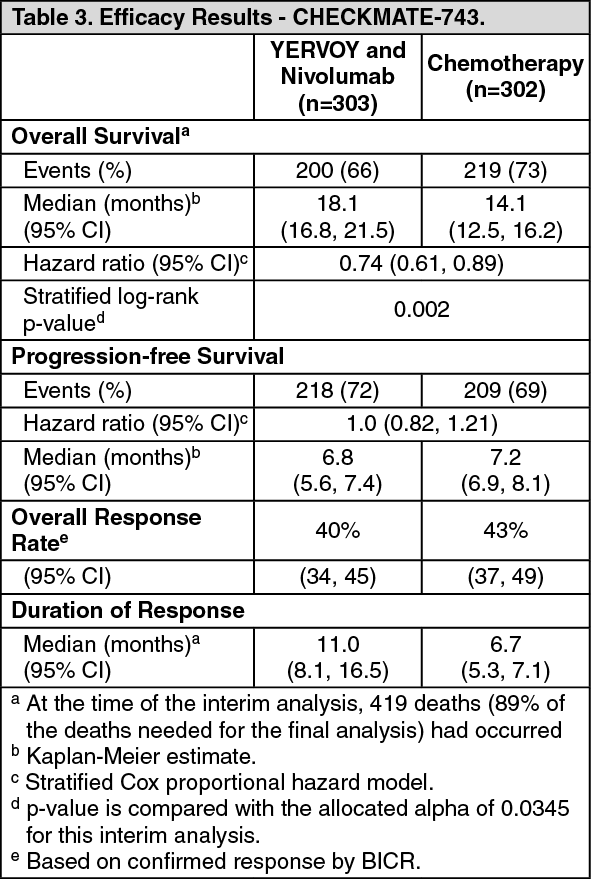 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
