Pharmacotherapeutic group: Antiviral for systemic use, nucleoside and nucleotide reverse transcriptase inhibitors.
ATC code: J05AF13.
Pharmacology: Pharmacodynamics: Mechanism of action: Tenofovir alafenamide is a phosphonamidate prodrug of tenofovir (2'-deoxyadenosine monophosphate analogue). Tenofovir alafenamide enters primary hepatocytes by passive diffusion and by the hepatic uptake transporters OATP1B1 and OATP1B3. Tenofovir alafenamide is primarily hydrolyzed to form tenofovir by carboxylesterase 1 in primary hepatocytes. Intracellular tenofovir is subsequently phosphorylated to the pharmacologically active metabolite tenofovir diphosphate. Tenofovir diphosphate inhibits HBV replication through incorporation into viral DNA by the HBV reverse transcriptase, which results in DNA chain termination.
Tenofovir has activity that is specific to hepatitis B virus and human immunodeficiency virus (HIV-1 and HIV-2). Tenofovir diphosphate is a weak inhibitor of mammalian DNA polymerases that include mitochondrial DNA polymerase γ and there is no evidence of mitochondrial toxicity
in vitro based on several assays including mitochondrial DNA analyses.
Antiviral activity: The antiviral activity of tenofovir alafenamide was assessed in HepG2 cells against a panel of HBV clinical isolates representing genotypes A-H. The EC50 (50% effective concentration) values for tenofovir alafenamide ranged from 34.7 to 134.4 nM, with an overall mean EC50 of 86.6 nM. The CC50 (50% cytotoxicity concentration) in HepG2 cells was > 44400 nM.
Resistance: In a pooled analysis of patients receiving Tenofovir Alafenamide tablets, sequence analysis was performed on paired baseline and on treatment HBV isolates for patients who either experienced virologic breakthrough (2 consecutive visits with HBV DNA ≥ 69 IU/mL after having been < 69 IU/mL, or 1.0 log10 or greater increase in HBV DNA from nadir) through Week 48, or had HBV DNA ≥ 69 IU/mL at early discontinuation at or after Week 24. No amino acid substitutions associated with resistance to Tenofovir Alafenamide tablets were identified in 20 paired isolates.
Cross-resistance: The antiviral activity of tenofovir alafenamide was evaluated against a panel of isolates containing nucleos(t)ide reverse transcriptase inhibitor mutations in HepG2 cells. HBV isolates expressing the rtV173L, rtL180M, and rtM204V/I substitutions associated with resistance to lamivudine remained susceptible to tenofovir alafenamide (< 2-fold change in EC50). HBV isolates expressing the rtL180M, rtM204V plus rtT184G, rtS202G, or rtM250V substitutions associated with resistance to entecavir remained susceptible to tenofovir alafenamide. HBV isolates expressing the rtA181T, rtA181V, or rtN236T single substitutions associated with resistance to adefovir remained susceptible to tenofovir alafenamide; however, the HBV isolate expressing rtA181V plus rtN236T exhibited reduced susceptibility to tenofovir alafenamide (3.7-fold change in EC50). The clinical relevance of these substitutions is not known.
Clinical data: From the clinical study of Vemlidy (tenofovir alafenamide): The efficacy and safety of tenofovir alafenamide tablets in patients with chronic hepatitis B are based on 48-week data from two randomized, double-blind, active-controlled studies, GS-US-320-0108 ("Study 108") and GS-US-320-0110 ("Study 110"): In Study 108, HBeAg-negative treatment-naïve and treatment-experienced patients with compensated liver function were randomized in a 2:1 ratio to receive tenofovir alafenamide tablets (25 mg; N = 285) once daily or tenofovir disoproxil fumarate (300 mg; N = 140) once daily. The mean age was 46 years, 61% were male, 72% were Asian, 25% were white and 2% (8 subjects) were black; 24%, 38%, and 31% had HBV genotype B, C, and D, respectively. 21% were treatment experienced (previous treatment with oral antivirals, including entecavir (N = 41), lamivudine (N = 42), tenofovir disoproxil fumarate (N = 21), or other (N = 18)). At baseline, mean plasma HBV DNA was 5.8 log
10 IU/mL, mean serum ALT was 94 U/L, and 9% of patients had a story of cirrhosis.
In Study 110, HBeAg-positive treatment-naïve and treatment-experienced patients with compensated liver function were randomized in a 2:1 ratio to receive tenofovir alafenamide tablets (25 mg; N = 581) once daily or tenofovir disoproxil fumarate (300 mg; N = 292) once daily. The mean age was 38 years, 64% were male, 82% were Asian, 17% were White and <1% (5 subjects) were Black. 17%, 52%, and 23% had HBV genotype B, C, and D, respectively. 26% were treatment experienced (previous treatment with oral antivirals, including adefovir (N = 42), entecavir (N = 117), lamivudine (N = 84), telbivudine (N = 25), tenofovir disoproxil fumarate (N = 70), or other (n = 17)). At baseline, mean plasma HBV DNA was 7.6 log
10 IU/mL, mean serum ALT was 120 U/L, and 7% of patients had a history of cirrhosis.
The primary efficacy endpoint in both trials was the proportion of patients with plasma HBV DNA levels below 29 IU/mL Tenofovir alafenamide tablets met the non-inferiority criteria in achieving HBV DNA less than 29 IU/mL when compared to tenofovir disoproxil fumarate.
Treatment outcomes of Study 108 and Study 110 through Week 48 are presented in Table 1 and Table 2. Additional outcomes through Week 72 are presented in Table 3. (See Table 1 and Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Experience beyond 48 weeks in Study 108 and Study 110: At week 72, viral suppression as well as biochemical and serological responses were maintained with continued tenofovir alafenamide treatment (see Table 3). Serological data were not collected at the Week 72 timepoint. (See Table 3.)
Click on icon to see table/diagram/image
Changes in measures of bone mineral density: In both studies tenofovir alafenamide was associated with smaller percentage decreases in bone mineral density (BMD; as measured by hip and lumbar spine dual energy X ray absorptiometry [DXA] analysis) compared to tenofovir disoproxil fumarate after 72 weeks of treatment.
Changes in measures of renal function: In both studies tenofovir alafenamide was associated with smaller changes in renal safety parameters (smaller reductions in estimated CrCl by Cockcroft-Gault and smaller percentage increases in urine protein to creatinine ratio and urine albumin to creatinine ratio) compared to tenofovir disoproxil fumarate after 72 weeks of treatment (see also Precautions).
Pharmacokinetics: Absorption: Following oral administration of Tenofovir Alafenamide tablets under fasted conditions in adult patients with chronic hepatitis B, peak plasma concentrations of tenofovir alafenamide were observed approximately 0.48 hours post-dose. Based on Phase 3 population pharmacokinetic analysis in subjects with CHB, mean steady state AUC
0-24 for tenofovir alafenamide (N = 698) and tenofovir (N = 856) were 0.22 μg•hr/mL and 0.32 μg•hr/mL, respectively. Steady state Cmax for tenofovir alafenamide and tenofovir were 0.18 and 0.02 μg•hr/mL, respectively. Relative to fasting conditions, the administration of a single dose of Tenofovir Alafenamide tablets with a high fat meal resulted in a 65% increase in tenofovir alafenamide exposure.
Distribution: The binding of tenofovir alafenamide to human plasma proteins in samples collected during clinical trials was approximately 80%. The binding of tenofovir to human plasma proteins is less than 0.7% and is independent of concentration over the range of 0.01-25 μg/mL.
Biotransformation: Metabolism is a major elimination pathway for tenofovir alafenamide in humans, accounting for >80% of an oral dose. In vitro studies have shown that tenofovir alafenamide is metabolized to tenofovir (major metabolite) by carboxylesterase-1 in hepatocytes; and by cathepsin A in peripheral blood mononuclear cells (PBMCs) and macrophages. In vivo, tenofovir alafenamide is hydrolysed within cells to form tenofovir (major metabolite), which is phosphorylated to the active metabolite, tenofovir diphosphate.
In vitro, tenofovir alafenamide is not metabolized by CYP1A2, CYP2C8, CYP2C9, CYP2C19, or CYP2D6. Tenofovir alafenamide is minimally metabolized by CYP3A4.
Elimination: Renal excretion of intact tenofovir alafenamide is a minor pathway with <1% of the dose eliminated in urine. Tenofovir alafenamide is mainly eliminated following metabolism to tenofovir. Tenofovir alafenamide and tenofovir have a median plasma half-life of 0.51 and 32.37 hours, respectively. Tenofovir is renally eliminated from the body by the kidneys by both glomerular filtration and active tubular secretion.
Linearity/non-linearity: Tenofovir alafenamide exposures are dose proportional over the dose range of 8 to 125 mg.
Pharmacokinetics in special populations: Age, gender and ethnicity: No clinically relevant differences in pharmacokinetics according to age or ethnicity have been identified. Differences in pharmacokinetics according to gender were not considered to be clinically relevant.
Hepatic impairment: In patients with severe hepatic impairment, total plasma concentrations of tenofovir alafenamide and tenofovir are lower than those seen in subjects with normal hepatic function. When corrected for protein binding, unbound (free) plasma concentrations of tenofovir alafenamide in severe hepatic impairment and normal hepatic function are similar.
Renal impairment: No clinically relevant differences in tenofovir alafenamide or tenofovir pharmacokinetics were observed between healthy subjects and patients with severe renal impairment (estimated CrCl >15 but <30 mL/min) in studies of tenofovir alafenamide.
Paediatric population: The pharmacokinetics of tenofovir alafenamide and tenofovir were evaluated in HIV-1-infected, treatment-naïve adolescents who received tenofovir alafenamide (10 mg) given with elvitegravir, cobicistat and emtricitabine as a fixed dose combination tablet (E/C/F/TAF; Genvoya). No clinically relevant differences in tenofovir alafenamide or tenofovir pharmacokinetics were observed between adolescent and adult HIV-1-infected subjects.
Toxicology: Preclinical safety data: Nonclinical studies in rats and dogs revealed bone and kidney as the primary target organs of toxicity. Bone toxicity was observed as reduced BMD in rats and dogs at tenofovir exposures at least four times greater than those expected after administration of tenofovir alafenamide. A minimal infiltration of histiocytes was present in the eye in dogs at tenofovir alafenamide and tenofovir exposures of approximately 4 and 17 times greater, respectively, than those expected after administration of tenofovir alafenamide.
Tenofovir alafenamide was not mutagenic or clastogenic in conventional genotoxic assays. Because there is a lower tenofovir exposure in rats and mice after tenofovir alafenamide administration compared to tenofovir disoproxil fumarate, carcinogenicity studies and a rat peri-postnatal study were conducted only with tenofovir disoproxil fumarate. No special hazard for humans was revealed in conventional studies of carcinogenic potential with tenofovir disoproxil (as fumarate) and toxicity to reproduction and development with tenofovir disoproxil (as fumarate) or tenofovir alafenamide. Reproductive toxicity studies in rats and rabbits showed no effects on mating, fertility, pregnancy or foetal parameters. However, tenofovir disoproxil fumarate reduced the viability index and weight of pups in a peri-postnatal toxicity study at maternally toxic doses. A long-term oral carcinogenicity study in mice showed a low incidence of duodenal tumours, considered likely related to high local concentrations in the gastrointestinal tract at the high dose of 600 mg/kg/day. The mechanism of tumour formation in mice and potential relevance for humans is uncertain.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image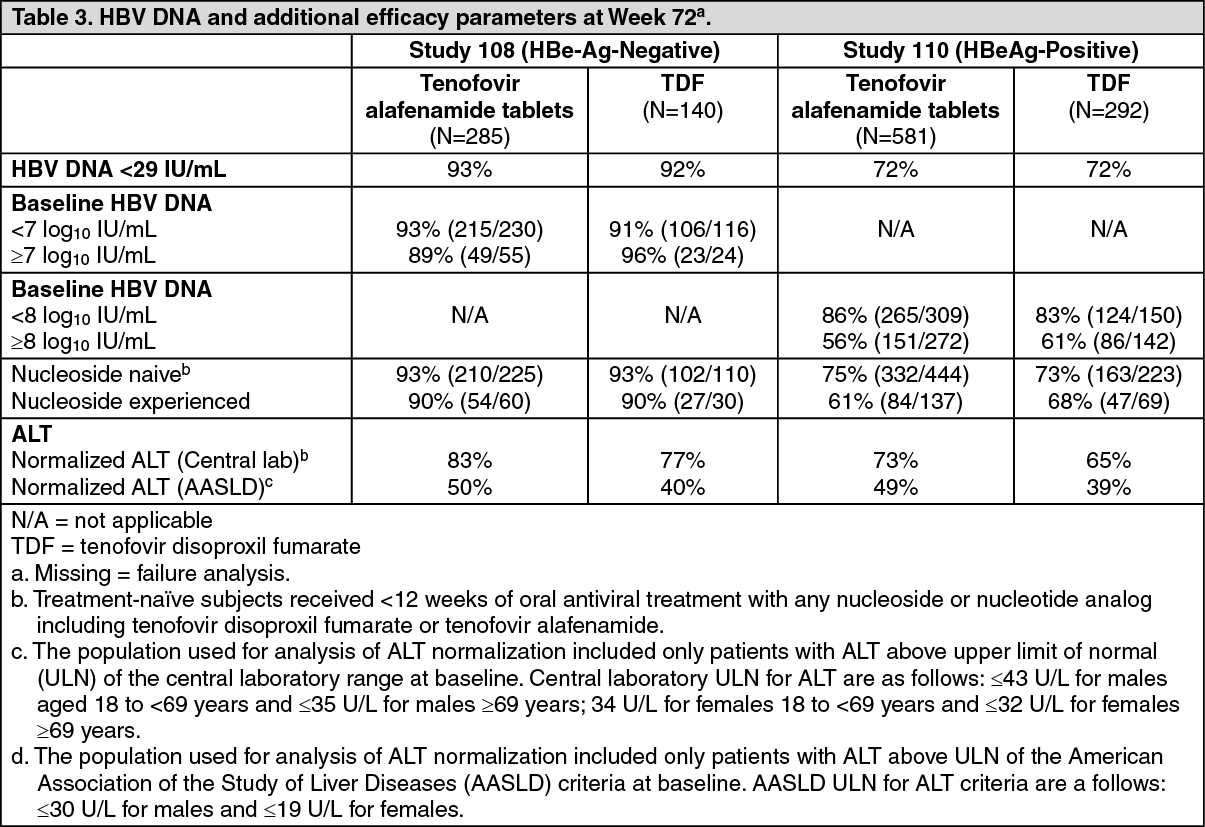 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
