


 Sign Out
Sign Out


Pradaxa treatment does not require anticoagulant monitoring. The INR test is unreliable in patients on Pradaxa and false positive INR elevations have been reported. Therefore, INR tests should not be performed.
Tests of anticoagulant activity eg, thrombin time (TT), ecarin clotting time (ECT) and activated partial thromboplastin time (aPTT) are available to detect excessive dabigatran activity.
Dabigatran-related anticoagulation can be assessed by ECT or TT. If ECT or TT is not available, the aPTT test provides an approximation of the anticoagulant activity of Pradaxa.
Prevention of Stroke, Systemic Embolism and Reduction of Vascular Mortality in Patients with Atrial Fibrillation: In atrial fibrillation patients in RE-LY treated with 150 mg twice daily, an aPTT of >2- to 3-fold of normal range at trough was associated with an increased risk of bleeding.
Pharmacokinetic studies demonstrated an increase in drug exposure in patients with reduced renal function including age-related decline of renal function. Pradaxa is contraindicated in cases of severe renal impairment (CrCl <30 mL/min).
Patients who develop acute renal failure should discontinue Pradaxa.
Factors [eg, decreased renal function (CrCl 30-50 mL/min), patients ≥75 years or strong P-gp inhibitor co-medications are associated with increased dabigatran plasma levels. The presence of one or more than one of these factors may increase the risk of bleeding (see Dosage & Administration).
The concomitant use of Pradaxa with the following treatments has not been studied and may increase the risk of bleeding: Unfractionated heparins (except at doses necessary to maintain patency of the central venous or arterial catheter) and heparin derivatives, low molecular weight heparins (LMWH), fondaparinux, desirudin, thrombolytic agents, glycoprotein IIb/IIIa (GPIIb/IIIa) receptor antagonists, ticlopidine, dextran, sulfinpyrazone, rivaroxaban, prasugrel, VKA and the P-gp inhibitors itraconazole, tacrolimus, cyclosporine, ritonavir, tipranavir, nelfinavir and saquinavir.
The concomitant use of dronedarone increases exposure of dabigatran and is not recommended (see Special Populations under Pharmacokinetics under Actions).
The concomitant use of ticagrelor increases the exposure to dabigatran and may show pharmacodynamic interaction, which may result in an increased risk of bleeding.
Bleeding risk may be increased in patients concomitantly treated with selective serotonin reuptake inhibitors (SSRIs) or selective serotonin norepinephrine reuptake inhibitors (SNRIs).
Use of Fibrinolytic Agents for the Treatment of Acute Ischemic Stroke: The use of fibrinolytic agents for the treatment of acute ischemic stroke may be considered if the patient presents with TT, ECT or aPTT not exceeding the ULN according to the local reference range.
In situations where there is an increased haemorrhagic risk (eg, recent biopsy or major trauma, bacterial endocarditis), close observation (ie, looking for signs of bleeding or anaemia) is generally required.
Prevention of VTE Events in Patients Who Have Undergone Major Orthopaedic Surgery: Nonsteroidal anti-inflammatory drugs (NSAIDs) given for short-term perioperative analgesia have been shown not to be associated with increased bleeding risk when given in conjunction with Pradaxa. There is limited evidence regarding the use of regular NSAID medication with t½ of <12 hrs during treatment with Pradaxa and this has not suggested additional bleeding risk.
Prevention of Stroke, Systemic Embolism and Reduction of Vascular Mortality in Patients with Atrial Fibrillation: Co-administration of antiplatelet (including aspirin and clopidogrel) and NSAID therapies increase the risk of bleeding. Specifically, with concomitant intake of antiplatelets or strong P-gp inhibitors in patients ≥75 years, the risk of major bleeding including gastrointestinal bleeding increases. If bleeding is clinically suspected, appropriate measures (eg, testing for occult blood in stool or testing for a drop in hemoglobin) is suggested.
Interaction with P-gp Inducers: The concomitant use of Pradaxa with the strong P-gp inducer rifampicin reduces dabigatran plasma concentrations. Other P-gp inducers eg, St. John's Wort or carbamazepine are also expected to reduce dabigatran plasma concentrations and should be co-administered with caution (see Special Populations under Pharmacokinetics under Actions and Interactions).
Surgery and Interventions: Patients on Pradaxa who undergo surgery or invasive procedures are at increased risk for bleeding. Therefore, surgical interventions may require the temporary discontinuation of Pradaxa (see also Pharmacokinetics under Pharmacology under Actions).
Preoperative Phase: Due to an increased risk of bleeding, Pradaxa may be stopped temporarily in advance of invasive or surgical procedures. If possible, Pradaxa should be discontinued at least 24 hrs before invasive or surgical procedures. In patients at higher risk of bleeding or in major surgery where complete hemostasis may be required, consider stopping Pradaxa 2-4 days before surgery.
Clearance of dabigatran in patients with renal insufficiency may take longer. This should be considered in advance of any procedures (see Table 11 and Pharmacology: Pharmacokinetics under Actions).
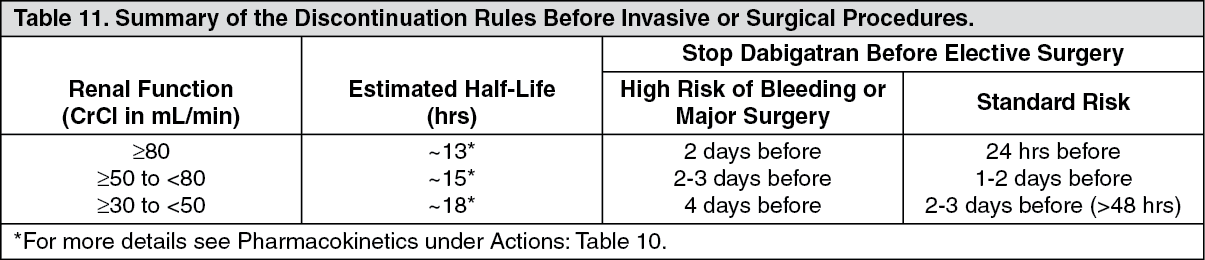 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePradaxa is contraindicated in patients with severe renal dysfunction (CrCl <30 mL/min), but should this occur, Pradaxa should be stopped at least 5 days before major surgery.
If an acute intervention is required, Pradaxa should be temporarily discontinued. A surgery/intervention should be delayed if possible until at least 12 hrs after the last dose. If surgery cannot be delayed, there may be an increase in the risk of bleeding. This risk of bleeding should be weighed together with the urgency of intervention. (For cardioversion, see Dosage & Administration).
Spinal Anesthesia/Epidural Anesthesia/Lumbar Puncture: Procedures (eg, spinal anesthesia) may require complete hemostatic function.
The risk of spinal or epidural hematoma may be increased in cases of traumatic or repeated puncture and by the prolonged use of epidural catheters. After removal of a catheter, an interval of at least 1 hr should elapse before the administration of the 1st dose of Pradaxa. These patients require frequent observation for neurological signs and symptoms of spinal or epidural hematoma.
Postprocedural Period: Resume treatment after complete haemostasis is achieved.
Excipients: Pradaxa contains the excipient sunset yellow (E110) which may cause allergic reactions.
Effects on the Ability to Drive or Operate Machinery: No studies on the effects on the ability to drive and use machines have been performed.
Impairment of Fertility: No clinical data are available. Nonclinical reproductive studies did not show any adverse effects on fertility or postnatal development of the neonate.
Use in Pregnancy: No clinical data on exposed pregnancies are available. The potential risk for humans is unknown.
Women of childbearing potential should avoid pregnancy during treatment with Pradaxa and when pregnant, women should not be treated with Pradaxa unless the expected benefit is greater than the risk.
Use in Lactation: No clinical data are available. As a precaution, breastfeeding should be stopped.
Use in Children: Prevention of VTE Events in Patients Who Have Undergone Major Orthopaedic Surgery and Prevention of Stroke, Systemic Embolism and Reduction of Vascular Mortality in Patients with Atrial Fibrillation: Pradaxa has not been investigated in patients <18 years. Treatment of children with Pradaxa is not recommended.
Treatment and Prevention of Acute or Recurrent DVT and/or PE and Prevention of Related Death: Pradaxa is under investigation in patients <18 years. The safety and efficacy in children has not yet been established. Treatment of children with Pradaxa is therefore not recommended