Pharmacology: Mechanism of Action: Ibrutinib is a small-molecule inhibitor of BTK. Ibrutinib forms a covalent bond with a cysteine residue in the BTK active site, leading to inhibition of BTK enzymatic activity. BTK is a signaling molecule of the B-cell antigen receptor (BCR) and cytokine receptor pathways. BTK's role in signaling through the B-cell surface receptors results in activation of pathways necessary for B-cell trafficking, chemotaxis, and adhesion. Nonclinical studies show that ibrutinib inhibits malignant B-cell proliferation and survival
in vivo as well as cell migration and substrate adhesion
in vitro.
Pharmacodynamics: In patients with recurrent B-cell lymphoma > 90% occupancy of the BTK active site in peripheral blood mononuclear cells was observed up to 24 hours after ibrutinib doses of ≥ 2.5 mg/kg/day (≥ 175 mg/day for average weight of 70 kg).
In vitro Platelet Aggregation: Ibrutinib demonstrated inhibition of collagen-induced platelet aggregation, with IC50 values at 4.6 μM (2026 ng/mL), 0.8 μM (352 ng/mL), and 3 μM (1321 ng/mL) in blood samples from healthy donors, donors taking warfarin, and donors with severe renal dysfunction, respectively. Ibrutinib did not show meaningful inhibition of platelet aggregation for ADP, arachidonic acid, ristocetin, and TRAP-6.
Cardiac Electrophysiology: At a single dose 3 times the maximum recommended dose (1680 mg), IMBRUVICA did not prolong the QT interval to any clinically relevant extent.
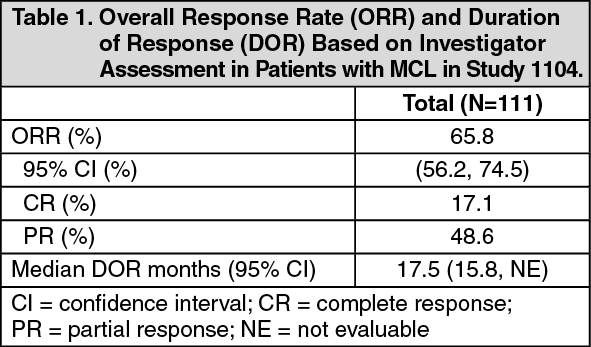
Clinical Studies: Mantle Cell Lymphoma: The safety and efficacy of IMBRUVICA in patients with MCL who have received at least one prior therapy were evaluated in Study1104 (NCT01236391), an open-label, multi-center, single-arm trial of 111 previously treated patients. IMBRUVICA was administered orally at 560 mg once daily until disease progression or unacceptable toxicity. Tumor response was assessed according to the revised International Working Group (IWG) for non-Hodgkin's lymphoma (NHL) criteria. The primary endpoint in this study was investigator-assessed overall response rate (ORR).
The median age was 68 years (range, 40 to 84 years), 77% were male, and 92% were White. At baseline, 89% of patients had a baseline ECOG performance status of 0 or 1. The median time since diagnosis was 42 months, and median number of prior treatments was 3 (range, 1 to 5 treatments), including 11% with prior stem cell transplantation. At baseline, 39% of subjects had at least one tumor ≥ 5 cm, 49% had bone marrow involvement, and 54% had extranodal involvement at screening.
Responses to IMBRUVICA are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
An Independent Review Committee (IRC) performed independent reading and interpretation of imaging scans. The IRC review demonstrated an ORR of 69%.
The median time to response was 1.9 months.
Lymphocytosis: Upon initiation of IMBRUVICA, a temporary increase in lymphocyte counts (i.e., ≥ 50% increase from baseline and above absolute lymphocyte count of 5,000/mcL) occurred in 33% of patients in the MCL study. The onset of isolated lymphocytosis occurs during the first few weeks of IMBRUVICA therapy and resolves by a median of 8 weeks.
Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma: The safety and efficacy of IMBRUVICA in patients with CLL/SLL were demonstrated in one uncontrolled trial and five randomized, controlled trials.
Study 1102: Study 1102 (NCT01105247), an open-label, multi-center trial, was conducted in 48 previously treated CLL patients. IMBRUVICA was administered orally at 420 mg once daily until disease progression or unacceptable toxicity. The ORR and DOR were assessed using a modified version of the International Workshop on CLL Criteria by an Independent Review Committee.
The median age was 67 years (range, 37 to 82 years), 71% were male, and 94% were White. All patients had a baseline ECOG performance status of 0 or 1. The median time since diagnosis was 80 months and the median number of prior treatments was 4 (range, 1 to 12 treatments). At baseline, 46% of subjects had at least one tumor ≥ 5 cm.
The ORR was 58.3% (95% CI: 43.2%, 72.4%), all partial responses. None of the patients achieved a complete response. The DOR ranged from 5.6 to 24.2+ months. The median DOR was not reached.
RESONATE: The RESONATE study, a randomized, multicenter, open-label, phase 3 study of IMBRUVICA versus ofatumumab (NCT01578707), was conducted in patients with previously treated CLL or SLL. Patients (n=391) were randomized 1:1 to receive either IMBRUVICA 420 mg daily until disease progression, or unacceptable toxicity or ofatumumab at an initial dose of 300 mg, followed one week later by a dose of 2000 mg weekly for 7 doses and then every 4 weeks for 4 additional doses. Fifty seven patients randomized to ofatumumab crossed over following progression to receive IMBRUVICA.
The median age was 67 years (range, 30 to 88 years), 68% were male, and 90% were White. All patients had a baseline ECOG performance status of 0 or 1. The trial enrolled 373 patients with CLL and 18 patients with SLL. The median time since diagnosis was 91 months and the median number of prior treatments was 2 (range, 1 to 13 treatments). At baseline, 58% of patients had at least one tumor ≥ 5 cm. Thirty-two percent of patients had 17p deletion.
Efficacy results for RESONATE are shown in Table 2 and the Kaplan-Meier curves for PFS, assessed by an IRC according to IWCLL criteria, and OS are shown in Figures 1 and 2, respectively. (See Table 2 and Figures 1 and 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
63-Month Follow-Up: With an overall follow-up of 63 months, the median investigator-assessed PFS per IWCLL criteria was 44.1 months [95% CI (38.5, 56.9)] in the IMBRUVICA arm and 8.1 months [95% CI (7.8, 8.3)] in the ofatumumab arm, respectively. Overall response rate as assessed by investigators was 87.2% in the IMBRUVICA arm versus 22.4% in the ofatumumab arm.
CLL/SLL with 17p deletion (del 17p CLL/SLL) in RESONATE: RESONATE included 127 patients with del 17p CLL/SLL. The median age was 67 years (range, 30 to 84 years), 62% were male, and 88% were White. All patients had a baseline ECOG performance status of 0 or 1. PFS and ORR were assessed by an IRC. Efficacy results for del 17p CLL/SLL are shown in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
63-Month Follow-Up: With an overall follow-up of 63 months, the median investigator-assessed PFS in patients with del 17p per IWCLL criteria was 40.6 months [95% CI (25.4, 44.6)] in the IMBRUVICA arm and 6.2 months [95% CI (4.6, 8.1)] in the ofatumumab arm, respectively. Overall response rate as assessed by investigators in patients with del 17p was 88.9% in the IMBRUVICA arm versus 18.8% in the ofatumumab arm.
RESONATE-2: The RESONATE-2 study, a randomized, multicenter, open-label, phase 3 study of IMBRUVICA versus chlorambucil (NCT01722487), was conducted in patients with treatment naïve CLL or SLL who were 65 years of age or older. Patients (n = 269) were randomized 1:1 to receive either IMBRUVICA 420 mg daily until disease progression or unacceptable toxicity, or chlorambucil at a starting dose of 0.5 mg/kg on Days 1 and 15 of each 28-day cycle for a maximum of 12 cycles, with an allowance for intrapatient dose increases up to 0.8 mg/kg based on tolerability.
The median age was 73 years (range, 65 to 90 years), 63% were male, and 91% were White. Ninety one percent of patients had a baseline ECOG performance status of 0 or 1 and 9% had an ECOG performance status of 2. The trial enrolled 249 patients with CLL and 20 patients with SLL. At baseline, 20% of patients had 11q deletion. The most common reasons for initiating CLL therapy include: progressive marrow failure demonstrated by anemia and/or thrombocytopenia (38%), progressive or symptomatic lymphadenopathy (37%), progressive or symptomatic splenomegaly (30%), fatigue (27%) and night sweats (25%).
With a median follow-up of 28.1 months, there were 32 observed death events [11 (8.1%) and 21 (15.8%) in IMBRUVICA and chlorambucil treatment arms, respectively]. With 41% of patients switching from chlorambucil to IMBRUVICA, the overall survival analysis in the ITT patient population resulted in a statistically significant HR of 0.44 [95% CI (0.21, 0.92)] and 2-year survival rate estimates of 94.7% [95% CI (89.1, 97.4)] and 84.3% [95% CI (76.7, 89.6)] in the IMBRUVICA and chlorambucil arms, respectively.
Efficacy results for RESONATE-2 are shown in Table 4 and the Kaplan-Meier curve for PFS, assessed by an IRC according to IWCLL criteria is shown in Figure 3. (See Table 4 and Figure 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
55-Month Follow-Up: With an overall follow-up of 55 months, the median PFS was not reached in the IMBRUVICA arm.
HELIOS: The HELIOS study, a randomized, double-blind, placebo-controlled phase 3 study of IMBRUVICA in combination with bendamustine and rituximab (BR) (NCT01611090), was conducted in patients with previously treated CLL or SLL. Patients (n = 578) were randomized 1:1 to receive either IMBRUVICA 420 mg daily or placebo in combination with BR until disease progression, or unacceptable toxicity. All patients received BR for a maximum of six 28-day cycles. Bendamustine was dosed at 70 mg/m
2 infused IV over 30 minutes on Cycle 1, Days 2 and 3, and on Cycles 2-6, Days 1 and 2 for up to 6 cycles, and all patients had a CLCr ≥ 40 mL/min at baseline. Rituximab was administered at a dose of 375 mg/m
2 in the first cycle, Day 1, and 500 mg/m
2 Cycles 2 through 6, Day 1.
The median age was 64 years (range, 31 to 86 years), 66% were male, and 91% were White. All patients had a baseline ECOG performance status of 0 or 1. The median time since diagnosis was 5.9 years and the median number of prior treatments was 2 (range, 1 to 11 treatments). At baseline, 56% of patients had at least one tumor ≥ 5 cm and 26% presented with del11q.
Efficacy results for HELIOS are shown in Table 5 and the Kaplan-Meier curves for PFS are shown in Figure 4. (See Table 5 and Figure 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
iLLUMINATE: The iLLUMINATE study, a randomized, multi-center, phase 3 study of IMBRUVICA in combination with obinutuzumab versus chlorambucil in combination with obinutuzumab (NCT02264574), was conducted in patients with treatment naïve CLL or SLL. Patients were 65 years of age or older or < 65 years of age with coexisting medical conditions, reduced renal function as measured by creatinine clearance < 70 mL/min, or presence of del 17p/TP53 mutation. Patients (n = 229) were randomized 1:1 to receive either IMBRUVICA 420 mg daily until disease progression or unacceptable toxicity or chlorambucil at a dose of 0.5 mg/kg on Days 1 and 15 of each 28-day cycle for 6 cycles. In both arms, patients received 1,000 mg of obinutuzumab on Days 1, 8, and 15 of the first cycle, followed by treatment on the first day of 5 subsequent cycles (total of 6 cycles, 28 days each). The first dose of obinutuzumab was divided between Day 1 (100 mg) and Day 2 (900 mg).
The median age was 71 years (range, 40 to 87 years), 64% were male, and 96% were White. All patients had a baseline ECOG performance status of 0 (48%) or 1-2 (52%). The trial enrolled 214 patients with CLL and 15 patients with SLL. At baseline, 65% of patients presented with CLL/SLL with high risk factors (del 17p/TP53 mutation [18%], del 11q [15%], or unmutated immunoglobulin heavy-chain variable region (unmutated IGHV) [54%]). The most common reasons for initiating CLL therapy included: lymphadenopathy (38%), night sweats (34%), progressive marrow failure (31%), fatigue (29%), splenomegaly (25%), and progressive lymphocytosis (21%).
With a median follow-up time on study of 31 months, efficacy results for iLLUMINATE assessed by an IRC according to IWCLL criteria are shown in Table 6, and the Kaplan-Meier curve for PFS is shown in Figure 5. (See Table 6 and Figure 5.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the high risk CLL/SLL population (del 17p/TP53 mutation, del 11q, or unmutated IGHV), the PFS HR was 0.15% [95% Cl (0.09, 0.27)].
E1912: The E1912 study, a randomized, multi-center, phase 3 study of IMBRUVICA in combination with rituximab versus standard fludarabine, cyclophosphamide, and rituximab (FCR) chemoimmunotherapy (NCT02048813), was conducted in adult patients who were 70 years or younger with previously untreated CLL or SLL requiring systemic therapy. All patients had a CLcr > 40 mL/min at baseline. Patients with 17p deletion were excluded. Patients (n =529) were randomized 2:1 to receive either IMBRUVICA plus rituximab or FCR. IMBRUVICA was administered at 420 mg daily until disease progression or unacceptable toxicity. Fludarabine was administered at a dose of 25 mg/m
2, and cyclophosphamide was administered at a dose of 250 mg/m
2, both on Days 1, 2, and 3 of Cycles 1-6. Rituximab was initiated in Cycle 2 for the IMBRUVICA plus rituximab arm and in Cycle 1 for the FCR arm and was administered at 50 mg/m
2 on Day 1 of the first cycle, 325 mg/m
2 on Day 2 of the first cycle, and 500 mg/m
2 on Day 1 of 5 subsequent cycles, for a total of 6 cycles. Each cycle was 28 days.
The median age was 58 years (range, 28 to 70 years), 67% were male, 90% were White and 98% had a ECOG performance status of 0-1. At baseline, 43% of patients were Rai stage 3 or 4 and 59% of patients presented with high risk factors (TP53 mutation [6%], del11q [22%], or unmutated IGHV [53%]).
With a median follow-up time on study of 37 months, efficacy results for E1912 are shown in Table 7. The Kaplan-Meier curves for PFS, assessed according to IWCLL criteria is shown in Figure 6. (See Table 7 and Figure 6.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
With a median follow-up time on study of 49 months, median overall survival was not reached with a total of 23 deaths: 11 (3%) in the IMBRUVICA plus rituximab and 12 (7%) in the FCR treatment arms.
Lymphocytosis: Upon initiation of single-agent IMBRUVICA, an increase in lymphocyte counts (i.e., ≥ 50% increase from baseline and above absolute lymphocyte count of 5,000/mcL) occurred in 66% of patients in the CLL studies. The onset of isolated lymphocytosis occurs during the first month of IMBRUVICA therapy and resolves by a median of 14 weeks (range, 0.1 to 104 weeks). When IMBRUVICA was administered in combination, lymphocytosis was 7% with IMBRUVICA + BR versus 6% with placebo + BR and 7% with IMBRUVICA + obinutuzumab versus 1% with chlorambucil + obinutuzumab.
Waldenström's Macroglobulinemia: The safety and efficacy of IMBRUVICA in patients with WM were demonstrated in two single-arm trials and one randomized, controlled trial.
Study 1118 and INNOVATE Monotherapy Arm: Study 1118 (NCT01614821), an open-label, multi-center, single-arm trial was conducted in 63 previously treated patients with WM. IMBRUVICA was administered orally at 420 mg once daily until disease progression or unacceptable toxicity. The responses were assessed by investigators and an IRC using criteria adopted from the International Workshop of Waldenström's Macroglobulinemia.
The median age was 63 years (range, 44 to 86 years), 76% were male, and 95% were White. All patients had a baseline ECOG performance status of 0 or 1. The median time since diagnosis was 74 months, and the median number of prior treatments was 2 (range, 1 to 11 treatments). At baseline, the median serum IgM value was 3.5 g/dL (range, 0.7 to 8.4 g/dL).
Responses, defined as partial response or better, per IRC are shown in Table 8. (See Table 8.)
Click on icon to see table/diagram/image
The median time to response was 1.2 months (range, 0.7-13.4 months).
The INNOVATE monotherapy arm included 31 patients with previously treated WM who failed prior rituximab-containing therapy and received single-agent IMBRUVICA. The median age was 67 years (range, 47 to 90 years). Eighty-one percent of patients had a baseline ECOG performance status of 0 or 1, and 19% had a baseline ECOG performance status of 2. The median number of prior treatments was 4 (range, 1 to 7 treatments). With an overall follow-up of 61 months, the response rate observed in the INNOVATE monotherapy arm per IRC assessment was 77% (0% CR, 29% VGPR, 48% PR). The median duration of response was 33 months (range, 2.4 to 60.2+ months).
INNOVATE: The INNOVATE study, a randomized, double-blind, placebo-controlled, phase 3 study of IMBRUVICA or placebo in combination with rituximab (NCT02165397), was conducted in treatment naïve or previously treated patients with WM. Patients (n = 150) were randomized 1:1 to receive either IMBRUVICA 420 mg daily or placebo in combination with rituximab until disease progression or unacceptable toxicity. Rituximab was administered weekly at a dose of 375 mg/m
2 for 4 consecutive weeks (weeks 1-4) followed by a second course of weekly rituximab for 4 consecutive weeks (weeks 17-20). The major efficacy outcome measure is progression-free survival (PFS) assessed by an IRC with additional efficacy measure of response rate.
The median age was 69 years (range, 36 to 89 years), 66% were male, and 79% were White. Ninety-three percent of patients had a baseline ECOG performance status of 0 or 1, and 7% of patients had a baseline ECOG performance status of 2. Forty-five percent of patients were treatment naïve, and 55% of patients were previously treated. Among previously treated patients, the median number of prior treatments was 2 (range, 1 to 6 treatments). At baseline, the median serum IgM value was 3.2 g/dL (range, 0.6 to 8.3 g/dL), and MYD88 L265P mutations were present in 77% of patients, absent in 13% of patients, and 9% of patients were not evaluable for mutation status.
An exploratory analysis demonstrated a sustained hemoglobin improvement (defined as increase of ≥ 2 g/dL over baseline for at least 8 weeks without blood transfusions or growth factor support) in 65% of patients in the IMBRUVICA + R group and 39% of patients in the placebo + R group.
With an overall follow-up of 63 months, efficacy results as assessed by an IRC at the time of the final analysis for INNOVATE are shown in Table 9, and the Kaplan-Meier curves for PFS are shown in Figure 7. (See Table 9 and Figure 7.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Median overall survival was not reached for either treatment arm. With an overall follow-up of 63 months, 9 (12%) patients on IMBRUVICA + R and 10 (13.3%) patients on placebo + R had died. Forty-seven percent of patients randomized to the placebo + R arm crossed over to receive IMBRUVICA.
Marginal Zone Lymphoma: The safety and efficacy of IMBRUVICA in MZL were evaluated in Study 1121 (NCT01980628), an open-label, multi-center, single-arm trial of patients who received at least one prior therapy. IMBRUVICA was administered orally at 560 mg once daily until disease progression or unacceptable toxicity. The responses were assessed by investigators and an IRC using criteria adopted from the International Working Group criteria for malignant lymphoma.
The efficacy analysis included 63 patients with 3 sub-types of MZL: mucosa-associated lymphoid tissue (MALT; N=32), nodal (N=17), and splenic (N=14). The median age was 66 years (range, 30 to 92 years), 59% were female, and 84% were White. Ninety two percent of patients had a baseline ECOG performance status of 0 or 1 and 8% had ECOG performance status 2. The median time since diagnosis was 3.8 years, and the median number of prior treatments was 2 (range, 1 to 9 treatments).
Responses per IRC are shown in Table 10. (See Table 10.)
Click on icon to see table/diagram/image
The median time to response was 4.5 months (range, 2.3 to 16.4 months). Overall response rates were 46.9%, 41.2%, and 50.0% for the 3 MZL sub-types (MALT, nodal, splenic), respectively.
Chronic Graft versus Host Disease: The safety and efficacy of IMBRUVICA in cGVHD were evaluated in Study 1129 (NCT02195869), an open-label, multi-center, single-arm trial of 42 patients with cGVHD after failure of first line corticosteroid therapy and requiring additional therapy. IMBRUVICA was administered orally at 420 mg once daily. The responses were assessed by investigators using the 2005 National Institute of Health (NIH) Consensus Panel Response Criteria with two modifications to align with the updated 2014 NIH Consensus Panel Response Criteria.
The median age was 56 years (range, 19 to 74 years), 52% were male, and 93% were White. The most common underlying malignancies leading to transplantation were acute lymphocytic leukemia, acute myeloid leukemia, and CLL. The median time since cGVHD diagnosis was 14 months, the median number of prior cGVHD treatments was 2 (range, 1 to 3 treatments), and 60% of patients had a Karnofsky performance score of ≤ 80. The majority of patients (88 %) had at least 2 organs involved at baseline, with the most commonly involved organs being mouth (86%), skin (81%), and gastrointestinal tract (33%). The median daily corticosteroid dose (prednisone or prednisone equivalent) at baseline was 0.3 mg/kg/day, and 52% of patients were receiving ongoing immunosuppressants in addition to systemic corticosteroids at baseline. Prophylaxis for infections were managed per institutional guidelines with 79% of patients receiving combinations of sulfonamides and trimethoprim and 64% receiving triazole derivatives.
Efficacy results are shown in Table 11. (See Table 11.)
Click on icon to see table/diagram/image
The median time to response coinciding with the first scheduled response assessment was 12.3 weeks (range, 4.1 to 42.1 weeks). Responses were seen across all organs involved for cGVHD (skin, mouth, gastrointestinal tract, and liver).
ORR results were supported by exploratory analyses of patient-reported symptom bother which showed at least a 7-point decrease in Lee Symptom Scale overall summary score in 24% (10/42) of patients on at least 2 consecutive visits.
Pharmacokinetics: Ibrutinib exposure increases with doses up to 840 mg (1.5 times the maximum approved recommended dosage) in patients with B-cell malignancies. The mean steady-state AUC (% coefficient of variation) observed in patients at 560 mg with MCL is 865 (69%) ng·h/mL and with MZL is 978 (82%) ng·h/mL, and in patients at 420 mg with CLL/SLL is 708 (71%) ng·h/mL, with WM is 707 (72%) ng·h/mL, and with cGVHD is 1159 (50%) ng·h/mL. Steady-state concentrations of ibrutinib without CYP3A inhibitors were achieved with an accumulation ratio of 1 to 1.6 after 1 week of multiple daily doses of 420 mg or 560 mg.
Absorption: Absolute bioavailability of ibrutinib in fasted condition was 2.9% (90% CI: 2.1, 3.9) in healthy subjects. Ibrutinib is absorbed after oral administration with a median T
max of 1 hour to 2 hours.
Effect of Food: The administration of IMBRUVICA with a high-fat and high-calorie meal (800 calories to 1,000 calories with approximately 50% of total caloric content of the meal from fat) increased ibrutinib C
max by 2- to 4-fold and AUC by approximately 2-fold, compared with administration of ibrutinib after overnight fasting.
In vitro studies suggest that ibrutinib is not a substrate of p-glycoprotein (P-gp) or breast cancer resistance protein (BCRP).
Distribution: Reversible binding of ibrutinib to human plasma protein
in vitro was 97.3% with no concentration dependence in the range of 50 ng/mL to 1000 ng/mL. The volume of distribution (V
d) was 683 L, and the apparent volume of distribution at steady state (V
d,ss/F) was approximately 10,000 L.
Elimination: Intravenous clearance was 62 L/h in fasted conditions and 76 L/h in fed conditions. In line with the high first-pass effect, the apparent oral clearance is 2000 L/h in fasted conditions and 1000 L/h in fed conditions. The half-life of ibrutinib is 4 hours to 6 hours.
Metabolism: Metabolism is the main route of elimination for ibrutinib. It is metabolized to several metabolites primarily by cytochrome P450 (CYP) 3A and to a minor extent by CYP2D6. The active metabolite, PCI-45227, is a dihydrodiol metabolite with inhibitory activity towards BTK approximately 15 times lower than that of ibrutinib. The range of the mean metabolite to parent ratio for PCI-45227 at steady-state is 1 to 2.8.
Excretion: Ibrutinib, mainly in the form of metabolites, is eliminated primarily via feces. After a single oral administration of radiolabeled ibrutinib, 90% of radioactivity was excreted within 168 hours, with 80% excreted in the feces and less than 10% eliminated in urine. Unchanged ibrutinib accounted for 1% of the radiolabeled excreted dose in feces and none in urine, with the remainder of the excreted dose being metabolites.
Specific Populations: Age and Sex: Age and sex have no clinically meaningful effect on ibrutinib pharmacokinetics.
Patients with Renal Impairment: Mild and moderate renal impairment (creatinine clearance [CLcr] > 25 mL/min as estimated by Cockcroft-Gault equation) had no influence on the exposure of ibrutinib. No data is available in patients with severe renal impairment (CLcr < 25 mL/min) or in patients on dialysis.
Patients with Hepatic Impairment: The AUC of ibrutinib increased 2.7-fold in subjects with mild hepatic impairment (Child-Pugh class A), 8.2-fold in subjects with moderate hepatic impairment (Child-Pugh class B) and 9.8 fold in subjects with severe hepatic impairment (Child-Pugh class C) relative to subjects with normal liver function. The C
max of ibrutinib increased 5.2-fold in mild hepatic impairment, 8.8 fold in moderate hepatic impairment and 7-fold in severe hepatic impairment relative to subjects with normal liver function [see Use in Specific Populations: Hepatic Impairment under Dosage & Administration].
Drug Interaction Studies: Clinical Studies and Model-Informed Approaches: Effect of CYP3A Inhibitors on Ibrutinib: The coadministration of multiple doses of ketoconazole (strong CYP3A inhibitor) increased the C
max of ibrutinib by 29-fold and AUC by 24-fold. The coadministration of multiple doses of voriconazole (strong CYP3A inhibitor) increased steady state C
max of ibrutinib by 6.7-fold and AUC by 5.7-fold. Simulations under fed conditions suggest that posaconazole (strong CYP3A inhibitor) may increase the AUC of ibrutinib 3-fold to 10-fold.
The coadministration of multiple doses of erythromycin (moderate CYP3A inhibitor) increased steady state C
max of ibrutinib by 3.4-fold and AUC by 3-fold.
Effect of CYP3A Inducers on Ibrutinib: The coadministration of rifampin (strong CYP3A inducer) decreased the C
max of ibrutinib by more than 13-fold and AUC by more than 10-fold. Simulations suggest that efavirenz (moderate CYP3A inducer) may decrease the AUC of ibrutinib by 3-fold.
In Vitro Studies: Effect of Ibrutinib on CYP Substrates:
In vitro studies suggest that ibrutinib and PCI-45227 are unlikely to inhibit CYP1A2, 2B6, 2C8, 2C9, 2C19, 2D6 or 3A at clinical doses. Both ibrutinib and PCI-45227 are unlikely to induce CYP1A2, CYP2B6 or CYP3A at clinical doses.
Effect of Ibrutinib on Substrates of Transporters:
In vitro studies suggest that ibrutinib may inhibit BCRP and P-gp transport at clinical doses. The coadministration of oral P-gp or BCRP substrates with a narrow therapeutic index (e.g., digoxin, methotrexate) with IMBRUVICA may increase their concentrations.
Toxicology: Preclinical Safety data: Carcinogenesis, Mutagenesis, Impairment of Fertility: Ibrutinib was not carcinogenic in a 6-month rasH2 mouse study at oral doses up to 2000 mg/kg/day resulting in exposures approximately 23 (males) to 37 (females) times higher than the exposure in humans at a dose of 560 mg daily [see Second Primary Malignancies under Precautions].
Ibrutinib was not mutagenic in a bacterial mutagenicity (Ames) assay, was not clastogenic in a chromosome aberration assay in mammalian (CHO) cells, nor was it clastogenic in an
in vivo bone marrow micronucleus assay in mice at doses up to 2000 mg/kg.
Rats were administered oral daily doses of ibrutinib for 4 weeks prior to pairing and during pairing in males and 2 weeks prior to pairing and during pairing in females. Treatment of female rats continued following pregnancy up to gestation day (GD) 7, and treatment of male rats continued until end of study. No effects on fertility or reproductive capacities were observed in male or female rats up to the maximum dose tested, 100 mg/kg/day (Human Equivalent Dose [HED] 16 mg/kg).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image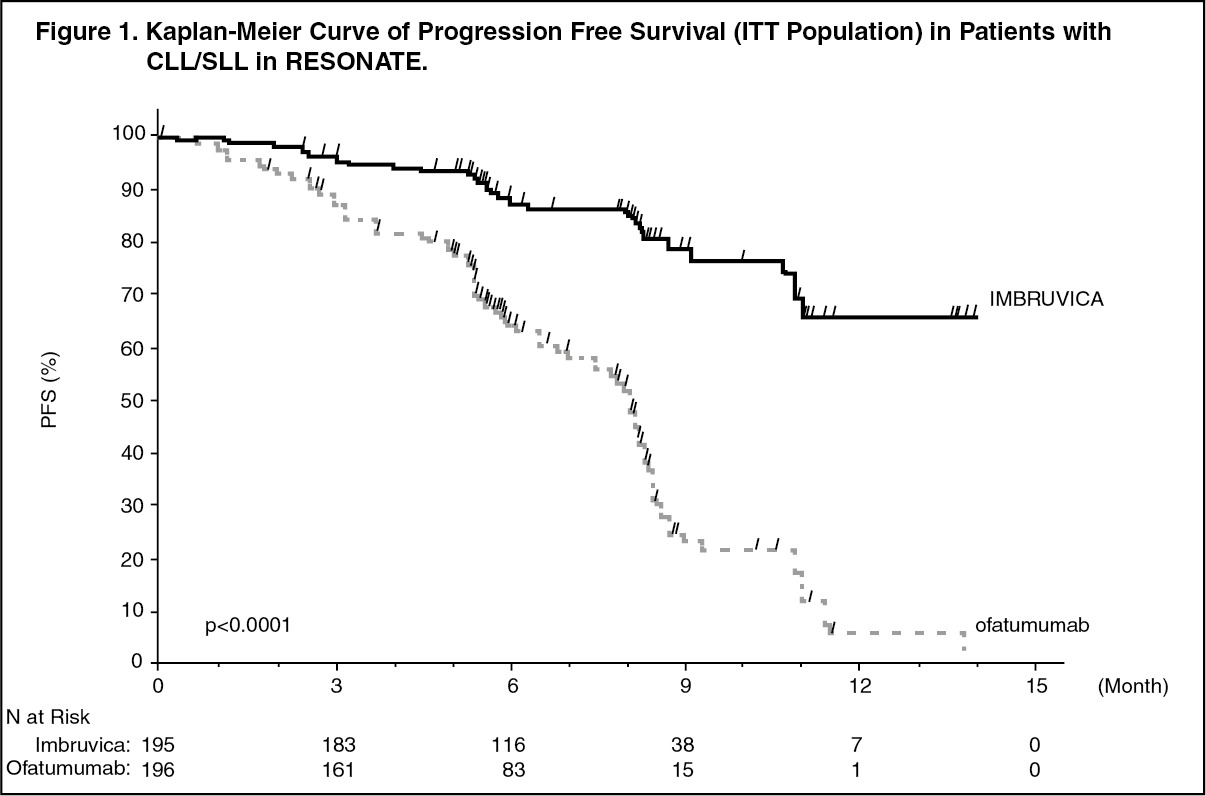 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image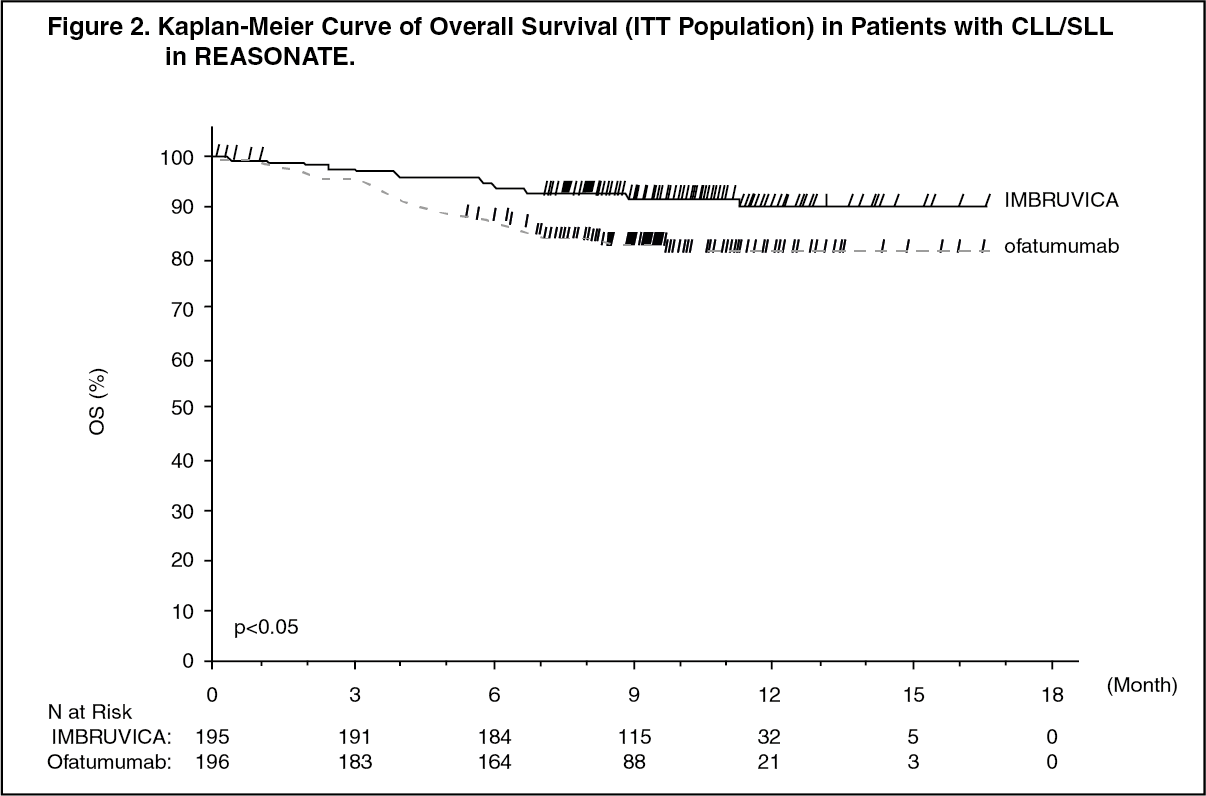 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image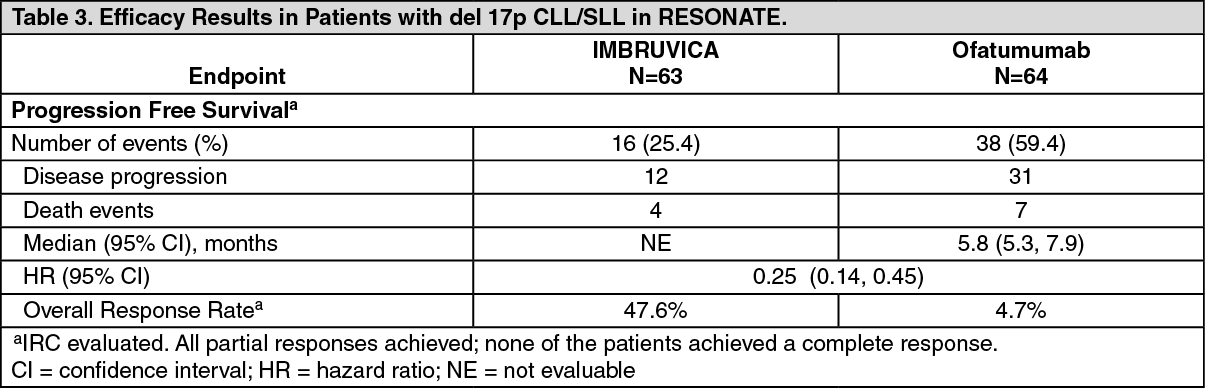 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image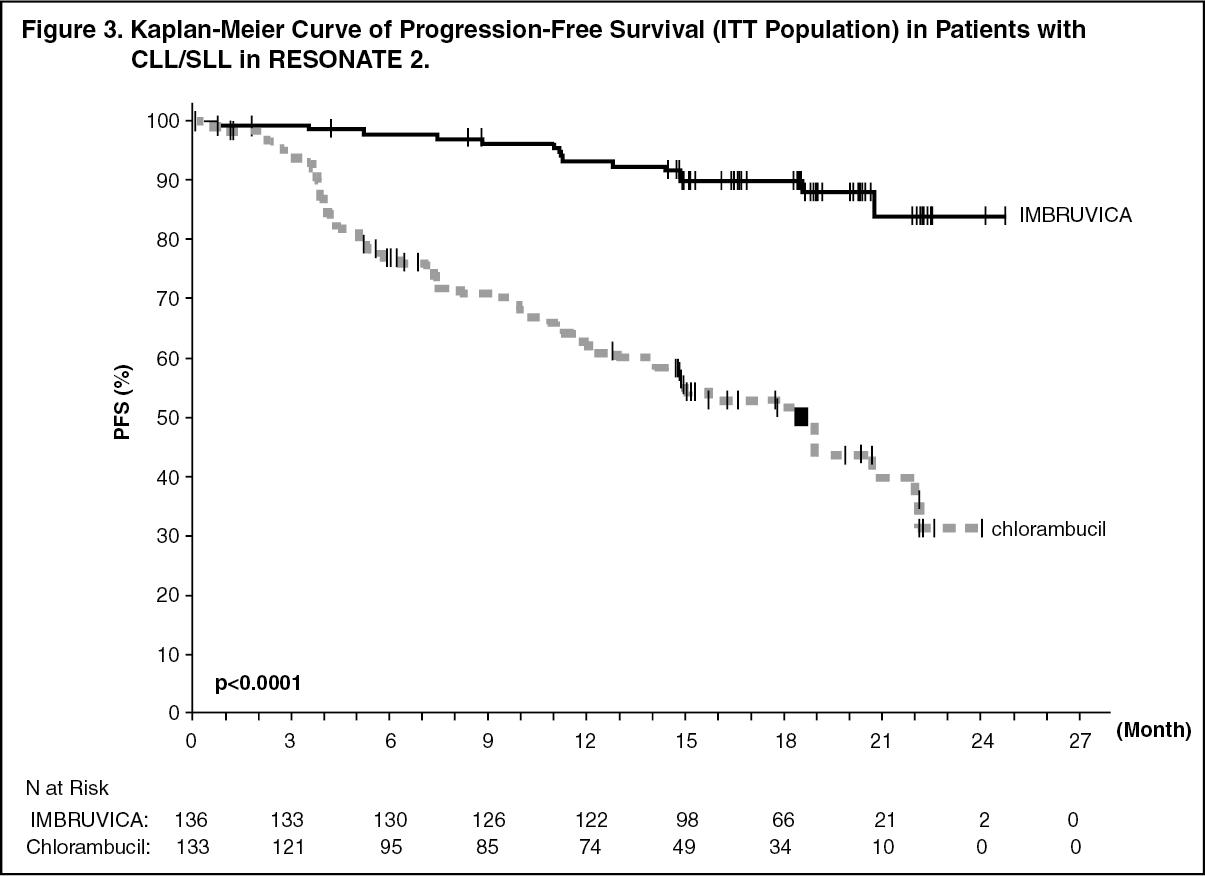 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image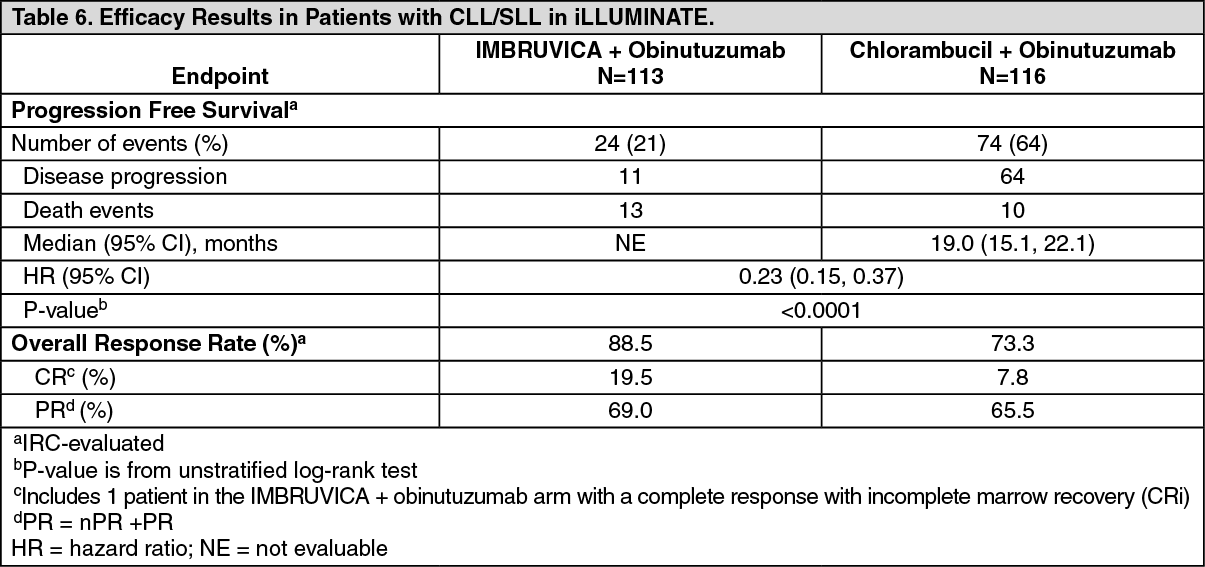 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image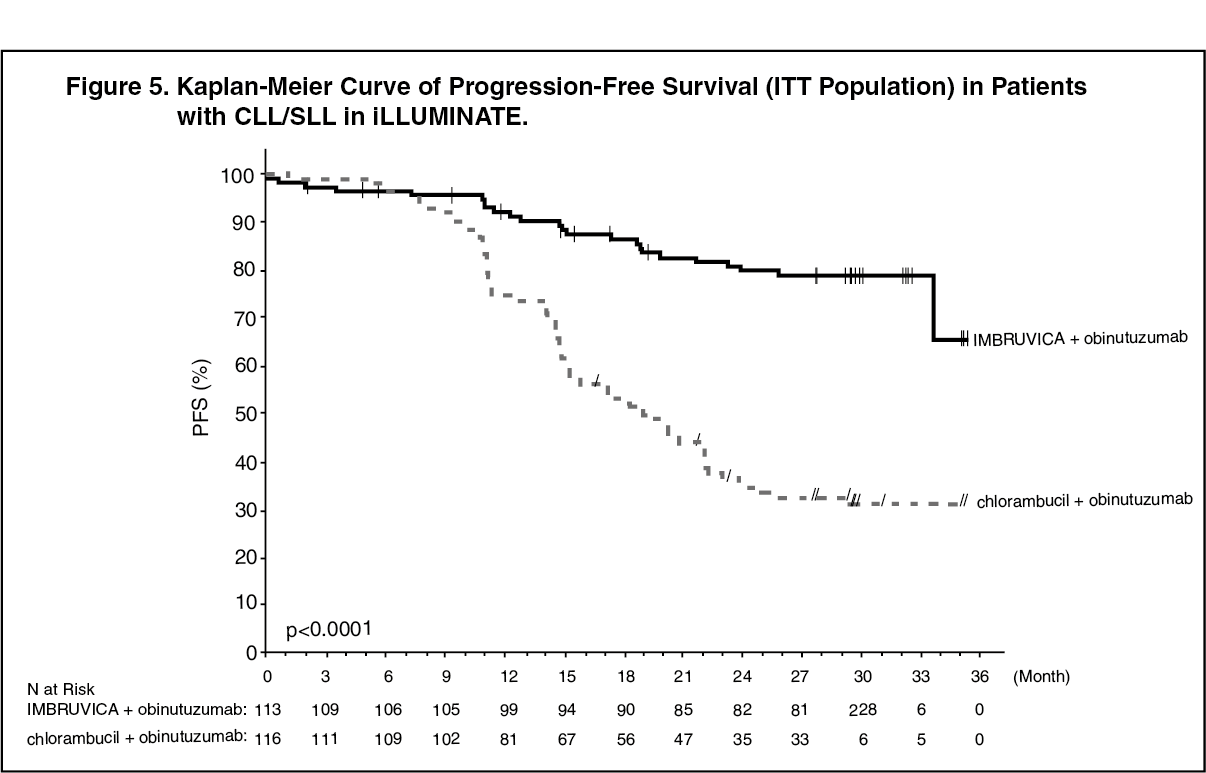 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
