


 Sign Out
Sign Out

The most serious adverse drug reactions were: Infusion related reactions which is more common in CLL patients (see General under Precautions); Tumor Lysis Syndrome, which is more common in patients with a high tumour burden and/or a high circulating lymphocyte count patients and/or renal impairment (see General under Precautions); Thrombocytopenia, which can be fatal in Cycle 1 (see General under Precautions).
The most frequently observed adverse drug reactions across clinical trials in patients receiving GAZYVA were IRR, neutropenia, diarrhea, constipation, and cough.
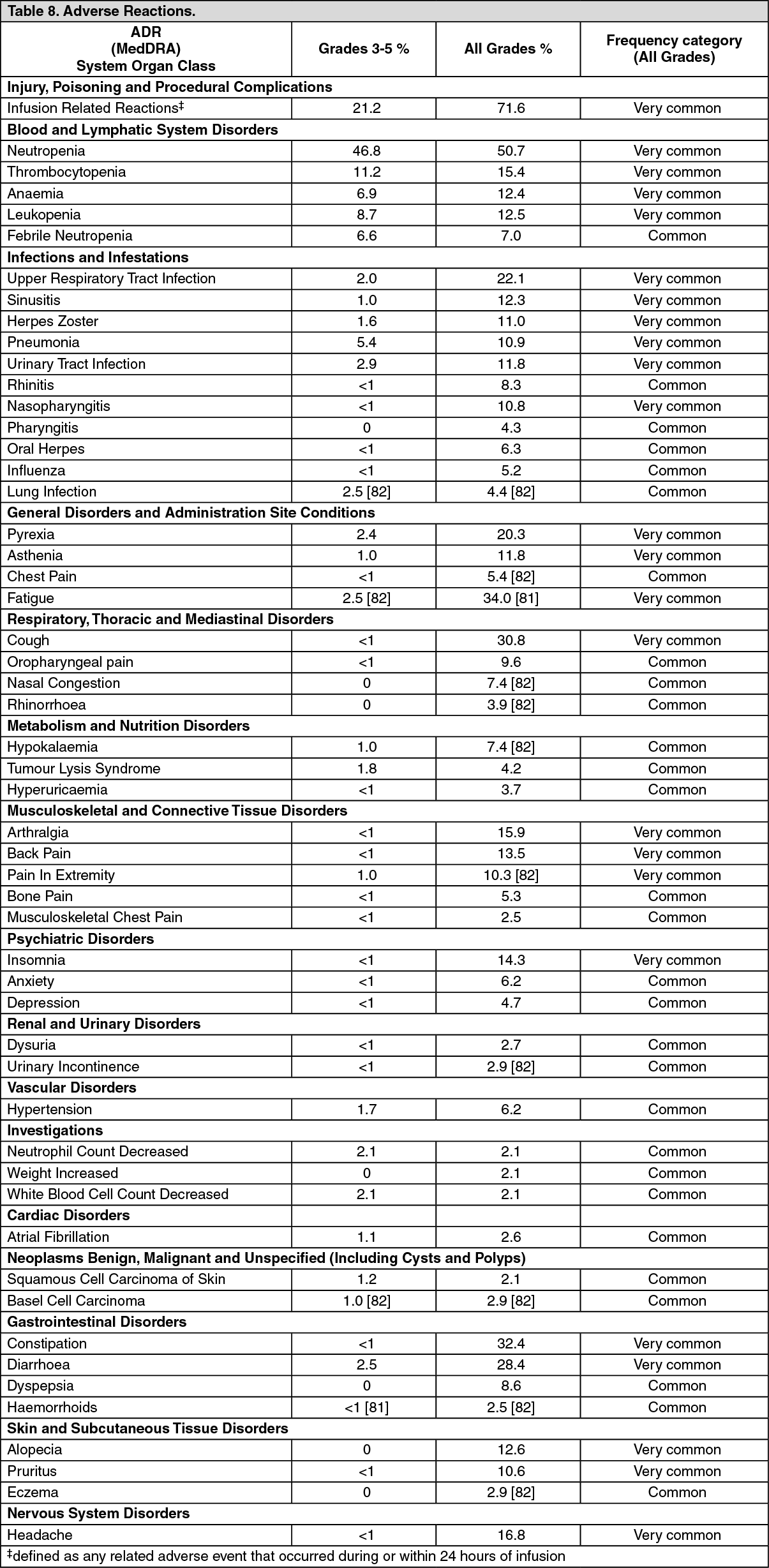
Table 8 lists adverse drug reactions associated with the use of GAZYVA in combination with different chemotherapy regimens in multiple indications. The adverse drug reactions listed in this table fall into the following categories (Very Common (≥10%), Common (≥1% - < 10%) and Uncommon (≥0.1% - < 1%)). Adverse drug reactions are added to the appropriate category in the table as follows according to the highest incidence (difference of ≥2% compared to the relevant comparator arm) seen in any of the major clinical trials. Within each frequency grouping adverse drug reactions are presented in order by system organ class. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFurther information on selected adverse drug reactions: Infusion-related reactions: Most frequently reported (≥5%) symptoms associated with an IRR were nausea, vomiting, diarrhoea, headache, dizziness, fatigue, chills, pyrexia, hypotension, flushing, hypertension, tachycardia, dyspnoea, and chest discomfort. Respiratory symptoms such as, bronchospasm, larynx and throat irritation, wheezing, laryngeal oedema and cardiac symptoms such as atrial fibrillation have also been reported (See Precautions).
Chronic Lymphocytic Leukaemia: The incidence of IRRs was 65% with the infusion of the first 1000 mg of GAZYVA (20% of patients experiencing a Grade 3-4 IRR). Overall, 7% of patients experienced an IRR leading to discontinuation of GAZYVA. The incidence of IRR with subsequent infusions was 3% with the second 1000 mg dose and 1% thereafter. No Grade 3-5 IRR were reported beyond the first 1000 mg infusions of Cycle 1.
In patients who received the recommended measures for prevention of IRRs as described in Dosage & Administration, a decreased incidence of all Grades IRRs was observed. The rates of Grade 3-4 IRRs (which are based on a relatively low number of patients) were similar before and after mitigation measures were implemented.
Non-Hodgkin Lymphoma: In Cycle 1, the overall incidence of IRRs was higher in patients receiving GAZYVA plus chemotherapy compared to patients in the comparator arm. In patients receiving GAZYVA plus chemotherapy, the incidence of IRR was highest on Day 1 and gradually decreased with subsequent infusions. This decreasing trend continued during maintenance therapy with GAZYVA alone.
Overall, 4% of patients experienced an infusion related reaction leading to discontinuation of GAZYVA.
Neutropenia and infections: Chronic Lymphocytic Leukaemia: The incidence of neutropenia was higher in the GAZYVA plus chlorambucil arm compared to the rituximab plus chlorambucil arm with the neutropenia resolving spontaneously or with use of granulocyte colony-stimulating factors. The incidence of infection was 38% in the GAZYVA plus chlorambucil arm and 37% in the rituximab plus chlorambucil arm (with Grade 3-5 events reported in 12% and 14%, respectively and fatal events reported in <1% in both treatment arms). Cases of prolonged neutropenia (2% in the GAZYVA plus chlorambucil arm and 4% in rituximab plus chlorambucil arm) and late onset neutropenia (16% in the GAZYVA plus chlorambucil arm and 12% in the rituximab plus chlorambucil arm) were also reported (See Precautions).
Non-Hodgkin Lymphoma: In the GAZYVA plus chemotherapy arm, the incidence of neutropenia was higher relative to the comparator arm with an increased risk during the induction period. The incidence of prolonged neutropenia and late onset neutropenia in the GAZYVA plus chemotherapy arm were 3% and 7%, respectively. The incidence of infection was 78% in the GAZYVA plus chemotherapy arm (with Grade 3-5 events reported in 22% and fatal events reported in 3% of patients). Patients who received G-CSF prophylaxis had a lower rate of Grade 3-5 infections. (See Precautions).
Thrombocytopenia and haemorrhagic events: Chronic Lymphocytic Leukaemia: The incidence of thrombocytopenia was higher in the GAZYVA plus chlorambucil arm compared to the rituximab plus chlorambucil arm especially during the first cycle. Four percent of patients treated with GAZYVA arm plus chlorambucil experienced acute thrombocytopenia (occurring within 24 hours after the GAZYVA infusion) (See Precautions). The overall incidence of haemorrhagic events was similar in the GAZYVA treated arm and in the rituximab treated arm. The number of fatal haemorrhagic events was balanced between the treatment arms; however, all of the events in patients treated with GAZYVA were reported in Cycle 1. A clear relationship between thrombocytopenia and haemorrhagic events has not been established.
Non-Hodgkin Lymphoma: Thrombocytopenia occurred more frequently during Cycle 1 in the GAZYVA plus chemotherapy arm. Thrombocytopenia occurring during or 24 hours from end of infusion (acute thrombocytopenia) was more frequently observed in patients treated with GAZYVA plus chemotherapy than in the relevant comparator arm. The incidence of haemorrhagic AEs was similar across all treatment arms. Haemorrhagic events and Grade 3-5 haemorrhagic events occurred in 12% and 4% of patients, respectively. While fatal haemorrhagic events occurred in less than 1% of patients, none of these fatal AEs occurred in Cycle 1.
Progressive multifocal leukoencephalopathy (PML): PML has been reported in patients treated with GAZYVA (see Precautions).
Hepatitis B Reactivation: Cases of hepatitis B reactivation have been reported in patients treated with GAZYVA (see Precautions).
Worsening of Pre-existing Cardiac Conditions: Cases of fatal cardiac events have been reported in patients treated with GAZYVA (see Precautions).
Gastro-Intestinal Perforation: Cases of gastro-intestinal perforation have been reported in patients receiving GAZYVA, mainly in NHL.
Maintenance treatment in iNHL patients: In GAO4753g, patients in the B arm received 6 months of induction treatment only, whereas after the induction period, patients in the G+B arm continued on with GAZYVA maintenance treatment. During the maintenance period with GAZYVA, the most common adverse reactions were cough (20.3%), neutropenia (12.7%), upper respiratory tract infections (12.0%), diarrhoea (10.1%), bronchitis (9.5%), sinusitis (9.5%), nausea (8.9%), fatigue (8.49%), infusion related reactions (8.2%), urinary tract infections (7.0%), nasopharyngitis (7.0%), pyrexia (7.0%), arthralgia (6.3%), vomiting (5.7%), rash (5.7%), pneumonia (5.1%), dyspnea (5.1%) and pain in extremity (5.1%). The most common grade 3-5 adverse reactions were neutropenia (10.8%), febrile neutropenia (1.9%) and anaemia, thrombocytopenia, pneumonia, sepsis, upper respiratory tract infection, and urinary tract infection (all at 1.3%).
Laboratory Abnormalities: Transient elevation in liver enzymes (AST, ALT, ALP) has been observed shortly after the first infusion of GAZYVA.
For additional information, see further information on selected adverse drug reactions: Neutropenia and Infections and Thrombocytopenia and Haemorrhagic events as previously mentioned.
Post Marketing Experience: No data to report.
View ADR Monitoring Form