Pharmacotherapeutic group: Natural and semisynthetic oestrogens, plain.
ATC code: G03CA03.
Pharmacology: Pharmacodynamics: The active ingredient, synthetic 17β-estradiol, is chemically and biologically identical to endogenous human estradiol.
Endogenous 17β-estradiol induces and maintains the primary and secondary female sexual characteristics. The biological effect of 17β-estradiol is carried out through a number of specific oestrogen receptors. The steroid receptor complex is bound to the cells' DNA and induces synthesis of specific proteins.
Maturation of the vaginal epithelium is dependent upon oestrogens. Oestrogens increase the number of superficial and intermediate cells and decrease the number of basal cells in vaginal smear.
Oestrogens maintain vaginal pH around normal range (4.5) which enhances normal bacterial flora.
Treatment of vaginal oestrogen deficiency symptoms: vaginally applied oestrogen alleviates the symptoms of vaginal atrophy due to oestrogen deficiency in postmenopausal women.
A 12-month, double-blind, randomised, parallel group, placebo-controlled, multicentre study was conducted to evaluate the efficacy and safety of Femiest 10 micrograms in the treatment of postmenopausal vaginal atrophy symptoms.
After 12 weeks of treatment with Femiest 10 micrograms, the change from baseline, in comparison with placebo treatment, demonstrated significant improvements in the three primary endpoints: Vaginal Maturation Index and Value, normalisation of vaginal pH and relief of the moderate/severe urogenital symptoms considered most bothersome by the subjects.
Endometrial safety of Femiest 10 micrograms was evaluated in the previously mentioned trial and a second, open-label, multicentre trial. In total, 386 women underwent endometrial biopsy at the beginning and at the end of 52 weeks treatment. Incidence rate of hyperplasia and/or carcinoma was 0.52% (95% CI 0.06%, 1.86%), indicating no increased risk.
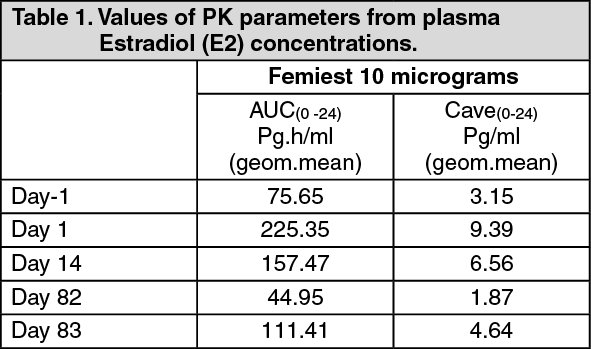
Pharmacokinetics: Absorption: Oestrogens are well absorbed through the skin, mucous membranes and the gastrointestinal tract. After vaginal administration, estradiol is absorbed circumventing first-pass metabolism. A 12-week, single-centre, randomised, open-label, multiple dose, parallel-group trial was conducted to evaluate the extent of systemic absorption of estradiol from the Femiest 10 micrograms tablet. Subjects were randomised 1:1 to receive either 10 micrograms or 25 micrograms Femiest. Plasma levels of estradiol (E2), oestrone (E1) and oestrone sulfate (E1S) were determined. The AUC
(0-24) for plasma E2 levels increased almost proportionally after the administration of 10 micrograms and 25 micrograms Femiest. The AUC
(0-24) indicated higher systemic estradiol levels for the 10 micrograms E2 tablet as compared to baseline on treatment days 1, 14 and 83, being statistically significant at days 1 and 14 (Table 1). However, average plasma E2 concentrations (C
ave (0-24)) at all evaluated days remained within the normal postmenopausal range in all subjects. The data from days 82 and 83 as compared to baseline indicate that there is no cumulative effect during twice-weekly maintenance therapy. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The levels of oestrone and oestrone sulfate seen after 12 weeks of Femiest 10 micrograms administration did not exceed baseline levels, i.e. no accumulation of oestrone or oestrone sulfate was observed.
Distribution: The distribution of exogenous oestrogens is similar to that of endogenous oestrogens. Oestrogens are widely distributed in the body and are generally found in higher concentrations in the sex hormone target organs. Oestrogens circulate in the blood largely bound to sex hormone binding globulin (SHBG) and albumin.
Biotransformation: Exogenous oestrogens are metabolized in the same manner as endogenous oestrogens. The metabolic transformations take place mainly in the liver. Estradiol is converted reversibly to oestrone and both can be converted to estriol which is the major urinary metabolite. In postmenopausal women, a significant portion of the circulating oestrogens exists as sulfate conjugates, especially oestrone sulfate, which serves as a circulating reservoir for the formation of more active oestrogens.
Elimination: Estradiol, oestrone and estriol are excreted in the urine along with glucuronide and sulfate conjugates.
Special patient groups: The extent of systemic absorption of estradiol during treatment with Femiest 10 micrograms has been evaluated in postmenopausal women aged 60-70 (mean age 65.4) only.
Toxicology: Preclinical safety data: 17β-estradiol is a well-known substance. Non-clinical studies provided no additional data of relevance to clinical safety beyond those already included in other sections of the monograph.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
