Pharmacotherapeutic group: Immunosuppressants, selective immunosuppressants.
ATC code: L04AA33.
Pharmacology: Pharmacodynamics: Vedolizumab is a gut-selective immunosuppressive biologic. It is a humanized monoclonal antibody that binds specifically to the α
4β
7 integrin, which is preferentially expressed on gut homing T helper lymphocytes. By binding to α
4β
7 on certain lymphocytes, vedolizumab inhibits adhesion of these cells to mucosal addressin cell adhesion molecule-1 (MAdCAM-1), but not to vascular cell adhesion molecule-1 (VCAM-1). MAdCAM-1 is mainly expressed on gut endothelial cells and plays a critical role in the homing of T lymphocytes to tissues within the gastrointestinal tract. Vedolizumab does not bind to, nor inhibit function of, the α
4β
1 and α
Eβ
7 integrins.
The α
4β
7 integrin is expressed on a discrete subset of memory T helper lymphocytes which preferentially migrate into the gastrointestinal (GI) tract and cause inflammation that is characteristic of ulcerative colitis and Crohn's disease, both of which are chronic inflammatory immunologically mediated conditions of the GI tract. Vedolizumab reduces gastrointestinal inflammation in UC and CD patients. Inhibiting the interaction of α
4β
7 with MAdCAM-1 with vedolizumab prevents transmigration of gut-homing memory T helper lymphocytes across the vascular endothelium into parenchymal tissue in nonhuman primates and induced a reversible 3-fold elevation of these cells in peripheral blood. The murine precursor of vedolizumab alleviated gastrointestinal inflammation in colitic cotton-top tamarins, a model of ulcerative colitis.
In healthy subjects, ulcerative colitis patients, or Crohn's disease patients, vedolizumab does not elevate neutrophils, basophils, eosinophils, B-helper and cytotoxic T lymphocytes, total memory T helper lymphocytes, monocytes or natural killer cells, in the peripheral blood with no leukocytosis observed.
Vedolizumab did not affect immune surveillance and inflammation of the central nervous system in Experimental Autoimmune Encephalomyelitis in non-human primates, a model of multiple sclerosis. Vedolizumab did not affect immune responses to antigenic challenge in the dermis and muscle (see Precautions). In contrast, vedolizumab inhibited an immune response to a gastrointestinal antigenic challenge in healthy human volunteers (see Precautions).
Immunogenicity: Antibodies to vedolizumab may develop during vedolizumab treatment most of which are neutralising. The formation of anti-vedolizumab antibodies is associated with increased clearance of vedolizumab and lower rates of clinical remission.
Infusion related reactions after vedolizumab infusion are reported in subjects with anti-vedolizumab antibodies.
Pharmacodynamic effects: In clinical trials with vedolizumab at doses ranging from 2 to 10 mg/kg, >95% saturation of α
4β
7 receptors on subsets of circulating lymphocytes involved in gut immune surveillance was observed in patients.
Vedolizumab did not affect CD4
+ and CD8
+ trafficking into the CNS as evidenced by the lack of change in the ratio of CD4
+/CD8
+ in cerebrospinal fluid pre- and post-vedolizumab administration in healthy human volunteers. These data are consistent with investigations in nonhuman primates which did not detect effects on immune surveillance of the CNS.
Clinical efficacy: Ulcerative Colitis: The efficacy and safety of vedolizumab for the treatment of adult patients with moderately to severely active ulcerative colitis (Mayo score 6 to 12 with endoscopic sub score ≥2) was demonstrated in a randomised, double-blind, placebo-controlled study evaluating efficacy endpoints at Week 6 and Week 52 (GEMINI I). Enrolled patients had failed at least one conventional therapy, including corticosteroids, immunomodulators, and/or the TNFα antagonist infliximab (including primary non-responders). Concomitant stable doses of oral aminosalicylates, corticosteroids and/or immunomodulators were permitted.
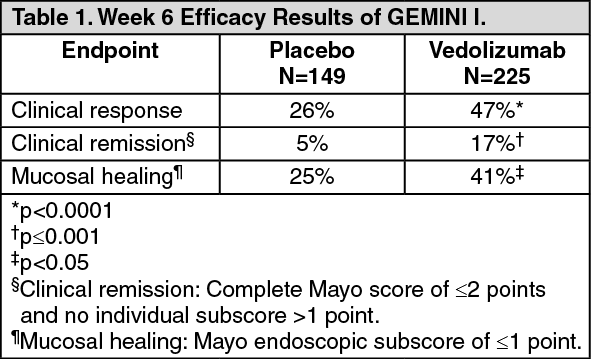
For the evaluation of the Week 6 endpoints, 374 patients were randomised in a double-blind fashion (3:2) to receive vedolizumab 300 mg or placebo at Week 0 and Week 2. Primary endpoint was the proportion of patients with clinical response (defined as reduction in complete Mayo score of ≥3 points and ≥30% from baseline with an accompanying decrease in rectal bleeding subscore of ≥1 point or absolute rectal bleeding subscore of ≤1 point) at Week 6. Table 1 shows the results from the primary and secondary endpoints evaluated. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The beneficial effect of vedolizumab on clinical response, remission and mucosal healing was observed both in patients with no prior TNFα antagonist exposure as well as in those who had failed prior TNFα antagonist therapy.
In GEMINI I, two cohorts of patients received vedolizumab at Week 0 and Week 2: cohort 1 patients were randomised to receive either vedolizumab 300 mg or placebo in a double-blind fashion, and cohort 2 patients were treated with open-label vedolizumab 300 mg. To evaluate efficacy at Week 52, 373 patients from cohort 1 and 2 who were treated with vedolizumab and had achieved clinical response at Week 6 were randomised in a double-blind fashion (1:1:1) to one of the following regimens beginning at Week 6: vedolizumab 300 mg every eight weeks, vedolizumab 300 mg every four weeks, or placebo every four weeks. Beginning at Week 6, patients who had achieved clinical response and were receiving corticosteroids were required to begin a corticosteroid-tapering regimen. Primary endpoint was the proportion of patients in clinical remission at Week 52. Table 2 shows the results from the primary and secondary endpoints evaluated. (See Table 2.)
Click on icon to see table/diagram/image
Exploratory analyses provide additional data on key subpopulations studied. Approximately one-third of patients had failed prior TNFα antagonist therapy. Among these patients, 37% receiving vedolizumab every eight weeks, 35% receiving vedolizumab every four weeks, and 5% receiving placebo achieved clinical remission at Week 52. Improvements in durable clinical response (47%, 43%, 16%), mucosal healing (42%, 48%, 8%), durable clinical remission (21%, 13%, 3%) and corticosteroid-free clinical remission (23%, 32%, 4%) were seen in the prior TNFα antagonist failure population treated with vedolizumab every eight weeks, vedolizumab every four weeks and placebo, respectively.
Patients who failed to demonstrate response at Week 6 remained in the study and received vedolizumab every four weeks. Clinical response using partial Mayo scores was achieved at Week 10 and Week 14 by greater proportions of vedolizumab patients (32% and 39%, respectively) compared with placebo patients (15% and 21%, respectively).
Patients who lost response to vedolizumab when treated every eight weeks were allowed to enter an open-label extension study and receive vedolizumab every four weeks. In these patients, clinical remission was achieved in 25% of patients at Week 28 and Week 52.
Patients who achieved a clinical response after receiving vedolizumab at Week 0 and 2 and were then randomised to placebo (for 6 to 52 weeks) and lost response were allowed to enter the open-label extension study and receive vedolizumab every four weeks. In these patients, clinical remission was achieved in 45% of patients by 28 weeks and 36% of patients by 52 weeks.
In this open-label extension study, the benefits of vedolizumab treatment as assessed by partial Mayo score, clinical remission, and clinical response were shown for up to 196 weeks.
Health-related quality of life (HRQOL) was assessed by Inflammatory Bowel Disease Questionnaire (IBDQ), a disease specific instrument, and SF-36 and EQ-5D, which are general measures. Exploratory analysis show clinically meaningful improvements were observed for vedolizumab groups, and the improvements were significantly greater as compared with the placebo group at Week 6 and Week 52 on EQ-5D and EQ-5D VAS scores, all subscales of IBDQ (bowel symptoms, systemic function, emotional function and social function), and all subscales of SF-36 including the Physical Component Summary (PCS) and Mental Component Summary (MCS).
Crohn's Disease: The efficacy and safety of vedolizumab for the treatment of adult patients with moderately to severely active Crohn's Disease (Crohn's Disease Activity Index [CDAI] score of 220 to 450) were evaluated in two studies (GEMINI II and III). Enrolled patients have failed at least one conventional therapy, including corticosteroids, immunomodulators, and/or TNFα antagonists (including primary non-responders). Concomitant stable doses of oral corticosteroids, immunomodulators, and antibiotics were permitted.
The GEMINI II Study was a randomised, double-blind, placebo-controlled study evaluating efficacy endpoints at Week 6 and Week 52. Patients (n=368) were randomised in a double-blind fashion (3:2) to receive two doses of vedolizumab 300 mg or placebo at Week 0 and Week 2. The two primary endpoints were the proportion of patients in clinical remission (defined as CDAI score ≤150 points) at Week 6 and the proportion of patients with enhanced clinical response (defined as a ≥100-point decrease in CDAI score from baseline) at Week 6 (see Table 3).
GEMINI II contained two cohorts of patients that received vedolizumab at Weeks 0 and 2: Cohort 1 patients were randomised to receive either vedolizumab 300 mg or placebo in a double-blind fashion, and Cohort 2 patients were treated with open-label vedolizumab 300 mg. To evaluate efficacy at Week 52, 461 patients from Cohorts 1 and 2, who were treated with vedolizumab and had achieved clinical response (defined as a ≥70-point decrease in CDAI score from baseline) at Week 6, were randomised in a double-blind fashion (1:1:1) to one of the following regimens beginning at Week 6: vedolizumab 300 mg every eight weeks, vedolizumab 300 mg every four weeks, or placebo every four weeks. Patients showing clinical response at Week 6 were required to begin corticosteroid tapering. Primary endpoint was the proportion of patients in clinical remission at Week 52 (see Table 4).
The GEMINI III Study was a second randomised, double-blind, placebo-controlled study that evaluated efficacy at Week 6 and Week 10 in the subgroup of patients defined as having failed at least one conventional therapy and failed TNFα antagonist therapy (including primary non-responders) as well as the overall population, which also included patients who failed at least one conventional therapy and were naïve to TNFα antagonist therapy. Patients (n=416), which included approximately 75% TNFα antagonist failures patients, were randomised in a double-blind fashion (1:1) to receive either vedolizumab 300 mg or placebo at Weeks 0, 2, and 6. The primary endpoint was the proportion of patients in clinical remission at Week 6 in the TNFα antagonist failure subpopulation. As noted in Table 3, although the primary endpoint was not met, exploratory analyses show that clinically meaningful results were observed. (See Tables 3 and 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Exploratory analyses examined the effects of concomitant corticosteroids and immunomodulators on induction of remission with vedolizumab. Combination treatment, most notably with concomitant corticosteroids, appeared to be more effective in inducing remission in Crohn's disease than vedolizumab alone or with concomitant immunomodulators, which showed a smaller difference from placebo in the rate of remission. Clinical remission rate in GEMINI II at Week 6 was 10% (difference from placebo 2%, 95% CI: -6, 10) when administered without corticosteroids compared to 20% (difference from placebo 14%, 95% CI: -1, 29) when administered with concomitant corticosteroids. In GEMINI III at Week 6 and 10 the respective clinical remission rates were 18% (difference from placebo 3%, 95% CI: -7, 13) and 22% (difference from placebo 8%, 95% CI: -3, 19) when administered without corticosteroids compared to 20% (difference from placebo 11%, 95% CI: 2, 20) and 35% (difference from placebo 23%, 95% CI: 12, 33) respectively when administered with concomitant corticosteroids. These effects were seen whether or not immunomodulators were also concomitantly administered.
Exploratory analyses provide additional data on key subpopulations studied. In GEMINI II, approximately half of patients had previously failed TNFα antagonist therapy. Among these patients, 28% receiving vedolizumab every eight weeks, 27% receiving vedolizumab every four weeks, and 13% receiving placebo achieved clinical remission at Week 52. Enhanced clinical response was achieved in 29%, 38%, 21%, respectively, and corticosteroid-free clinical remission was achieved in 24%, 16%, 0%, respectively.
Patients who failed to demonstrate response at Week 6 in GEMINI II were retained in the study and received vedolizumab every four weeks. Enhanced clinical response was observed at Week 10 and Week 14 for greater proportions of vedolizumab patients 16% and 22%, respectively, compared with placebo patients 7% and 12%, respectively. There was no clinically meaningful difference in clinical remission between treatment groups at these time points. Analyses of Week 52 clinical remission in patients who were non-responders at Week 6 but achieved response at Week 10 or Week 14 indicate that non-responder CD patients may benefit from a dose of vedolizumab at Week 10.
Patients who lost response to vedolizumab when treated every eight weeks in GEMINI II were allowed to enter an open-label extension study and received vedolizumab every four weeks. In these patients, clinical remission was achieved in 23% of patients at Week 28 and 32% of patients at Week 52.
Patients who achieved a clinical response after receiving vedolizumab at Week 0 and 2 and were then randomised to placebo (for 6 to 52 weeks) and lost response were allowed to enter the open-label extension study and receive vedolizumab every four weeks. In these patients, clinical remission was achieved in 46% of patients by 28 weeks and 41% of patients by 52 weeks.
In this open-label extension study, clinical remission and clinical response were observed in patients for up to 196 weeks.
Exploratory analysis showed clinically meaningful improvements were observed for the vedolizumab every four weeks and every eight weeks groups in GEMINI II and the improvements were significantly greater as compared with the placebo group from baseline to Week 52 on EQ-5D and EQ-5D VAS scores, total IBDQ score, and IBDQ subscales of bowel symptoms and systemic function.
Paediatric population: The European Medicines Agency has deferred the obligation to submit the results of studies with vedolizumab in one or more subsets of the paediatric population in ulcerative colitis and Crohn's disease (see Dosage & Administration for information on paediatric use).
Pharmacokinetics: The single and multiple dose pharmacokinetics of vedolizumab have been studied in healthy subjects and in patients with moderate to severely active ulcerative colitis or Crohn's disease.
In patients administered 300 mg vedolizumab as a 30 minute intravenous infusion on Weeks 0 and 2, mean serum trough concentrations at Week 6 were 27.9 mcg/ml (SD ± 15.51) in ulcerative colitis and 26.8 mcg/ml (SD ± 17.45) in Crohn's disease. Starting at Week 6, patients received 300 mg vedolizumab every eight or four weeks. In patients with ulcerative colitis, mean steady-state serum trough concentrations were 11.2 mcg/ml (SD ± 7.24) and 38.3 mcg/ml (SD ± 24.43), respectively. In patients with Crohn's disease mean steady-state serum trough concentrations were 13.0 mcg/ml (SD ± 9.08) and 34.8 mcg/ml (SD ± 22.55), respectively.
Distribution: Population pharmacokinetic analyses indicate that the distribution volume of vedolizumab is approximately 5 litres. The plasma protein binding of vedolizumab has not been evaluated. Vedolizumab is a therapeutic monoclonal antibody and is not expected to bind to plasma proteins.
Vedolizumab does not pass the blood brain barrier after intravenous administration. Vedolizumab 450 mg administered intravenously was not detected in the cerebrospinal fluid of healthy subjects.
Elimination: Population pharmacokinetic analyses indicate that vedolizumab has a total body clearance of approximately 0.157 L/day and a serum half-life of 25 days. The exact elimination route of vedolizumab is not known. Population pharmacokinetic analyses suggest that while low albumin, higher body weight and, prior treatment with anti-TNF drugs may increase vedolizumab clearance, the magnitude of their effects is not considered to be clinically relevant.
Linearity: Vedolizumab exhibited linear pharmacokinetics at serum concentrations greater than 1 mcg/ml.
Special populations: Age does not impact the vedolizumab clearance in ulcerative colitis and Crohn's disease patients based on the population pharmacokinetic analyses. No formal studies have been conducted to examine the effects of either renal or hepatic impairment on the pharmacokinetics of vedolizumab.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction and development.
Long-term animal studies with vedolizumab to assess its carcinogenic potential have not been conducted because pharmacologically responsive models to monoclonal antibodies do not exist. In a pharmacologically responsive species (cynomolgus monkeys), there was no evidence of cellular hyperplasia or systemic immunomodulation that could potentially be associated with oncogenesis in 13- and 26-week toxicology studies. Furthermore, no effects were found of vedolizumab on the proliferative rate or cytotoxicity of a human tumour cell line expressing the α
4β
7 integrin in vitro.
No specific fertility studies in animals have been performed with vedolizumab. No definitive conclusion can be drawn on the male reproductive organs in cynomolgus monkey repeated dose toxicity study, but given the lack of binding of vedolizumab to male reproductive tissue in monkey and human, and the intact male fertility observed in β7 integrin-knockout mice, it is not expected that vedolizumab will affect male fertility.
Administration of vedolizumab to pregnant cynomolgus monkeys during most of gestation resulted in no evidence of effects on teratogenicity, prenatal or postnatal development in infants up to 6 months of age. Low levels (<300 mcg/L) of vedolizumab were detected on post-partum Day 28 in the milk of 3 of 11 cynomolgus monkeys treated 100 mg/kg of vedolizumab dosed every 2 weeks and not in any animals that received 10 mg/kg.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image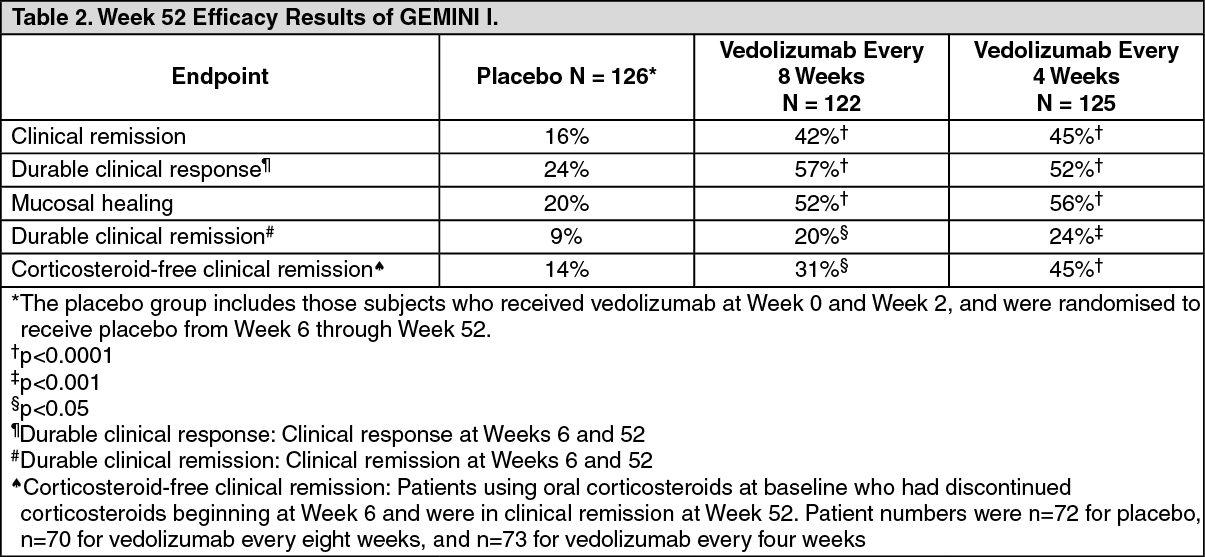 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image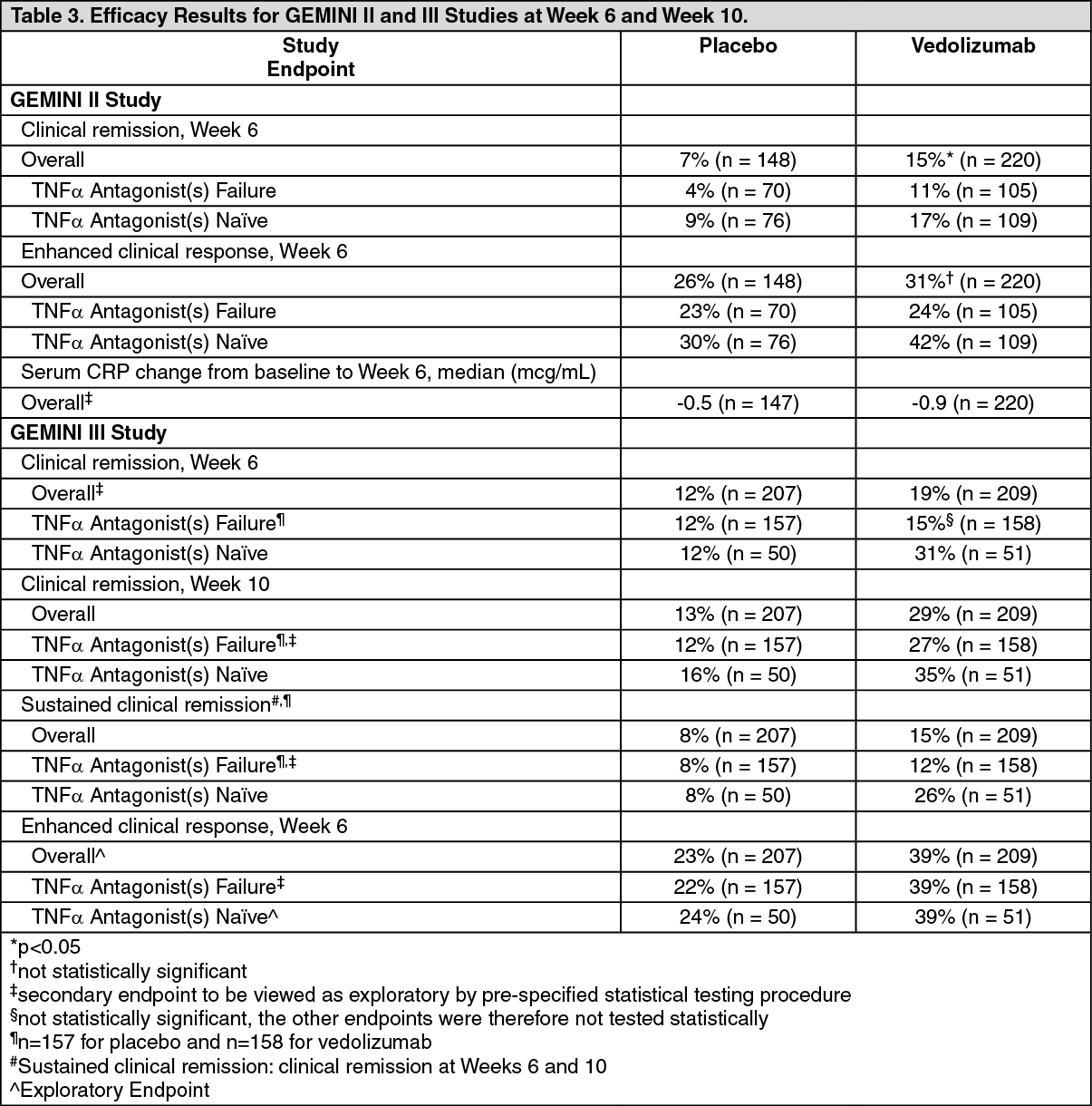 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image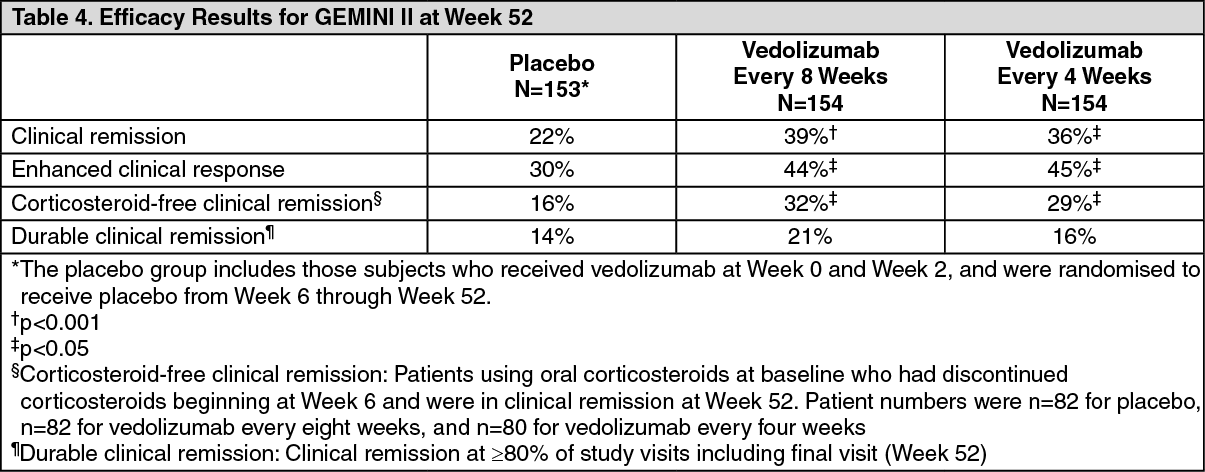 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
