


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Dydrogesterone is an orally-active progestogen which produces a complete secretory endometrium in an oestrogen-primed uterus thereby providing protection against the increased risk for endometrium hyperplasia and/or carcinogenesis induced by estrogens. It is indicated in all cases of endogenous progesterone deficiency. Dydrogesterone has no estrogenic, no androgenic, no thermogenic, no anabolic and no corticoid activity.
Clinical efficacy and safety: Luteal support as part of an Assisted Reproductive Technology (ART) treatment: A Double-Blind, Double-Dummy, Randomized, Two-arm, Multicenter Study Comparing the Efficacy, Safety, and Tolerability of Oral Dydrogesterone 30 mg daily versus Intravaginal Micronized Progesterone Capsules 600 mg daily for Luteal Support in In-Vitro Fertilization (LOTUS I).
The study achieved its primary objective of demonstrating non-inferiority of oral dydrogesterone compared to intravaginal micronized progesterone in terms of the presence of fetal heartbeats at 12 weeks gestation (10 weeks pregnancy).
In the patient population, pregnancy rates at 12 weeks' gestation (Week 10) were 37.6% and 33.1% in the dydrogesterone and micronized progesterone groups, respectively. The difference in the pregnancy rate between the groups was 4.7 (95% CI, -1.2, 10.6).
Within the safety sample of 1029 subjects with at least one dose of study medication administered, the incidence of the most frequently reported TEAE was similar between the two treatment groups.
Due to the nature of the studied patient population/indication a number of early abortions/miscarriages are expected; especially until 12 weeks' gestation (pregnancy week 10) as the expected pregnancy rate at this time point is about 35%.
The safety profile observed in this study is as expected taking into account the well-established safety profile of dydrogesterone and the treatment population/indication.
Adolescent population: Limited clinical trial data indicate that dydrogesterone is efficacious in relieving symptoms of dysmenorrhoea, premenstrual syndrome, dysfunctional uterine bleeding and irregular cycles in the population of patients younger than 18 years of age in a similar manner as in the adult population.
Pharmacokinetics: Absorption: Following oral administration, dydrogesterone is rapidly absorbed with a Tmax between 0.5 and 2.5 hours. The absolute bioavailability of dydrogesterone (oral 20 mg dose versus 7.8 mg intravenous infusion) is 28 %.
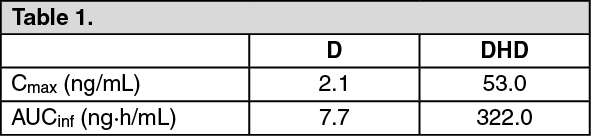
The following table provides pharmacokinetic parameters of dydrogesterone (D) and 20α-dihydrodydrogesterone (DHD) after single dose administration of 10 mg dydrogesterone: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDistribution: After intravenous administration of dydrogesterone the steady-state volume of distribution is approximately 1400 L. Dydrogesterone and DHD are more than 90% bound to plasma proteins.
Metabolism: Following oral administration, dydrogesterone is rapidly metabolized to DHD. The levels of the main active metabolite DHD peak about 1.5 hours postdose. The plasma levels of DHD are substantially higher as compared to the parent drug. The AUC and Cmax ratios of DHD to dydrogesterone are in the order of 40 and 25, respectively. Mean terminal half lives of dydrogesterone and DHD vary between 5 to 7 and 14 to 17 hours, respectively. A common feature of all metabolites characterised is the retention of the 4,6 diene-3-one configuration of the parent compound and the absence of 17α-hydroxylation. This explains the lack of estrogenic and androgenic effects of dydrogesterone.
Elimination: After oral administration of labelled dydrogesterone, on average 63% of the dose is excreted into the urine. Total plasma clearance is 6.4 L/min.
Within 72 hours excretion is complete. DHD is present in the urine predominantly as the glucuronic acid conjugate.
Dose and time dependencies: The single and multiple dose pharmacokinetics are linear in the oral dose range 2.5 to 10 mg. Comparison of the single and multiple dose kinetics shows that the pharmacokinetics of dydrogesterone and DHD are not changed as a result of repeated dosing. Steady state was reached after 3 days of treatment.
Toxicology: Preclinical safety data: Non-clinical data obtained from conventional studies on single and repeated dose toxicity, genotoxicity and carcinogenic potential reveal no special hazard for humans.
Reproduction toxicity studies in rats have shown an increased incidence of prominent nipples (between day 11 and day 19 of age) and of hypospadias in the male offspring at high dosages not comparable to human exposure. The actual risk of hypospadias in humans cannot be determined in animal studies due to major species differences in metabolism between rats and humans (see Use in Pregnancy & Lactation).
Limited animal safety data suggest that dydrogesterone has prolongating effects on parturition, which is consistent with its progestogenic activity.