


 Sign Out
Sign Out

Complete blood counts, liver chemistries and serum creatinine should be obtained prior to first dose.
Subsequent Treatment Cycles: Cycles should be repeated every 4 weeks. The dose may be increased to 100 mg/m2 if no beneficial effect is seen after 2 treatment cycles and if no toxicity other than nausea and vomiting has occurred. It is recommended that patients be treated for a minimum of 4 to 6 cycles.
However, complete or partial response may require more than 4 treatment cycles. Treatment may be continued as long as the patient continues to benefit.
Patients should be monitored for hematologic response and renal toxicities, and dosage delay or reduction as described as follows may be necessary.
Dose Adjustment Based on Hematology Laboratory Values: For patients with baseline (start of treatment) WBC ≥ 3.0 x 109/L, ANC ≥ 1.5 x 109/L, and platelets ≥ 75.0 x 109/L, adjust the dose as follows, based on nadir counts for any given cycle: See Table 5.
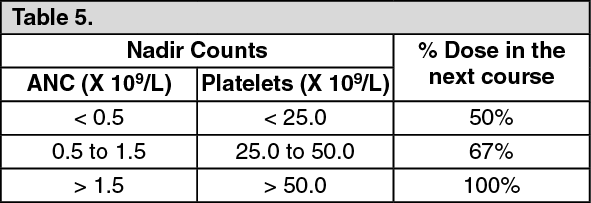 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor patients whose baseline counts are WBC < 3.0 x 109/L, ANC < 1.5 x 109/L, or platelets < 75.0 x 109/L, dose adjustments should be based on nadir counts and bone marrow biopsy cellularity at the time of the nadir as noted as follows, unless there is clear improvement in differentiation (percentage of mature granulocytes is higher and ANC is higher than at onset of that course) at the time of the next cycle, in which case the dose of the current treatment should be continued. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIf a nadir as defined in the table as previously mentioned has occurred, the next course of treatment should be given 28 days after the start of the preceding course, provided that both the WBC and the platelet counts are > 25% above the nadir and rising. If a > 25% increase above the nadir is not seen by day 28, counts should be reassessed every 7 days. If a 25% increase is not seen by day 42, then the patient should be treated with 50% of the scheduled dose.
Dosage Adjustment Based on Renal Function and Serum Electrolytes: If unexplained reductions in serum bicarbonate levels to less than 20 mEq/L occur, the dosage should be reduced by 50% on the next course. Similarly, if unexplained elevations of BUN or serum creatinine occur, the next cycle should be delayed until values return to normal or baseline and the dose should be reduced by 50% on the next course (see PRECAUTIONS).
Use in Geriatric Patients: Azacitidine and its metabolites are known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function (see PRECAUTIONS).
Preparation of azacitidine: Azacitidine is a cytotoxic drug and, as with other potentially toxic compounds, caution should be exercised when handling and preparing azacitidine suspensions. (See Handling and Disposal under Cautions for Usage.)
If reconstituted azacitidine comes into contact with the skin, immediately and thoroughly wash with soap and water. If it comes into contact with mucous membranes, flush thoroughly with water.
The azacitidine vial is single-use and does not contain any preservatives. Unused portions of each vial should be discarded properly. Do not save any unused portions for later administration.
Preparation for Subcutaneous Administration: Azacitidine should be reconstituted aseptically with 4 mL sterile water for injection. The diluent should be injected slowly into the vial. Vigorously shake or roll the vial until a uniform suspension is achieved. The suspension will be cloudy. The resulting suspension will contain azacitidine 25 mg/mL. Do not filter the suspension after reconstitution. Doing so could remove the active substance.
Preparation for Immediate Subcutaneous Administration: Doses greater than 4 mL should be divided equally into 2 syringes. The product may be held at room temperature for up to 1 hour, but must be administered within 1 hour after reconstitution.
Preparation for Delayed Subcutaneous Administration: The reconstituted product may be kept in the vial or drawn into a syringe. Doses greater than 4 mL should be divided equally into 2 syringes. The product must be refrigerated immediately, and may be held under refrigerated conditions (2-8°C, 36-46°F) for up to 8 hours. After removal from refrigerated conditions, the suspension may be allowed to equilibrate to room temperature for up to 30 minutes prior to administration.
Subcutaneous Administration: To provide a homogeneous suspension, the contents of the syringe must be re-suspended by inverting the syringe 2-3 times and vigorously rolling the syringe between the palms for 30 seconds immmediately prior to administration.
Azacitidine is administered subcutaneously. Doses greater than 4 mL should be divided equally into 2 syringes and injected into 2 separate sites. Rotate sites for each injection (thigh, abdomen, or upper arm). New injections should be given at least 1 inch from an old site and never into areas where the sites is tender, bruised, red, or hard.
Suspension Stability: Azacitidine reconstituted for subcutaneous administration may be stored for up to 1 hour at 25°C (77°F) or for up to 8 hours between 2°C and 8°C (36°F and 46°F).
Preparation for Intravenous Administration: Reconstitute that appropriate number of azacitidine vials to achieve the desired dose. Reconstitute each vial with 10 mL sterile water for injection. Vigorously shake or roll the vial until all solids are dissolved. The resulting solution will contain azacitidine 10 mg/mL. The solution should be clear. Parental drug product should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Withdraw the required amount of azacitidine solution to deliver the desired dose and inject into a 50-100 mL infusion bag of either 0.9% Sodium Chloride Injection or Lactated Ringer's Injection.
Intravenous Solution Incompatibility: Azacitidine is incompatible with 5% Dextrose solutions, Hespan, or solutions that contain bicarbonate. These solutions have the potential to increase the rate of degradation of azacitidine and should therefore be avoided.
Intravenous Administration: Azacitidine solution is administered intravenously. Administer the total dose over a period of 10-40 minutes. The administration must be completed within 1 hour of reconstitution of the azacitidine vial.
Solution Stability: Azacitidine reconstituted for intravenous administration may be stored at 25°C (77°F), but administration must be completed within 1 hour of reconstitution.