


 Sign Out
Sign Out

Abiraterone may cause hypertension, hypokalemia and fluid retention as a pharmacodynamics consequence of its mechanism of action. In clinical studies, anticipated mineralocorticoid adverse reactions were seen more commonly in patients treated with abiraterone acetate than in patients treated with placebo: hypokalemia 21% versus 11%, hypertension 16% versus 11% and fluid retention (peripheral oedema) 26% versus 20%, respectively. In patients treated with abiraterone acetate, CTCAE (version 3.0) Grades 3 and 4 hypokalemia and CTCAE (version 3.0) Grades 3 and 4 hypertension were observed in 4% and 2% of patients, respectively. Mineralocorticoid reactions generally were able to be successfully managed medically. Concomitant use of a corticosteroid reduces the incidence and severity of these adverse reactions.
Tabulated summary of adverse reactions: In studies of patients with metastatic advanced prostate cancer who were using a luteinising hormone-releasing hormone (LHRH) analogue, or were previously treated with orchiectomy, abiraterone was administered at a dose of 1,000 mg daily in combination with low dose prednisone or prednisolone (either 5 or 10 mg daily depending on the indication).
Adverse reactions observed during clinical studies and post-marketing experience are listed as follows by frequency category. Frequency categories are defined as follows: very common ( ≥1/10): common (≥ 1/100 to < 1/10): uncommon ( ≥ 1/1,000 to <1/100); rare ( ≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000) and not known (frequency cannot be estimated from the available data).
Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. (See table.)
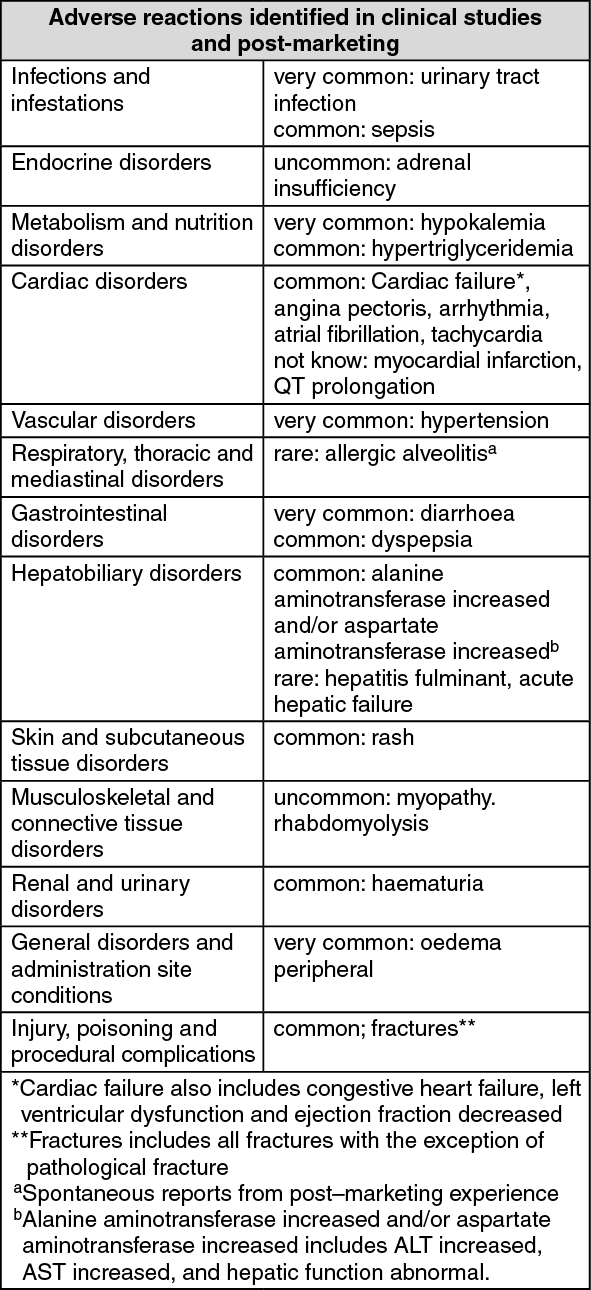 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe following CTCAE (version 3.0) Grade 3 adverse reactions occurred in patients treated with abiraterone acetate: hypokalemia 3%; urinary tract infection, alanine aminotransferase increased, hypertension, aspartate aminotransferase increased, fractures 2%; peripheral oedema, cardiac failure, and atrial fibrillation 1% each. CTCAE (version 3.0) Grade 3 hypertri-glyceridemia and angina pectoris occurred in < 1% of patients. CTCAE (version 3.0) Grade 4 peripheral oedema, hypokalemia, urinary tract infection, cardiac failure and fractures occurred in <1% of patients.
Description of selected adverse reactions: Cardiovascular reactions: Both phase 3 studies excluded patients with uncontrolled hypertension, clinically significant heart disease as evidenced by myocardial infarction, or arterial thrombotic events in the past 6 months, severe or unstable angina, or NYHA Class III or IV heart failure (study 301) or Class II to IV heart failure (study 302) or cardiac ejection fraction measurement of < 50%. All patients enrolled (both active and placebo-treated patients) were concomitantly treated with androgen deprivation therapy, predominantly with the use of LHRH analogues, which has been associated with diabetes, myocardial infarction, cerebrovascular accident and sudden cardiac death. The incidence of cardiovascular adverse reactions in the phase 3 studies in patients taking abiraterone acetate versus patients taking placebo were as follows: hypertension 14.5% VS. 10.5%, atrial fibrillation 3.4% vs. 3.4%, tachycardia 2.8% vs. 1.7%, angina pectoris 1.9% vs. 0.9%, cardiac failure 1.9% vs. 0.6%, and arrhythmia 1.1% vs. 0.4%.
Hepatotoxicity: Hepatotoxicity with elevated ALT, aspartate transaminase (AST) and total bilirubin has been reported in patients treated with abiraterone acetate. Across all clinical studies, liver function test elevations (ALT or AST increases of > 5x ULN or bilirubin increases > 1.5x ULN) were reported in approximately 4% of patients who received abiraterone acetate, typically during the first 3 months after starting treatment. In the 301 clinical study, patients whose baseline ALT or AST were elevated were more likely to experience liver function test elevations than those beginning with normal values. When elevations of either ALT or AST > 5x ULN, or elevations in bilirubin > 3x ULN were observed, abiraterone acetate was withheld or discontinued. In two instances marked increases in liver function tests occurred. These two patients with normal baseline hepatic function, experienced ALT or AST elevations 15 to 40x ULN and bilirubin elevations 2 to 6x ULN. Upon discontinuation of treatment, both patients had normalisation of their liver function tests and one patient was re-treated without recurrence of the elevations. In study 302, Grade 3 or 4 ALT or AST elevations were observed in 35 (6.5%) patients treated with abiraterone acetate. Aminotransferase elevations resolved in all but 3 patients (2 with new multiple liver metastases and 1 with AST elevation approximately 3 weeks after the last dose of abiraterone acetate). Treatment discontinuations due to ALT and AST increases were reported in 1.7% and 1.3% of patients treated with abiraterone acetate and 0.2% and 0% of patients treated with placebo, respectively. No deaths were reported due to hepatotoxicity event.
In clinical trials, the risk for hepatotoxicity was mitigated by exclusion of patients with baseline hepatitis or significant abnormalities of liver function tests. In the 301 trial, patients with baseline ALT and AST ≥ 2.5x ULN in the absence of liver metastases and > 5x ULN in the presence of liver metastases were excluded. In the 302 trial, patients with liver metastases were not eligible and patients with baseline ALT and AST ≥ 2.5x ULN were excluded. Abnormal liver function tests developing in patients participating in clinical trials were vigorously managed by requiring treatment interruption and permitting re-treatment only after return of liver function tests to the patient's baseline. Patients with elevations of ALT or AST > 20x ULN were not re-treated. The safety of re-treatment in such patients is unknown. The mechanism for hepatotoxicity is not understood.
View ADR Monitoring Form