


 Sign Out
Sign Out



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment discontinuation due to adverse events occurred in 2% (20/1015) of patients receiving ZERBAXA and 1.9% (20/1032) of patients receiving comparator drugs. Renal impairment (including the terms renal impairment, renal failure, and renal failure acute) led to discontinuation of treatment in 5/1015 (0.5%) subjects receiving ZERBAXA and none in the comparator arms.
Increased Mortality: In the cIAI trials (Phase 2 and 3), death occurred in 2.5% (14/564) of patients receiving ZERBAXA and in 1.5% (8/536) of patients receiving meropenem. The causes of death varied and included worsening and/or complications of infection, surgery and underlying conditions.
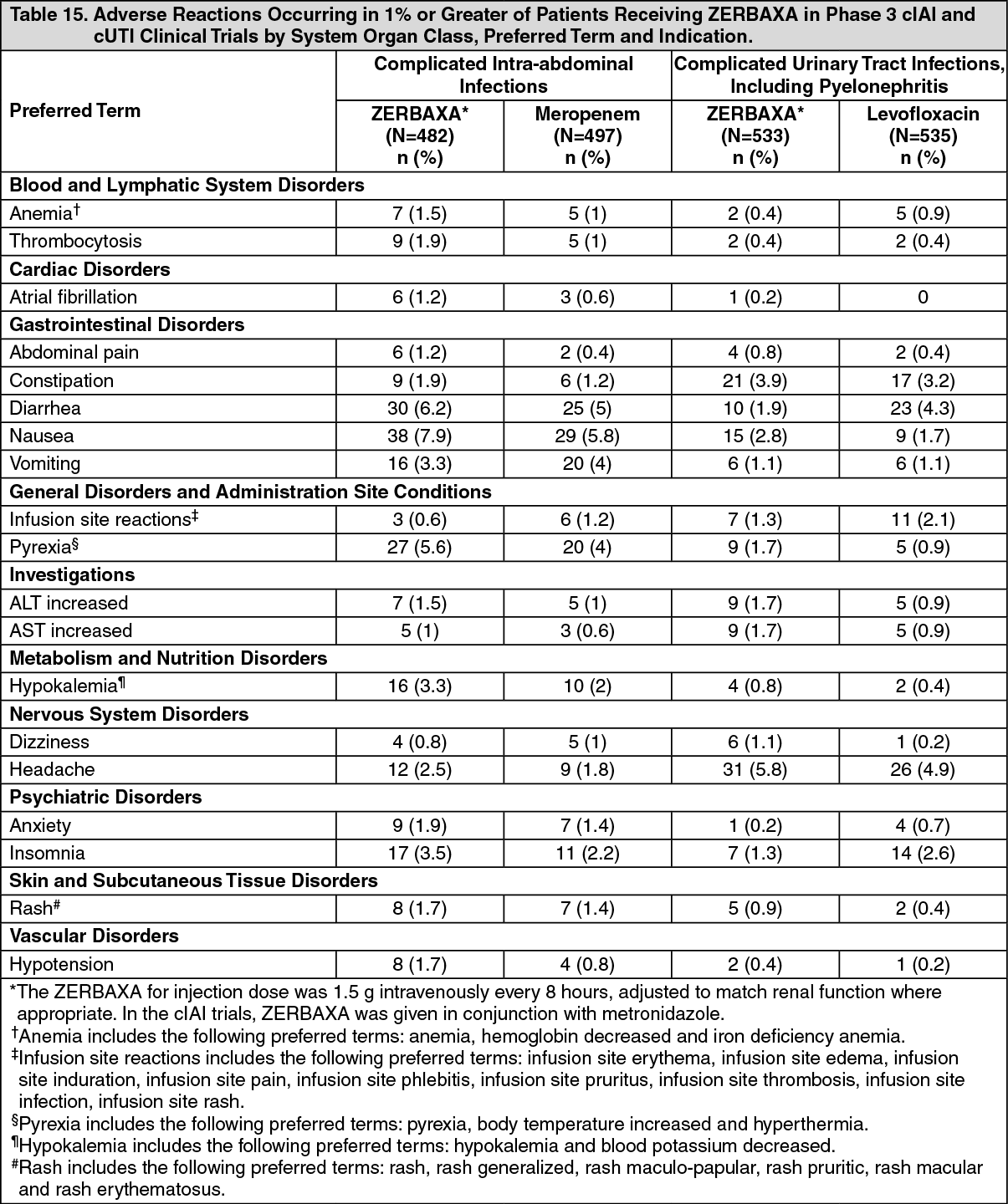
Less Common Adverse Reactions in Phase 3 cIAI and cUTI Clinical Trials: The following selected adverse reactions were reported in ZERBAXA-treated subjects at a rate of less than 1%: Cardiac disorders: tachycardia, angina pectoris.
Gastrointestinal disorders: gastritis, abdominal distension, dyspepsia, flatulence, ileus paralytic.
Infections and infestations: candidiasis including oropharyngeal and vulvovaginal, fungal urinary tract infection, Clostridium difficile colitis.
Investigations: increased serum gamma-glutamyl transpeptidase (GGT), increased serum alkaline phosphatase, positive Coombs test.
Metabolism and nutrition disorders: hyperglycemia, hypomagnesemia, hypophosphatemia.
Nervous system disorders: ischemic stroke.
Renal and urinary system: renal impairment, renal failure.
Respiratory, thoracic and mediastinal disorders: dyspnea.
Skin and subcutaneous tissue disorders: urticaria.
Vascular disorders: venous thrombosis.
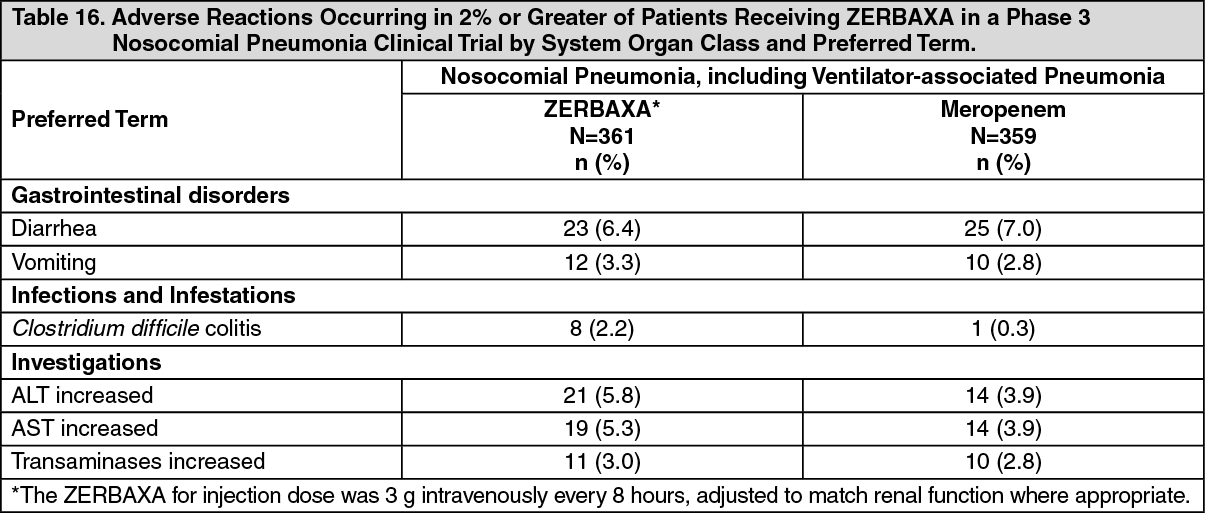
Nosocomial Pneumonia, including Ventilator-associated Pneumonia: ZERBAXA was evaluated in a Phase 3 comparator-controlled clinical trial for nosocomial pneumonia, which included a total of 361 patients treated with ZERBAXA (3 g every 8 hours, adjusted based on renal function where appropriate) and 359 patients treated with comparator (meropenem 1 g every 8 hours) for up to 14 days. The mean age of treated patients was 60 years (range 18 to 98 years), across treatment arms. About 44% of the subjects were 65 years of age or older. Most patients (71%) enrolled in the trial were male. All subjects were mechanically ventilated and 92% were in an intensive care unit (ICU) at randomization. The median APACHE II score was 17. Table 16 lists adverse reactions occurring in 2% or greater of patients receiving ZERBAXA in a Phase 3 nosocomial pneumonia clinical trial. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment discontinuation due to treatment-related adverse events occurred in 1.1% (4/361) of patients receiving ZERBAXA and 1.4% (5/359) of patients receiving meropenem.
Less Common Adverse Reactions in a Phase 3 Nosocomial Pneumonia Clinical Trial: The following selected adverse reactions were reported in ZERBAXA-treated subjects at a rate of less than 2%: Infections and infestations: Clostridium difficile infection.
Investigations: liver function test abnormal, blood alkaline phosphatase increased, gamma-glutamyltransferase increased, Clostridium test positive, Coombs direct test positive.
Laboratory Values: The development of a positive direct Coombs test may occur during treatment with ZERBAXA. The incidence of seroconversion to a positive direct Coombs test was 0.2% in patients receiving ZERBAXA and 0% in patients receiving the comparator in the cUTI and cIAI clinical trials. The incidence of seroconversion to a positive direct Coombs test was 31.2% in patients receiving ZERBAXA and 3.6% in patients receiving meropenem in the nosocomial pneumonia clinical trial. In clinical studies, there was no evidence of hemolysis in patients who developed a positive direct Coombs test in any treatment group.
View ADR Monitoring Form