


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: SOLIRIS is a recombinant humanised monoclonal IgG2/4k antibody that binds to the human C5 complement protein and inhibits the activation of terminal complement. The SOLIRIS antibody contains human constant regions and murine complementarity-determining regions grafted onto the human framework light- and heavy-chain variable regions. SOLIRIS is composed of two 448 amino acid heavy chains and two 214 amino acid light chains and has a molecular weight of approximately 148kDa.
SOLIRIS is produced in a murine myeloma (NS0 cell line) expression system and purified by affinity and ion exchange chromatography. The bulk drug substance manufacturing process also includes specific viral inactivation and removal steps.
Mechanism of Action: Eculizumab, the active ingredient in SOLIRIS, is a terminal complement inhibitor that specifically binds to the complement protein C5 with high affinity, thereby inhibiting its cleavage to C5a and C5b and preventing the generation of the terminal complement complex C5b-9. Eculizumab preserves the early components of complement activation that are essential for opsonization of microorganisms and clearance of immune complexes.
In PNH patients, uncontrolled terminal complement activation and the resulting complement-mediated intravascular haemolysis are blocked with SOLIRIS treatment.
In most PNH patients, eculizumab serum concentrations of approximately 35 microgram/ml are sufficient for essentially complete inhibition of terminal complement-mediated intravascular haemolysis.
In PNH, chronic administration of SOLIRIS resulted in a rapid and sustained reduction in complement-mediated haemolytic activity.
In aHUS patients, uncontrolled terminal complement activation and the resulting complement-mediated thrombotic microangiopathy are blocked with SOLIRIS treatment.
All patients treated with SOLIRIS when administered as recommended demonstrated rapid and sustained reduction in terminal complement activity. In all aHUS patients, eculizumab serum concentrations of approximately 50 - 100 microgram/ml are sufficient for essentially complete inhibition of terminal complement activity.
In aHUS, chronic administration of SOLIRIS resulted in a rapid and sustained reduction in complement-mediated thrombotic microangiopathy.
Clinical efficacy and safety: Paroxysmal Nocturnal Haemoglobinuria (PNH): The safety and efficacy of SOLIRIS in PNH patients with haemolysis were assessed in a randomized, double-blind, placebo-controlled 26-week study (C04-001). PNH patients were also treated with SOLIRIS in a single arm 52-week study (C04-002); and in a long-term extension study (E05-001). Patients received meningococcal vaccination prior to receipt of SOLIRIS. In all studies, the dose of eculizumab was 600 mg every 7 ± 2 days for 4 weeks, followed by 900 mg 7 ± 2 days later, then 900 mg every 14 ± 2 days for the study duration. Eculizumab was administered as an intravenous infusion over 25 - 45 minutes. An observational non-interventional Registry in patients with PNH (M07-001) was also initiated to characterize the natural history of PNH in untreated patients and the clinical outcomes during SOLIRIS treatment.
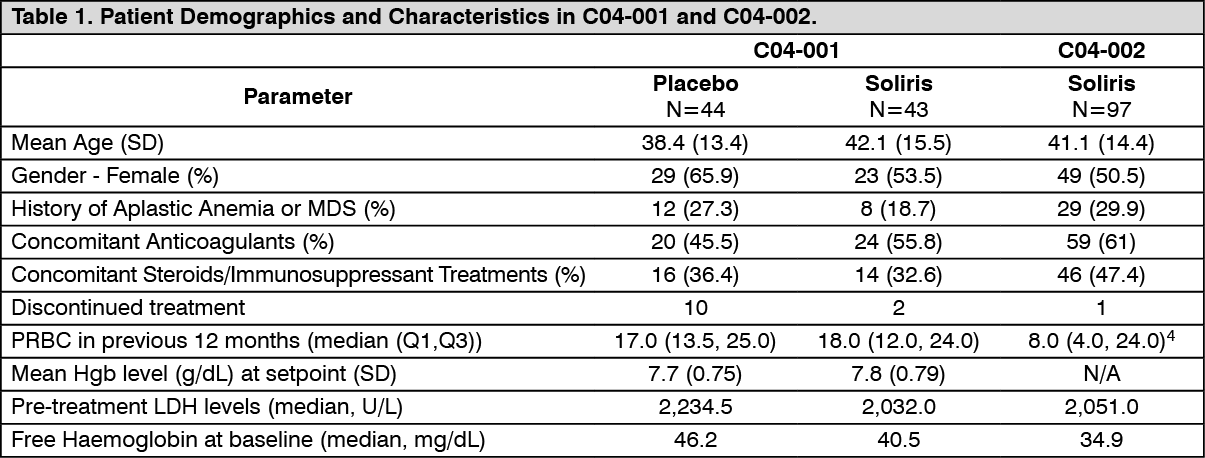
In study C04-001 (TRIUMPH) PNH patients with at least 4 transfusions in the prior 12 months, flow cytometric confirmation of at least 10% PNH cells and platelet counts of at least 100,000/microliter were randomized to either SOLIRIS (n = 43) or placebo (n = 44). Prior to randomization, all patients underwent an initial observation period to confirm the need for RBC transfusion and to identify the haemoglobin concentration (the "set-point") which would define each patient's haemoglobin stabilization and transfusion outcomes. The haemoglobin set-point was less than or equal to 9 g/dL in patients with symptoms and was less than or equal to 7 g/dL in patients without symptoms. Primary efficacy endpoints were haemoglobin stabilization (patients who maintained a haemoglobin concentration above the haemoglobin set-point and avoid any RBC transfusion for the entire 26 week period) and blood transfusion requirement. Fatigue and health-related quality of life were relevant secondary endpoints. Haemolysis was monitored mainly by the measurement of serum LDH levels, and the proportion of PNH RBCs was monitored by flow cytometry. Patients receiving anticoagulants and systemic corticosteroids at baseline continued these medications. Major baseline characteristics were balanced (see Table 1).
In the non-controlled study C04-002 (SHEPHERD), PNH patients with at least one transfusion in the prior 24 months and at least 30,000 platelets/microliter received SOLIRIS over a 52-week period. Concomitant medications included anti-thrombotic agents in 63% of the patients and systemic corticosteroids in 40% of the patients. Baseline characteristics are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
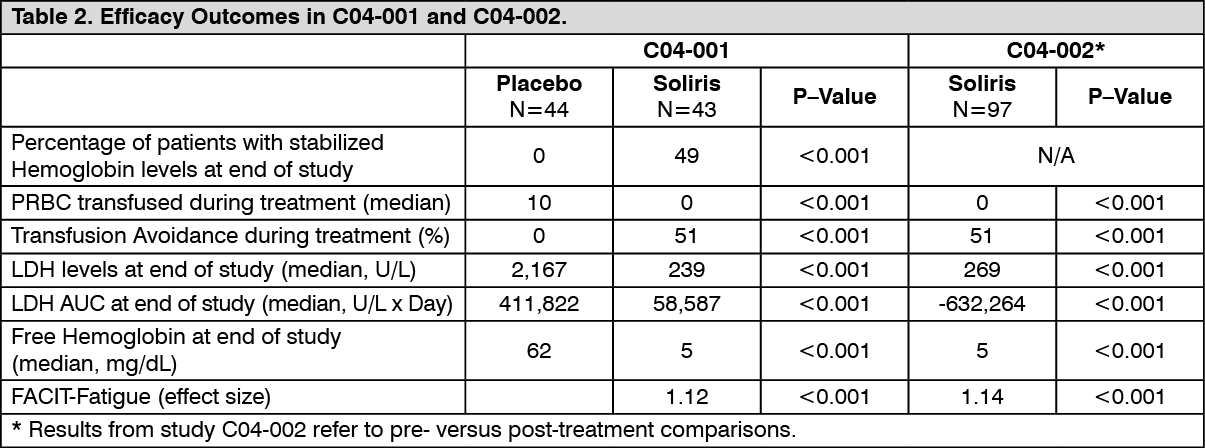
Click on icon to see table/diagram/imageIn TRIUMPH, study patients treated with SOLIRIS had significantly reduced (p< 0.001) haemolysis resulting in improvements in anaemia as indicated by increased haemoglobin stabilization and reduced need for RBC transfusions compared to placebo treated patients (see Table 2). These effects were seen among patients within each of the three pre-study RBC transfusion strata (4 - 14 units; 15 - 25 units; > 25 units). After 3 weeks of SOLIRIS treatment, patients reported less fatigue and improved health-related quality of life. Because of the study sample size and duration, the effects of SOLIRIS on thrombotic events could not be determined. In SHEPHERD study, 96 of the 97 enrolled patients completed the study (one patient died following a thrombotic event). A reduction in intravascular haemolysis as measured by serum LDH levels was sustained for the treatment period and resulted in increased transfusion avoidance, a reduced need for RBC transfusion and less fatigue. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFrom the 195 patients that originated in C04-001, C04-002 and other initial studies, SOLIRIS-treated PNH patients were enrolled in a long-term extension study (E05-001). All patients sustained a reduction in intravascular haemolysis over a total SOLIRIS exposure time ranging from 10 to 54 months. There were fewer thrombotic events with SOLIRIS treatment than during the same period of time prior to treatment. However, this finding was shown in non-controlled clinical trials.
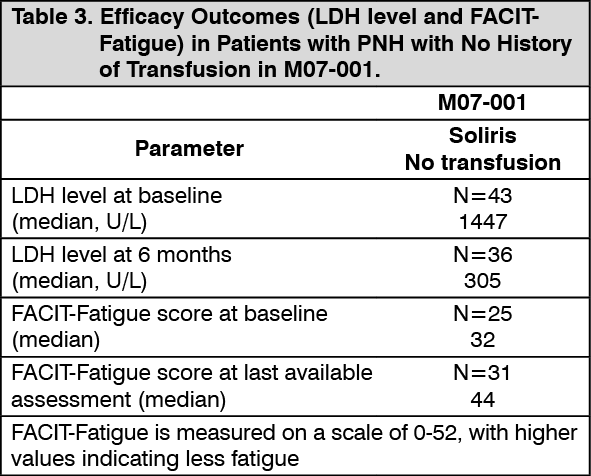
The PNH registry (M07-001) was used to evaluate the efficacy of SOLIRIS in PNH patients with no history of RBC transfusion. These patients had high disease activity as defined by elevated haemolysis (LDH ≥1.5x ULN) and the presence of related clinical symptom(s): fatigue, haemoglobinuria, abdominal pain, shortness of breath (dyspnoea), anaemia (haemoglobin <100 g/L), major adverse vascular event (including thrombosis), dysphagia, or erectile dysfunction.
In the PNH Registry, patients treated with SOLIRIS were observed to have a reduction in haemolysis and associated symptoms. At 6 months, patients treated with SOLIRIS with no history of RBC transfusion had significantly (p<0.001) reduced LDH levels (median LDH of 305 U/L; Table 3). Furthermore, 74% of the patients treated with SOLIRIS experienced clinically meaningful improvements in FACIT-Fatigue score (i.e., increase by 4 points or more) and 84% in EORTC fatigue score (i.e., decrease by 10 points or more). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAtypical Haemolytic Uraemic Syndrome (aHUS): Data from 100 patients in four prospective controlled studies, three in adult and adolescent patients (C08-002A/B C08-003A/B, C10-004) one in paediatric and adolescent patients (C10-003) and 30 patients in one retrospective study (C09-001r) were used to evaluate the efficacy of SOLIRIS in the treatment of aHUS.
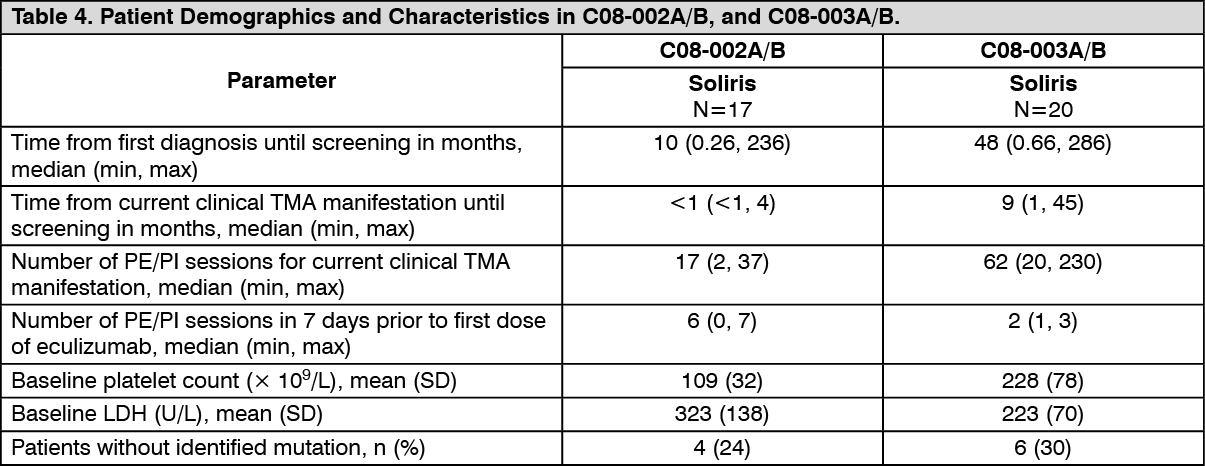
Study C08-002A/B was a prospective, controlled, open-label study which accrued patients in the early phase of aHUS with evidence of clinical thrombotic microangiopathy manifestations with platelet count ≤ 150 x 109/L despite PE/PI, and LDH and serum creatinine above upper limits of normal.
Study C08-003A/B was a prospective, single arm, open-label study which accrued patients with longer term aHUS without apparent evidence of clinical thrombotic microangiopathy manifestations and receiving chronic PE/PI (≥ 1 PE/PI treatment every two weeks and no more than 3 PE/PI treatments/week for at least 8 weeks before the first dose). Patients in both prospective studies were treated with SOLIRIS for 26 weeks and most patients enrolled into a long-term, open-label extension study. All patients enrolled in both prospective studies had an ADAMTS-13 level above 5%.
Patients received meningococcal vaccination prior to receipt of SOLIRIS or received prophylactic treatment with appropriate antibiotics until 2 weeks after vaccination. In all studies, the dose of SOLIRIS in adult and adolescent aHUS patients was 900 mg every 7 ± 2 days for 4 weeks, followed by 1,200 mg 7 ± 2 days later, then 1,200 mg every 14 ± 2 days for the study duration. SOLIRIS was administered as an intravenous infusion over 35 minutes. The dosing regimen in paediatric patients and adolescents weighing less than 40 kg was defined based on a pharmacokinetic (PK) simulation that identified the recommended dose and schedule based on body weight (see Dosage & Administration).
Primary endpoints included platelet count change from baseline in Study C08-002A/B and thrombotic microangiopathy (TMA) event-free status in Study C08-003A/B. Additional endpoints included TMA intervention rate, haematologic normalization, complete TMA response, changes in LDH, renal function and quality of life. TMA-event free status was defined as the absence for at least 12 weeks of the following: decrease in platelet count of > 25% from baseline, PE/PI, and new dialysis. TMA interventions were defined as PE/PI or new dialysis. Haematologic normalization was defined as normalization of platelet counts and LDH levels sustained for ≥ 2 consecutive measurements for ≥ 4 weeks. Complete TMA response was defined as haematologic normalization and a ≥ 25% reduction in serum creatinine sustained in ≥ 2 consecutive measurements for ≥ 4 weeks.
Baseline characteristics are show in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
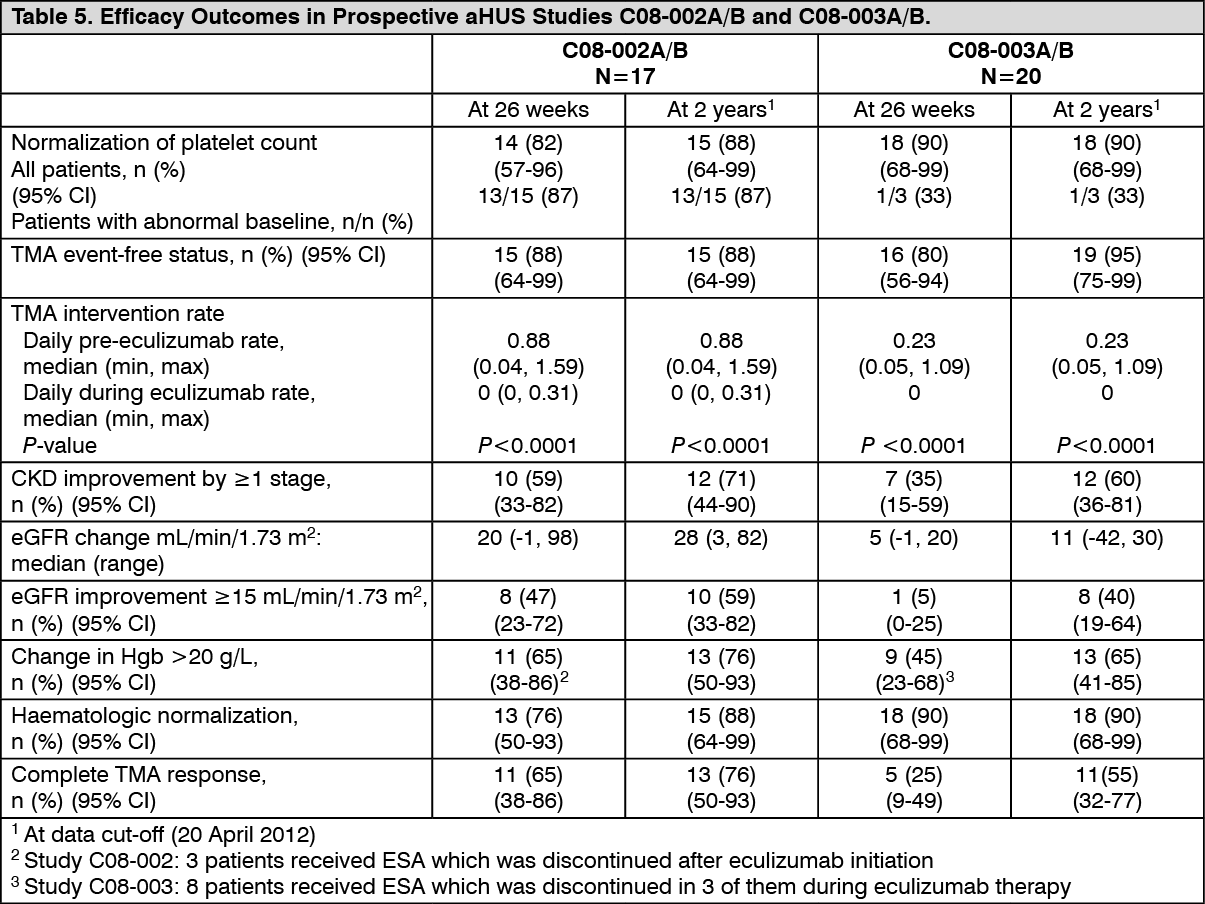
Click on icon to see table/diagram/imagePatients in aHUS Study C08-002A/B received SOLIRIS for a minimum of 26 weeks. After completion of the initial 26-week treatment period, most patients continued to receive SOLIRIS by enrolling into an extension study. In aHUS Study C08-002A/B, the median duration of SOLIRIS therapy was approximately100 weeks (range: 2 weeks to 145 weeks).
A reduction in terminal complement activity and an increase in platelet count relative to baseline were observed after commencement of SOLIRIS. Reduction in terminal complement activity was observed in all patients after commencement of SOLIRIS. Table 5 summarizes the efficacy results for aHUS Study C08-002A/B. All rates of efficacy endpoints improved or were maintained through 2 years of treatment. Complete TMA response was maintained by all responders. When treatment was continued for more than 26 weeks, two additional patients achieved and maintained Complete TMA response due to normalization of LDH (1 patient) and a decrease in serum creatinine (2 patients). Renal function, as measured by eGFR, was improved and maintained during SOLIRIS treatment. Four of the five patients who required dialysis at study entry were able to discontinue dialysis for the duration of SOLIRIS treatment, and one patient developed a new dialysis requirement. Patients reported improved health-related quality of life (QoL).
In aHUS Study C08-002A/B, responses to SOLIRIS were similar in patients with and without identified mutations in genes encoding complement regulatory factor proteins.
Patients in aHUS Study C08-003A/B received SOLIRIS for a minimum of 26 weeks. After completion of the initial 26-week treatment period, most patients continued to receive SOLIRIS by enrolling into an extension study. In aHUS Study C08-003A/B, the median duration of SOLIRIS therapy was approximately 114 weeks (range: 26 to 129 weeks). Table 5 summarizes the efficacy results for aHUS Study C08-003A/B.
In aHUS Study C08-003A/B, responses to SOLIRIS were similar in patients with and without identified mutations in genes encoding complement regulatory factor proteins. Reduction in terminal complement activity was observed in all patients after commencement of SOLIRIS. All rates of efficacy endpoints improved or were maintained through 2 years of treatment. Complete TMA response was maintained by all responders. When treatment was continued for more than 26 weeks, six additional patients achieved and maintained Complete TMA response due to a decrease in serum creatinine. No patients required new dialysis with SOLIRIS. Renal function, as measured by median eGFR, increased during SOLIRIS therapy. (See Table 5.)
 Click on icon to see table/diagram/image
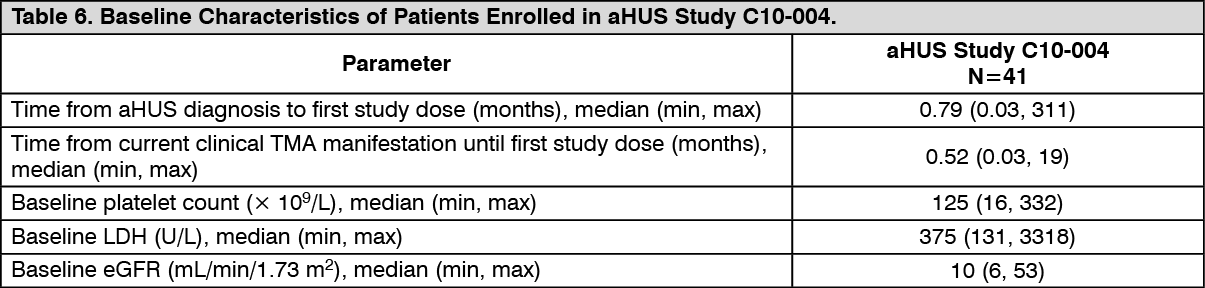
Click on icon to see table/diagram/imageaHUS Study C10-004 enrolled 41 patients who displayed signs of thrombotic microangiopathy (TMA). In order to qualify for enrolment, patients were required to have a platelet count < lower limit of normal range (LLN), evidence of haemolysis such as an elevation in serum LDH, and serum creatinine above the upper limits of normal, without the need for chronic dialysis. The median patient age was 35 (range: 18 to 80 years). All patients enrolled in aHUS Study C10-004 had an ADAMTS-13 level above 5%. Fifty-one percent of patients had an identified complement regulatory factor mutation or auto-antibody. A total of 35 patients received PE/PI prior to eculizumab. Table 6 summarizes the key baseline clinical and disease-related characteristics of patients enrolled in aHUS C10-004. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients in aHUS Study C10-004 received SOLIRIS for a minimum of 26 weeks. After completion of the initial 26-week treatment period, most patients elected to continue on chronic dosing.
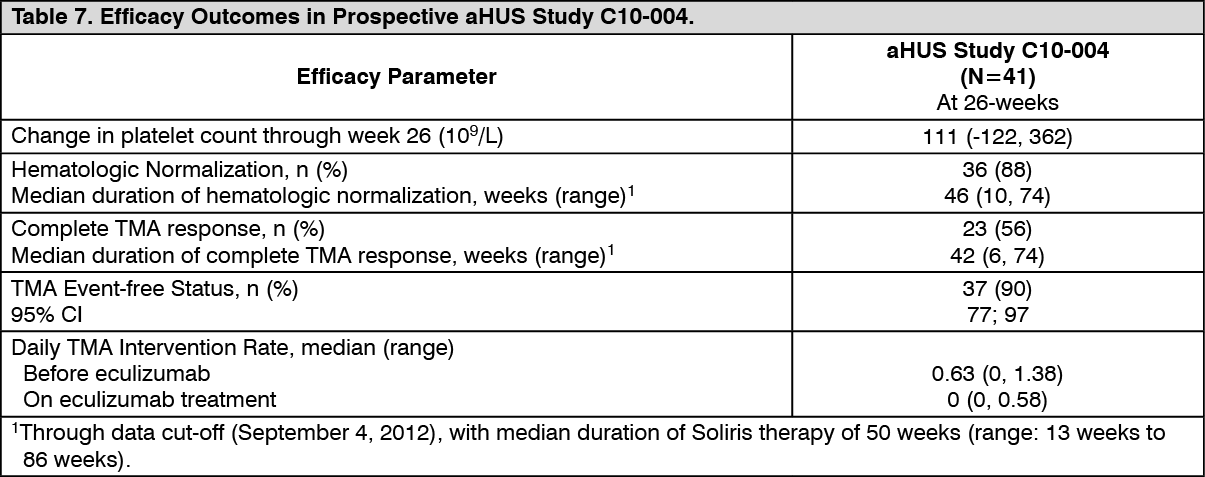
Reduction in terminal complement activity and an increase in platelet count relative to baseline were observed after commencement of SOLIRIS. SOLIRIS reduced signs of complement-mediated TMA activity, as shown by an increase in mean platelet counts from baseline to 26 weeks. In aHUS C10-004, mean (±SD) platelet count increased from 119 ± 66 x109/L at baseline to 200 ± 84 x109/L by one week; this effect was maintained through 26 weeks (mean platelet count (±SD) at week 26: 252 ± 70 x109/L). Renal function, as measured by eGFR, was improved during SOLIRIS therapy. Twenty of the 24 patients who required dialysis at baseline were able to discontinue dialysis during SOLIRIS treatment. Table 7 summarizes the efficacy results for aHUS study C10-004. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLonger term treatment with SOLIRIS (median 52 weeks ranging from 15 to 126 weeks) was associated with an increased rate of clinically meaningful improvements in adult patients with aHUS. When SOLIRIS treatment was continued for more than 26 weeks, three additional patients (63% of patients in total) achieved Complete TMA response and four additional patients (98% of patients in total) achieved hematologic normalization. At the last evaluation, 25 of 41 patients (61%) achieved eGFR improvement of ≥ 15 ml/min/1.73 m2 from baseline.
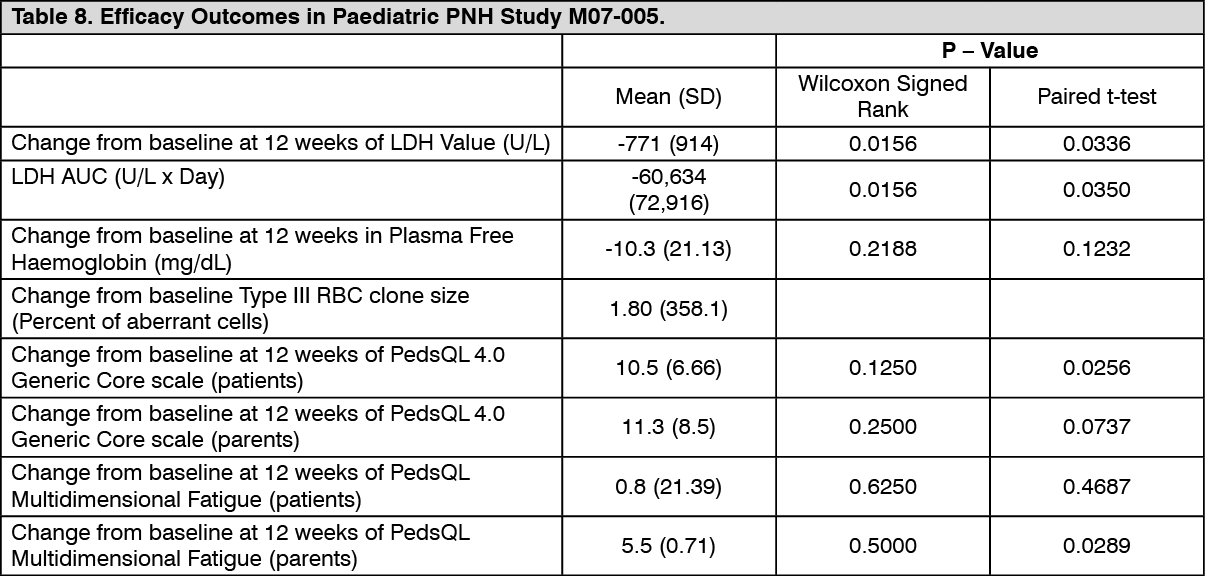
Paediatric Population: Paroxysmal Nocturnal Haemoglobinuria: A total of 7 PNH paediatric patients, with a median weight of 57.2 kg (range of 48.6 to 69.8 kg) and aged from 11 to 17 years (median age: 15.6 years), received SOLIRIS in study M07-005.
Treatment with eculizumab at the proposed dosing regimen in the paediatric population was associated with a reduction of intravascular haemolysis as measured by serum LDH level. It also resulted in a marked decrease or elimination of blood transfusions, and a trend towards an overall improvement in general function. The efficacy of eculizumab treatment in paediatric PNH patients appears to be consistent with that observed in adult PNH patients enrolled in PNH pivotal Studies (C04-001 and C04-002) (Tables 2 and 8). (See Table 8.)
 Click on icon to see table/diagram/image
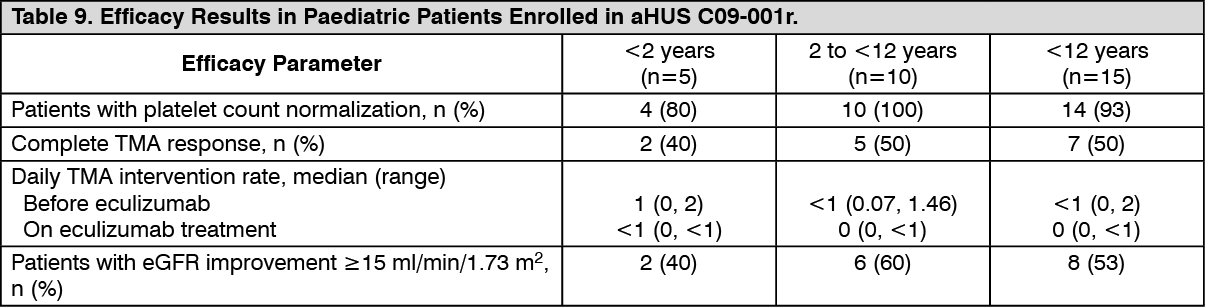
Click on icon to see table/diagram/imageAtypical Haemolytic Uremic Syndrome: A total of 15 paediatric patients (ages 2 months to 12 years) received SOLIRIS in aHUS Study C09-001r. Forty seven percent of patients had an identified complement regulatory factor mutation or auto-antibody. The median time from aHUS diagnosis to first dose of SOLIRIS was 14 months (range < 1 to 110 months). The median time from current thrombotic microangiopathy manifestation to first dose of SOLIRIS was 1 month (range < 1 to 16 months). The median duration of SOLIRIS therapy was 16 weeks (range 4 to 70 weeks) for children under 2 years of age (n = 5) and 31 weeks (range 19 to 63 weeks) for children 2 years to less than 12 years of age (n = 10).
Overall, the efficacy results of these paediatric patients appeared consistent with what was observed in patients enrolled in aHUS pivotal Studies C08-002 and C08-003 (Table 5). No paediatric patient required new dialysis during treatment with SOLIRIS. (See Table 9.)
 Click on icon to see table/diagram/image
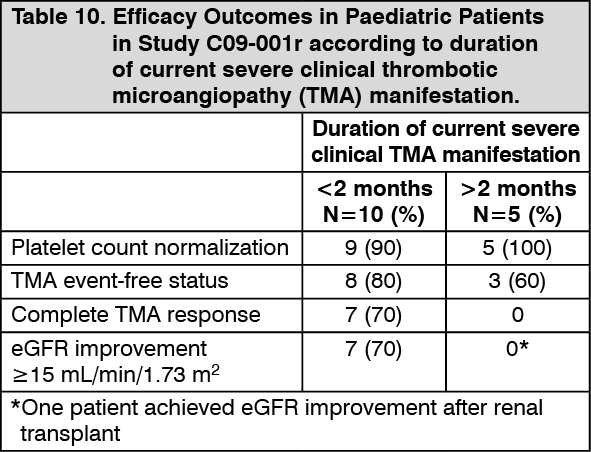
Click on icon to see table/diagram/imageIn paediatric patients with shorter duration of current severe clinical thrombotic microangiopathy (TMA) manifestation prior to eculizumab, there was TMA control and improvement of renal function with eculizumab treatment (Table 9).
In paediatric patients with longer duration of current severe clinical TMA manifestation prior to eculizumab, there was TMA control with eculizumab treatment. However, renal function was not changed due to prior irreversible kidney damage (see Table 10).
 Click on icon to see table/diagram/image
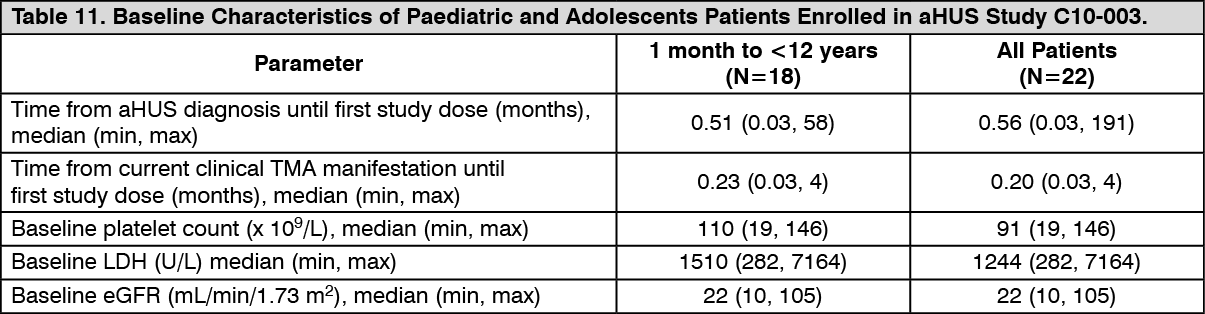
Click on icon to see table/diagram/imageA total of 22 paediatric and adolescents patients (aged 5 months to 17 years) received SOLIRIS in aHUS Study C10-003.
In Study C10-003, patients who enrolled in the study were required to have a platelet count < lower limit of normal range (LLN), evidence of haemolysis such as an elevation in serum LDH above the upper limits of normal and serum creatinine level ≥97 percentile for age without the need for chronic dialysis. The median patient age was 6.5 years (range: 5 months to 17 years). Patients enrolled in aHUS C10-003 had an ADAMTS-13 level above 5%. Fifty percent of patients had an identified complement regulatory factor mutation or auto-antibody. A total of 10 patients received PE/PI prior to eculizumab. Table 11 summarizes the key baseline clinical and disease-related characteristics of patients enrolled in aHUS Study C10-003. (See Table 11.)
 Click on icon to see table/diagram/image
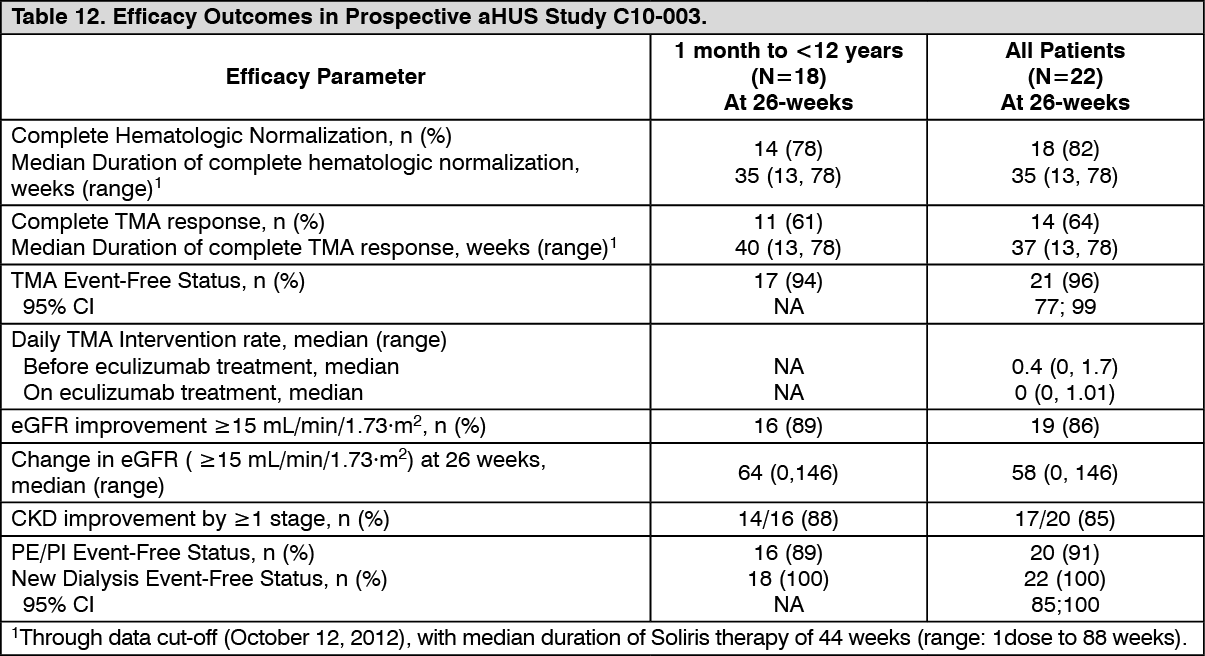
Click on icon to see table/diagram/imagePatients in aHUS C10-003 received SOLIRIS for a minimum of 26 weeks. After completion of the initial 26-week treatment period, most patients elected to continue on chronic dosing. Reduction in terminal complement activity was observed in all patients after commencement of SOLIRIS. SOLIRIS reduced signs of complement-mediated TMA activity, as shown by an increase in mean platelet counts from baseline to 26 weeks. The mean (±SD) platelet count increased from 88 ± 42 x109/L at baseline to 281 ± 123 x109/L by one week; this effect was maintained through 26 weeks (mean platelet count (±SD) at week 26: 293 ± 106 x109/L). Renal function, as measured by eGFR, was improved during SOLIRIS therapy. Nine of the 11 patients who required dialysis at baseline no longer required dialysis after Study Day 15 of eculizumab treatment. Responses were similar across all ages from 5 months to 17 years of age. In aHUS C10-003, responses to SOLIRIS were similar in patients with and without identified mutations in genes encoding complement regulatory factor proteins or auto-antibodies to factor H.
Table 12 summarizes the efficacy results for aHUS C10-003. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLonger term treatment with SOLIRIS (median 55 weeks ranging from 1day to 107 weeks) was associated with an increased rate of clinically meaningful improvements in paediatric and adolescent patients with aHUS. When SOLIRIS treatment was continued for more than 26 weeks, one additional patient (68% of patients in total) achieved Complete TMA Response and two additional patients (91% of patients in total) achieved hematologic normalization. At the last evaluation, 19 of 22 patients (86%) achieved eGFR improvement of ≥ 15 ml/min/1.73 m2 from baseline. No patient required new dialysis with SOLIRIS.
Pharmacokinetics: Pharmacokinetics and Drug Metabolism: Biotransformation: Human antibodies undergo endocytotic digestion in the cells of the reticuloendothelial system. Eculizumab contains only naturally occurring amino acids and has no known active metabolites. Human antibodies are predominately catabolized by lysosomal enzymes to small peptides and amino acids.
Elimination: No specific studies have been performed to evaluate the hepatic, renal, lung, or gastrointestinal routes of excretion/elimination for SOLIRIS. In normal kidneys, antibodies are not excreted and are excluded from filtration by their size.
Pharmacokinetic Parameters: In 40 patients with PNH, a 1-compartmental model was used to estimate pharmacokinetic parameters after multiple doses. Mean clearance was 0.31 ± 0.12 ml/hr/kg, mean volume of distribution was 110.3 ± 17.9 ml/kg, and mean elimination half-life was 11.3 ± 3.4 days. Based on these data, the onset of steady state is predicted to be approximately 49 - 56 days.
In PNH patients, pharmacodynamic activity correlates directly with eculizumab serum concentrations and maintenance of trough levels above ≥ 35 microgram/ml results in essentially complete blockade of haemolytic activity in the majority of PNH patients.
A second population PK analysis with a standard 1 compartmental model was conducted on the multiple dose PK data from 37 aHUS patients receiving the recommended SOLIRIS regimen in studies C08-002A/B and C08-003A/B. In this model, the clearance of SOLIRIS for a typical aHUS patient weighing 70 kg was 0.0139 L/hr and the volume of distribution was 5.6 L. The elimination half-life was 297 h (approximately 12.4 days).
The second population PK model was applied to the multiple dose PK data from 22 paediatric aHUS patients receiving the recommended SOLIRIS regimen in aHUS C10-003. The clearance and volume of distribution of SOLIRIS are weight dependent, which forms the basis for a weight categorical based dose regimen in paediatric patients (see Dosage & Administration). Clearance values of SOLIRIS in paediatric aHUS patients were 10.4, 5.3, and 2.2 ml/hr with body weight of 70, 30, and 10 kg, respectively; and the corresponding volume of distribution values were 5.23, 2.76, and 1.21 L, respectively. The corresponding elimination half-life remained almost unchanged within a range of 349 to 378 h (approximately 14.5 to 15.8 days).
The clearance and half-life of eculizumab were also evaluated during plasma exchange interventions. Plasma exchange resulted in an approximately 50% decline in eculizumab concentrations following a 1-hour intervention and the elimination half-life of eculizumab was reduced to 1.3 hours. Supplemental dosing is recommended when SOLIRIS is administered to aHUS patients receiving plasma infusion or exchange (see Dosage & Administration).
All aHUS patients treated with SOLIRIS when administered as recommended demonstrated rapid and sustained reduction in terminal complement activity. In aHUS patients, pharmacodynamic activity correlates directly with eculizumab serum concentrations and maintenance of trough levels of approximately 50-100 microgram/ml result in essentially complete blockade of terminal complement activity in all aHUS patients.
Special Populations: PNH: Dedicated studies have not been conducted to evaluate the pharmacokinetics of SOLIRIS administration in special PNH patient populations identified by gender, race, age (geriatric), or the presence of renal or hepatic impairment.
Paediatric population: The pharmacokinetics of eculizumab was evaluated in Study M07-005 including 7 PNH paediatric patients (aged from 11 to less than 18 years).
Weight was a significant covariate resulting in a lower eculizumab clearance 0.0105 L/h in the adolescent patients. Dosing for paediatric patients <40 kg is based on paediatric patients with aHUS.
aHUS: The pharmacokinetics of SOLIRIS have been studied in aHUS patients with a range of renal impairment and age. There have been no observed differences in PK parameters noted in these subpopulations of aHUS patients.
Toxicology: Preclinical safety data: The specificity of eculizumab for C5 in human serum was evaluated in two in vitro studies.
The tissue cross-reactivity of eculizumab was evaluated by assessing binding to a panel of 38 human tissues. C5 expression in the human tissue panel examined in this study is consistent with published reports of C5 expression, as C5 has been reported in smooth muscle, striated muscle, and renal proximal tubular epithelium. No unexpected tissue cross-reactivity was observed.
Animal reproduction studies have not been conducted with eculizumab due to lack of pharmacologic activity in non-human species.
In a 26-week toxicity study performed in mice with a surrogate antibody directed against murine C5, treatment did not affect any of the toxicity parameters examined. Haemolytic activity during the course of the study was effectively blocked in both female and male mice.
No clear treatment-related effects or adverse effects were observed in reproductive toxicology studies in mice with a surrogate terminal complement inhibitory antibody, which was utilized to assess the reproductive safety of C5 blockade. These studies included assessment of fertility and early embryonic development, developmental toxicity, and pre- and post-natal development.
When maternal exposure to the antibody occurred during organogenesis, two cases of retinal dysplasia and one case of umbilical hernia were observed among 230 offspring born to mothers exposed to the higher antibody dose (approximately 4 times the maximum recommended human SOLIRIS dose, based on a body weight comparison); however, the exposure did not increase foetal loss or neonatal death.
No animal studies have been conducted to evaluate the genotoxic and carcinogenic potential of eculizumab or its effect on fertility.