


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Interferons (IFNs) are a group of endogenous glycoproteins endowed with immunomodulatory, antiviral and antiproliferative properties.
Rebif (interferon beta-1a) shares the same amino acid sequence with endogenous human interferon beta. It is produced in mammalian cells (Chinese hamster ovary) and is therefore glycosylated like the natural protein.
Regardless of the route of dosing, pronounced pharmacodynamic changes are associated with the administration of Rebif. After a single dose, intracellular and serum activity of 2‑5A synthetase and serum concentrations of beta‑2 microglobulin and neopterin increase within 24 hours, and start to decline within 2 days. Intramuscular and subcutaneous administrations produce fully superimposable responses. After repeated subcutaneous administration every 48 hours for 4 doses, these biological responses remain elevated, with no signs of tolerance development.
Biological response markers (e.g., 2',5'-OAS activity, neopterin and beta 2-microglobulin) are induced by interferon beta-1a following subcutaneous doses administered to healthy volunteer subjects. Time to peak concentrations following a single subcutaneous injection were 24 to 48 hours for neopterin, beta-2-microglobulin and 2'5'OAS, 12 hours for MX1 and 24 hours for OAS1 and OAS2 gene expression. Peaks of similar height and time were observed for most of these markers after first and sixth administration.
The precise mechanism of action of Rebif in multiple sclerosis is still under investigation.
Relapsing-remitting multiple sclerosis: The safety and efficacy of Rebif has been evaluated in patients with relapsing-remitting multiple sclerosis at doses ranging from 11 to 44 micrograms (3-12 million IU), administered subcutaneously three times per week. At licensed posology, Rebif 22 micrograms has been demonstrated to decrease the incidence (approximately 30% over 2 years) and severity of clinical relapses in patients with at least 2 exacerbations in the previous 2 years and with an EDSS of 0-5.0 at entry. The proportion of patients with disability progression, as defined by at least one point increase in EDSS confirmed three months later, was reduced from 39% (placebo) to 30% (Rebif 22 micrograms). Over 4 years, the reduction in the mean exacerbation rate was 22% in patients treated with Rebif 22 micrograms, and 29% in patients treated with Rebif 44 micrograms group compared with a group of patients treated with placebo for 2 years and then either Rebif 22 or Rebif 44 micrograms for 2 years.
Secondary progressive multiple sclerosis: In a 3-year study in patients with secondary progressive multiple sclerosis (EDSS 3-6.5) with evidence of clinical progression in the preceding two years and who had not experienced relapses in the preceding 8 weeks, Rebif had no significant effect on progression of disability, but relapse rate was reduced by approximately 30%. If the patient population was divided into 2 subgroups (those with and those without relapses in the 2-year period prior to study entry), there was no effect on disability in patients without relapses, but in patients with relapses, the proportion with progression in disability at the end of the study was reduced from 70% (placebo) to 57% (Rebif 22 micrograms and 44 micrograms combined).
These results obtained in a subgroup of patients a posteriori should be interpreted cautiously.
Primary progressive multiple sclerosis: Rebif has not yet been investigated in patients with primary progressive multiple sclerosis, and should not be used in such patients.
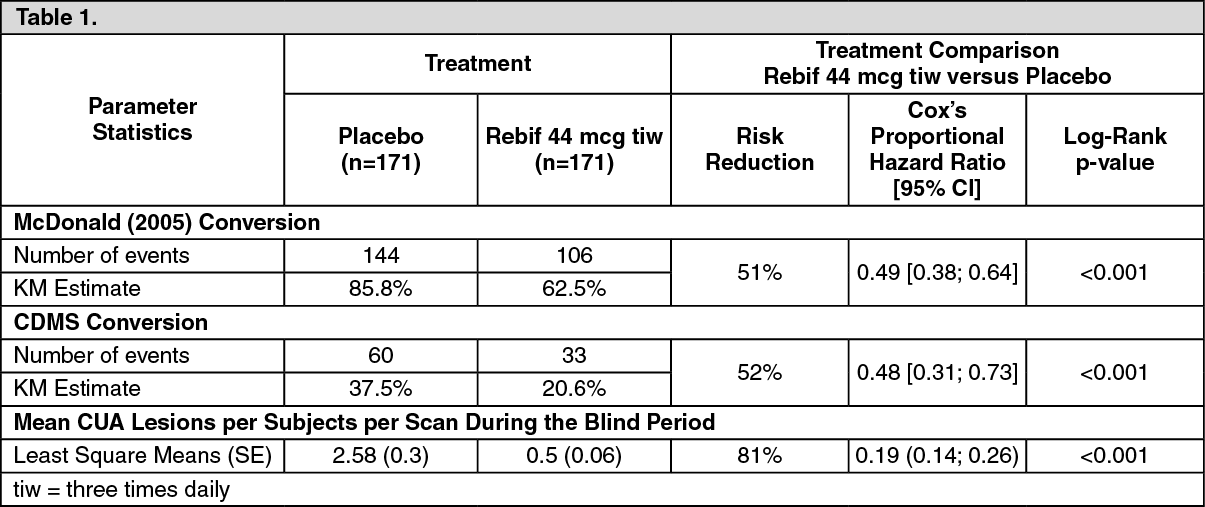
44mcg: Single clinical event suggestive of multiple sclerosis: One 2-year controlled clinical trial with Rebif was performed in patients with a single clinical event suggestive of demyelination due to multiple sclerosis. The patients enrolled into the trial had at least two clinically silent lesions on the T2-weighted MRI scan, with a size of at least 3 mm, at least one of which is ovoid or periventricular or infratentorial. Any disease other than multiple sclerosis that could better explain signs and symptoms of the patient had to be excluded.
Patients were randomised in a double-blind manner to either Rebif 44 micrograms given three times per week, Rebif 44 micrograms once weekly, or placebo. If a second clinical demyelinating event occurred confirming definite multiple sclerosis, patients switched to the recommended posology of Rebif 44 micrograms three times per week in an open label manner, while maintaining blinding as to initial randomisation. Efficacy results of Rebif 44 micrograms given three times per week compared to placebo from this study are as follows: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor the time being there is no well established definition of a high risk patient, although a more conservative approach is to accept at least nine T2 hyperintense lesions on the initial scan and at least one new T2 or one new Gd-enhancing lesion on a follow-up scan taken at least 1 month after the initial scan. In any case, treatment should only be considered for patients classified as high risk.
Pharmacokinetics: Absorption: In healthy volunteers after intravenous administration, interferon beta‑1a exhibits a sharp multi‑exponential decline, with serum levels proportional to the dose. The initial half‑life is in the order of minutes and the terminal half‑life is several hours.
When administered by the subcutaneous or intramuscular routes, serum levels of interferon beta remain low, but are still measurable up to 12 to 24 hours post‑dose. Subcutaneous and intramuscular administrations of Rebif produce equivalent exposure to interferon beta.
Distribution: Following repeated subcutaneous injections of 22 and 44 micrograms doses of Rebif maximum concentrations were typically observed after 8 hours, but this was highly variable.
Elimination: After repeated subcutaneous doses in healthy volunteers, the main PK parameters (AUCtau and Cmax) increased proportional to the increased in dose from 22 micrograms to 44 micrograms. The estimated apparent half-life is 50 to 60 hours, which is in line with the accumulation observed after multiple dosing.
Metabolism: Interferon beta‑1a is mainly metabolised and excreted by the liver and the kidneys.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated-dose toxicity, and genotoxicity.
Rebif has not been investigated for carcinogenicity.
A study on embryo/foetal toxicity in monkeys showed no evidence of reproductive disturbances.
An increased risk of abortions has been reported in animal studies of other alpha and beta interferons. No information is available on the effects of the interferon beta-1a on male fertility.