


 Sign Out
Sign Out


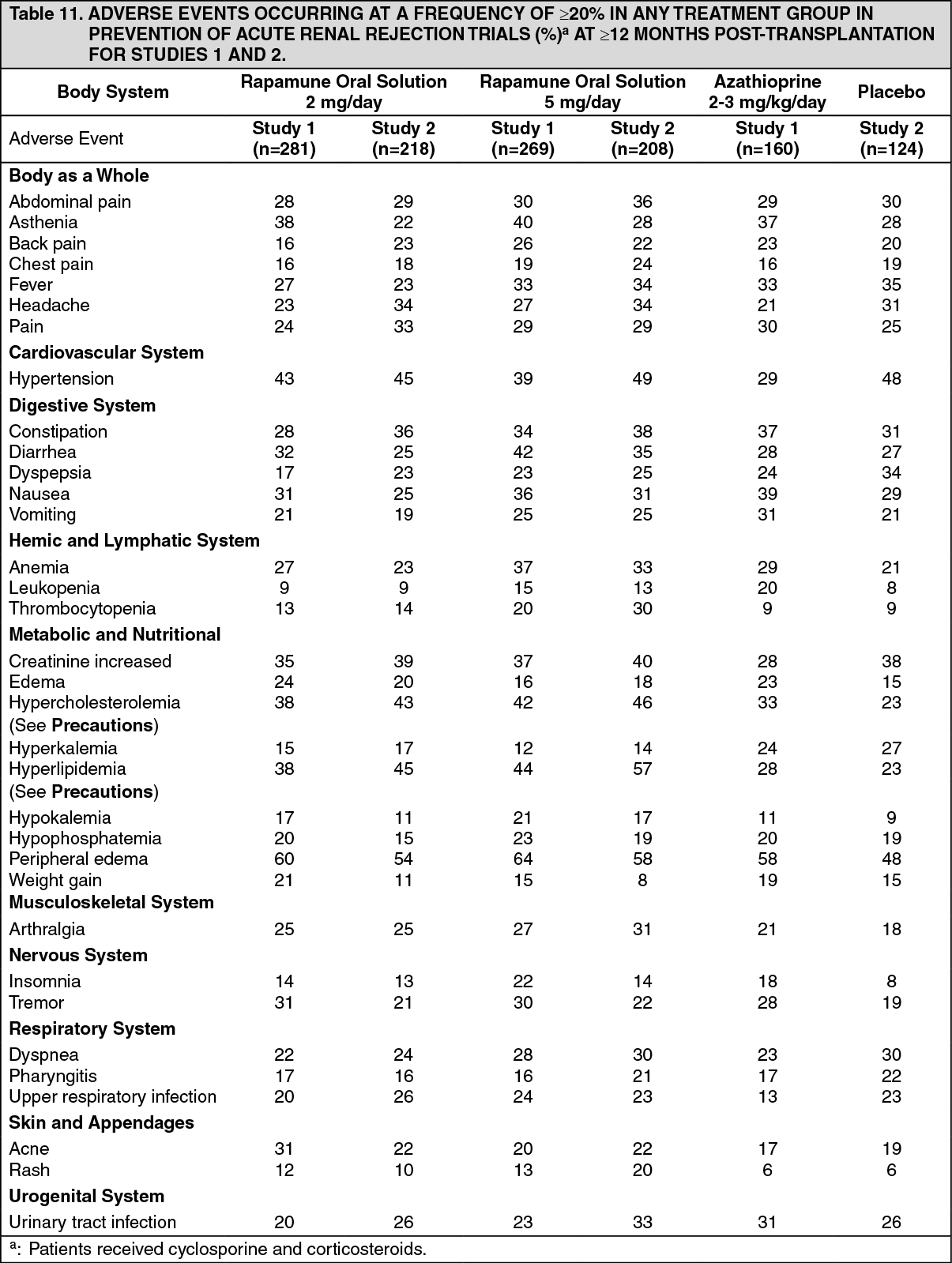
Specific adverse reactions associated with the administration of Rapamune Oral Solution occurred at a significantly higher frequency than in the respective control group. For both Rapamune Oral Solution 2 mg/day and 5 mg/day these include hypercholesterolemia, hyperlipemia, hypertension, and rash; for Rapamune Oral Solution 2 mg/day acne; and for Rapamune Oral Solution 5 mg/day anemia, arthralgia, diarrhea, hypokalemia, and thrombocytopenia. The elevations of triglycerides and cholesterol and decreases in platelets and hemoglobin occurred in a dose-related manner in patients receiving Rapamune.
Patients maintained on Rapamune Oral Solution 5 mg/day, when compared with patients on Rapamune Oral Solution 2 mg/day, demonstrated an increased incidence of the following adverse events: anemia, leukopenia, thrombocytopenia, hypokalemia, hyperlipemia, fever, and diarrhea.
In general, adverse events related to the administration of Rapamune were dependent on dose/concentration. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAt 12 months, there were no significant differences in incidence rates for clinically important opportunistic or common transplant-related infections across treatment groups, with the exception of mucosal infections with Herpes simplex, which occurred at a significantly greater rate in patients treated with Rapamune 5 mg/day than in both of the comparator groups.
Among the adverse events that were reported at a rate of ≥3% and <20%, the following were more prominent in patients maintained on Rapamune 5 mg/day, when compared to patients on Rapamune 2 mg/day; epistaxis, lymphocele, insomnia, thrombotic thrombocytopenic purpura (hemolytic-uremic syndrome), skin ulcer, increased LDH, hypotension, facial edema.
The frequency of adverse reactions listed in the following table includes reactions reported in patients treated with Rapamune-based regimens.
In general, adverse events related to administration of Rapamune were dependent on dose/concentration.
The adverse reactions in the table as follows are listed in the MedDRA frequency categories. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRapamune following cyclosporine withdrawal: The incidence of adverse reactions was determined through 60 months in a randomized, multicenter controlled trial in which 215 renal transplant patients received Rapamune as a maintenance regimen following cyclosporine withdrawal, and 215 patients received Rapamune with cyclosporine therapy. All patients were treated with corticosteroids. The safety profile prior to randomization (start of cyclosporine withdrawal) was similar to that of the 2-mg Rapamune groups in studies of Rapamune in combination with cyclosporine. Following randomization (at 3 months), patients who had cyclosporine eliminated from their therapy experienced significantly higher incidences of increased AST/SGOT and increased ALT/SGPT, liver damage, hypokalemia, thrombocytopenia, abnormal healing, acne, ileus, and joint disorder. Conversely, the incidence of acidosis, hypertension, cyclosporine toxicity, increased creatinine, abnormal kidney function, toxic nephropathy, edema, hyperuricemia, gout, and gum hyperplasia was significantly higher in patients who remained on cyclosporine than those who had cyclosporine withdrawn from therapy. Mean systolic and diastolic blood pressure improved significantly following cyclosporine withdrawal.
Following cyclosporine withdrawal, (at 60 months), the incidence of Herpes zoster infection was significantly lower in patients receiving Rapamune following cyclosporine withdrawal, compared with patients who continued to receive Rapamune and cyclosporine.
The incidence of malignancies following cyclosporine withdrawal, based upon distinct categories, is presented in the following table. The incidence of lymphoma/lymphoproliferative disease was similar in all treatment groups. The overall incidence of malignancy, based upon the number of patients who had one or more malignancy, was lower in patients who had cyclosporine withdrawn than in patients receiving Rapamune plus cyclosporine (10.7% versus 15.8%, respectively). (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBy 60 months, the incidence of non-skin malignancies (lymphoma/lymphoproliferative disease plus other malignancy from the previous table) was significantly higher in the cohort who continued cyclosporine as compared with the cohort who had cyclosporine withdrawn (8.4% versus 3.8%, respectively). For skin cancer, the median time to first occurrence was significantly delayed (491 versus 1126 days) and when taking into account that a patient may have multiple skin cancers the relative risk (RR = 0.346) for developing skin cancer was significantly lowered in the cyclosporine withdrawal group as compared with the group that continued cyclosporine.
Safety was assessed in a controlled trial (see Pharmacology: Pharmacodynamics: Clinical Trials Data on Efficacy under Actions) involving 448 patients who received at least one dose of study drug (safety population): 224 patients received at least one dose of sirolimus with tacrolimus, and 224 patients received at least one dose of sirolimus with cyclosporine. Overall, the incidence and nature of adverse events was similar to those seen in previous combination studies with Rapamune. Diarrhea and herpes simplex occurred significantly more frequently in patients who received sirolimus and tacrolimus, whereas, hypertension, cardiomegaly, lymphocele, increased creatinine, acne, urinary tract disorder, ovarian cyst, and calcineurin inhibitor toxicity occurred at a significantly higher rate in patients who received sirolimus and cyclosporine. The incidence of malignancy was low (1.3% in each group).
The safety and efficacy of conversion from calcineurin inhibitors to Rapamune in maintenance renal transplant patients has not been established.
In a study evaluating the safety and efficacy of conversion (6 to 120 months after transplantation) from calcineurin inhibitors to Rapamune (sirolimus target levels of 12-20 ng/mL by chromatographic assay) in maintenance renal transplant patients, enrollment was stopped in the subset of patients (n=90) with a baseline glomerular filtration rate of less than 40 mL/min. There was a higher rate of serious adverse events including pneumonia, acute rejection, graft loss and death in this Rapamune treatment arm (n=60, median time post-transplant 36 months).
In a study evaluating the safety and efficacy of conversion from tacrolimus to Rapamune 3 to 5 months post renal transplant, a higher rate of acute rejection and new onset diabetes mellitus was observed following conversion to Rapamune (see Pharmacology: Pharmacodynamics: Clinical Trials Data on Efficacy under Actions).
The concomitant use of sirolimus with a calcineurin inhibitor may increase the risk of calcineurin inhibitor-induced HUS/TTP/TMA (see Precautions).
In patients with delayed graft function, Rapamune may delay recovery of renal function (see Renal Function under Precautions).
Other Clinical Experience: Azoospermia has been reported with the use of Rapamune and has been reversible upon discontinuation of Rapamune in most cases (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Clostridium difficile enterocolitis has been reported in patients receiving sirolimus.
Interstitial Lung Disease: Cases of interstitial lung disease [including pneumonitis, and infrequently bronchiolitis obliterans organizing pneumonia (BOOP) and pulmonary fibrosis], some fatal, with no identified infectious etiology have occurred in patients receiving immunosuppressive regimens including Rapamune. In some cases, the interstitial lung disease has resolved upon discontinuation or dose reduction of Rapamune. The risk may be increased as the trough sirolimus level increases. (See Interstitial Lung Disease under Precautions.)
Latent Viral Infections: BK virus associated nephropathy and progressive multifocal leukoencephalopathy (PML) have been observed in patients receiving immunosuppressants, including Rapamune. These infection may be associated with serious or fatal outcomes, including renal graft loss (see Latent Viral Infections under Precautions).
Hepatotoxicity: Hepatotoxicity has been reported, including fatal hepatic necrosis with elevated trough sirolimus levels (i.e., exceeding therapeutic levels).
Abnormal Healing: Abnormal healing following transplant surgery has been reported, including fascial dehiscence, incisional hernia and anastomosis disruption (e.g., wound, vascular, airway, ureteral, biliary).
View ADR Monitoring Form