Pharmacology: PUMPITOR contains Omeprazole, a new class of antisecretory compounds, the substituted benzimidazole, which suppress gastric acid secretion by specific inhibition of H
+/K
+ ATPase enzyme system at the secretory surface of the gastric parietal cells.
Because this enzyme system is regarded as the acid (proton) pump within the gastric mucosa, Omeprazole has been characterized as a gastric acid-pump inhibitor, in that it blocks the final step of acid production. This effect is dose-related and leads to inhibition of both basal and stimulated acid secretion irrespective of the stimulus.
PUMPITOR does not exhibit anticholinergic or H
2 histamine antagonistic properties. Animal studies indicate that after rapid disappearance from plasma, Omeprazole can be found within the gastric mucosa for a day or more.
Antisecretory Activity: After oral administration, the onset of the antisecretory effect of Omeprazole occurs within one hour, with the maximum effect occurring within 2 hours. Inhibition of secretion is about 50% of the maximum at 24 hours and the duration of inhibition lasts up to 72 hours.
The antisecretory effect of Omeprazole thus lasts for longer than would be expected from the very short plasma half-life (less than one hour), apparently due to prolonged binding of the parietal H
+/K
+ ATPase enzyme.
When the drug is discontinued, secretory activity returns gradually over 3 to 5 days. The inhibitory effect on acid secretion increases with repeated once-daily dosing, reaching the maximum effect after 4 days.
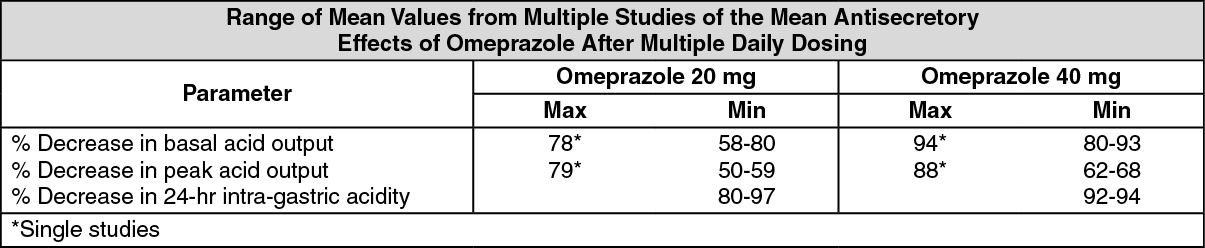
Results from numerous studies of the antisecretory effect of multiple doses of 20 mg and 40 mg of Omeprazole in normal volunteers and patients are shown below. The "max" value represents determinations at a time of maximum effect (2-6 hours after dosing), while "min" values are those 24 hours after the last dose of Omeprazole. (See table).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
PUMPITOR is rapidly absorbed and peak plasma level occurring within 0.5 hours to 3.5 hours.
Absolute bioavailability is about 30% - 40% at doses of 20-40 mg, due in large part to presystemic metabolism. Plasma half-life occurs within 0.5 to 1 hour and the total body clearance is 500-600 mL/minute.
Approximately 95% of Omeprazole is bound to protein plasma.
The bioavailability of Omeprazole increases slightly upon repeated administration.
Little if any unchanged drug was excreted in urine. About 77% was eliminated in urine as at least six metabolites, the remainder of the dose was recoverable in the feces.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
