


 Sign Out
Sign Out



Lactic acidosis and severe hepatomegaly with steatosis [see Warnings and Lactic Acidosis and Severe Hepatomegaly with Steatosis under Precautions].
Clinical Trial Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
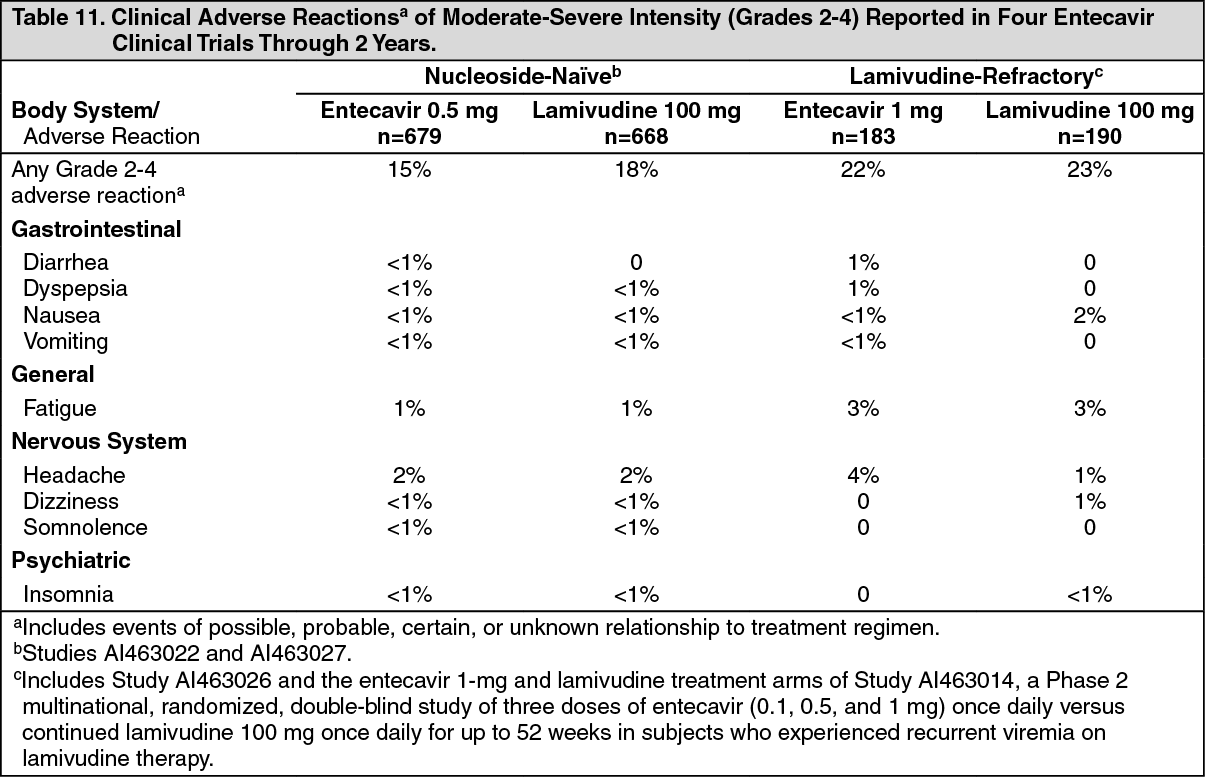
Compensated Liver Disease: Assessment of adverse reactions is based on four studies (AI463014, AI463022, AI463026, and AI463027) in which 1720 subjects with chronic hepatitis B virus infection and compensated liver disease received double-blind treatment with entecavir 0.5 mg/day (n=679), 1 mg/day (n=183), or lamivudine (n=858) for up to 2 years. Median duration of therapy was 69 weeks for entecavir-treated subjects and 63 weeks for lamivudine-treated subjects in Studies AI463022 and AI463027 and 73 weeks for entecavir-treated subjects and 51 weeks for lamivudine-treated subjects in Studies AI463026 and AI463014. The safety profiles of entecavir and lamivudine were comparable in these studies. The most common adverse reactions of any severity (≥3%) with at least a possible relation to study drug for entecavir-treated subjects were headache, fatigue, dizziness, and nausea. The most common adverse reactions among lamivudine-treated subjects were headache, fatigue, and dizziness. One percent of entecavir-treated subjects in these four studies compared with 4% of lamivudine-treated subjects discontinued for adverse events or abnormal laboratory test results.
Clinical adverse reactions of moderate-severe intensity and considered at least possibly related to treatment occurring during therapy in four clinical studies in which entecavir was compared with lamivudine are presented in Table 11. (See Table 11.)
 Click on icon to see table/diagram/image
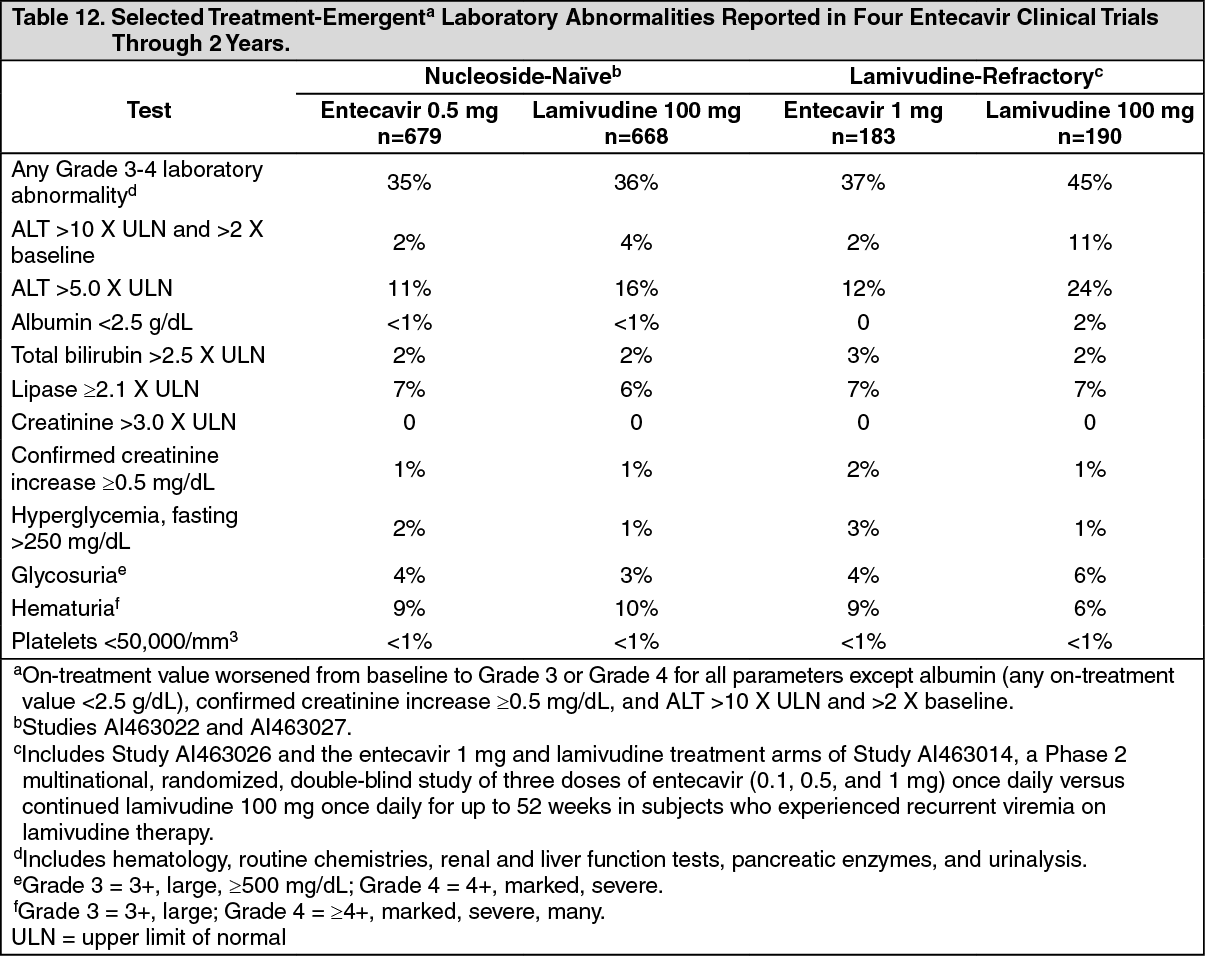
Click on icon to see table/diagram/imageLaboratory Abnormalities: Frequencies of selected treatment-emergent laboratory abnormalities reported during therapy in four clinical trials of entecavir compared with lamivudine are listed in Table 12. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAmong entecavir-treated subjects in these studies, on-treatment ALT elevations greater than 10 times the upper limit of normal (ULN) and greater than 2 times baseline generally resolved with continued treatment. A majority of these exacerbations were associated with a ≥2 log10/mL reduction in viral load that preceded or coincided with the ALT elevation. Periodic monitoring of hepatic function is recommended during treatment.
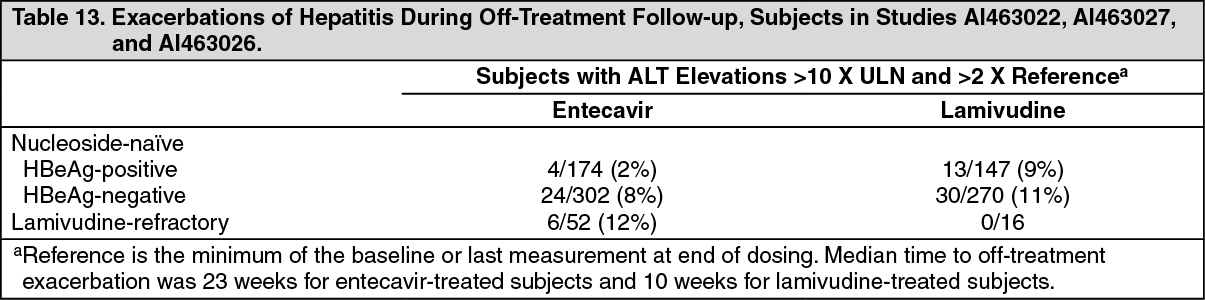
Exacerbations of Hepatitis after Discontinuation of Treatment: An exacerbation of hepatitis or ALT flare was defined as ALT greater than 10 times the upper limit of normal (ULN) and greater than 2 times the subject's reference level (minimum of the baseline or last measurement at end of dosing). For all subjects who discontinued treatment (regardless of reason), Table 13 presents the proportion of subjects in each study who experienced post-treatment ALT flares. In these studies, a subset of subjects was allowed to discontinue treatment at or after 52 weeks if they achieved a protocol-defined response to therapy. If entecavir is discontinued without regard to treatment response, the rate of post-treatment flares could be higher [see Severe Acute Exacerbations of Hepatitis B under Precautions]. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDecompensated Liver Disease: Study AI463048 was a randomized, open-label study of entecavir 1 mg once daily versus adefovir dipivoxil 10 mg once daily given for up to 48 weeks in adult subjects with chronic HBV infection and evidence of hepatic decompensation, defined as a Child-Turcotte-Pugh (CTP) score of 7 or higher [see Pharmacology: Pharmacodynamics: Clinical Studies: Outcomes at 48 Weeks under Actions]. Among the 102 subjects receiving entecavir, the most common treatment-emergent adverse events of any severity, regardless of causality, occurring through Week 48 were peripheral edema (16%), ascites (15%), pyrexia (14%), hepatic encephalopathy (10%), and upper respiratory infection (10%). Clinical adverse reactions not listed in Table 11 that were observed through Week 48 include blood bicarbonate decreased (2%) and renal failure (<1%).
Eighteen of 102 (18%) subjects treated with entecavir and 18/89 (20%) subjects treated with adefovir dipivoxil died during the first 48 weeks of therapy. The majority of deaths (11 in the entecavir group and 16 in the adefovir dipivoxil group) were due to liver-related causes such as hepatic failure, hepatic encephalopathy, hepatorenal syndrome, and upper gastrointestinal hemorrhage. The rate of hepatocellular carcinoma (HCC) through Week 48 was 6% (6/102) for subjects treated with entecavir and 8% (7/89) for subjects treated with adefovir dipivoxil. Five percent of subjects in either treatment arm discontinued therapy due to an adverse event through Week 48.
No subject in either treatment arm experienced an on-treatment hepatic flare (ALT >2 X baseline and >10 X ULN) through Week 48. Eleven of 102 (11%) subjects treated with entecavir and 11/89 (13%) subjects treated with adefovir dipivoxil had a confirmed increase in serum creatinine of 0.5 mg/dL through Week 48.
HIV/HBV Co-infected: The safety profile of entecavir 1 mg (n=51) in HIV/HBV co-infected subjects enrolled in Study AI463038 was similar to that of placebo (n=17) through 24 weeks of blinded treatment and similar to that seen in non-HIV infected subjects [see Patients Co-infected with HIV and HBV under Precautions].
Liver Transplant Recipients: Among 65 subjects receiving entecavir in an open-label, post-liver transplant trial [see Use in Specific Populations: Liver Transplant Recipients under Precautions], the frequency and nature of adverse events were consistent with those expected in patients who have received a liver transplant and the known safety profile of entecavir.
Postmarketing Experience: Data from Long-Term Observational Study: Study AI463080 was a randomized, global, observational, open-label Phase 4 study to assess long-term risks and benefits of entecavir (0.5 mg/day or 1 mg/day) treatment as compared to other standard-of-care HBV nucleos(t)ide analogues in subjects with chronic HBV infection.
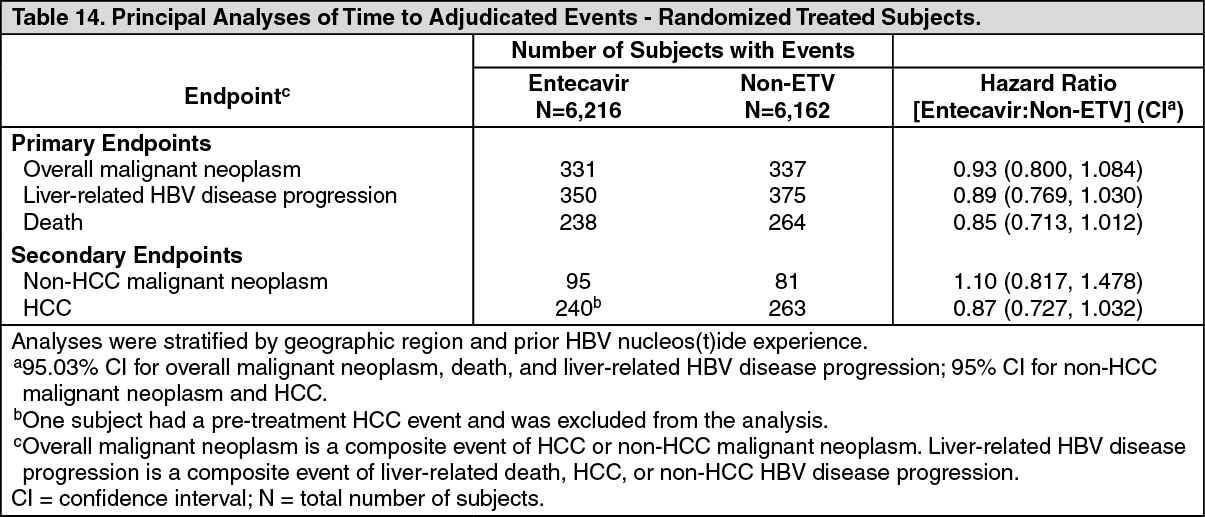
A total of 12,378 patients were treated with entecavir (n=6,216) or other HBV nucleos(t)ide treatment [non-entecavir (ETV)] (n=6,162). Patients were evaluated at baseline and subsequently every 6 months for up to 10 years. The principal clinical outcome events assessed during the study were overall malignant neoplasms, liver-related HBV disease progression, HCC, non-HCC malignant neoplasms, and death. The study showed that entecavir was not significantly associated with an increased risk of malignant neoplasms compared to other standard-of-care HBV nucleos(t)ides, as assessed by either the composite endpoint of overall malignant neoplasms or the individual endpoint of non-HCC malignant neoplasms. The most commonly reported malignancy in both the entecavir and non-ETV groups was HCC followed by gastrointestinal malignancies. The data also showed that long-term entecavir use was not associated with a lower occurrence of HBV disease progression or a lower rate of death overall compared to other HBV nucleos(t)ides. The principal clinical outcome event assessments are shown in Table 14. (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLimitations of the study included population changes over the long-term follow-up period and more frequent post-randomization treatment changes in the non-ETV group. In addition, the study was underpowered to demonstrate a difference in the non-HCC malignancy rate because of the lower than expected background rate.
Adverse Reactions from Postmarketing Spontaneous Reports: The following adverse reactions have been reported during postmarketing use of entecavir. Because these reactions were reported voluntarily from a population of unknown size, it is not possible to reliably estimate their frequency or establish a causal relationship to entecavir exposure.
Immune system disorders: anaphylactoid reaction.
Metabolism and nutrition disorders: lactic acidosis.
Hepatobiliary disorders: increased transaminases.
Skin and subcutaneous tissue disorders: alopecia, rash.
View ADR Monitoring Form