ATC code: A02BC04.
Pharmacology: Pharmacodynamics: Mechanism of Action: Rabeprazole sodium belongs to the class of anti-secretory compounds, the substituted benzimidazoles, that do not exhibit anticholinergic or H
2 histamine antagonist properties, but suppress gastric acid secretion by the specific inhibition of the H
+/K
+-ATPase enzyme (the acid or proton pump). The effect is dose-related and leads to inhibition of both basal and stimulated acid secretion irrespective of the stimulus. Animal studies indicate that after administration, rabeprazole sodium rapidly disappears from both the plasma and gastric mucosa. As a weak base, rabeprazole is rapidly absorbed following all doses and is concentrated in the acid environment of the parietal cells. Rabeprazole is converted to the active sulphenamide form through protonation and it subsequently reacts with the available cysteines on the proton pump.
Anti-secretory Activity: After oral administration of a 20 mg dose of rabeprazole sodium the onset of the antisecretory effect occurs within one hour, with the maximum effect occurring within two to four hours. Inhibition of basal and food stimulated acid secretion 23 hours after the first dose of sodium rabeprazole are 69% and 82% respectively and the duration of inhibition lasts up to 48 hours. The inhibitory effect of sodium rabeprazole on acid secretion increases slightly with repeated once-daily dosing, achieving steady state inhibition after three days. When the drug is discontinued, secretory activity normalizes over 2 to 3 days.
Decreased gastric acidity due to any means, including proton pump inhibitors such as rabeprazole, increases counts of bacteria normally present in the gastrointestinal tract. Treatment with proton pump inhibitors may possibly increase the risk of gastrointestinal infections such as Salmonella, Campylobacter and Clostridium difficile.
Intragastric pH Effects: Administration of PARIET at 5, 10 and 20 mg once a day all resulted in a significantly increased intragastric pH in healthy adult men. The proportion of time that showed a pH of 4 or above in the period of 24 hours on day 5 of administration was 46% and 63% for EM and PM at 5 mg once a day, respectively, 58% and 72% for EM and PM at 10 mg once a day, respectively, and 61% and 76% for EM and PM at 20 mg once a day, respectively (see Pharmacology: Pharmacokinetics as follows).
Serum Gastrin Effects: In clinical studies patients were treated once daily with 10 or 20 mg rabeprazole sodium, for up to 43 months duration. Serum gastrin levels increased during the first 2 to 8 weeks reflecting the inhibitory effects on acid secretion and remained stable while treatment was continued. Gastrin values returned to pre-treatment levels, usually within 1 to 2 weeks after discontinuation of therapy.
Human gastric biopsy specimens from the antrum and the fundus from over 500 patients receiving rabeprazole or comparator treatment for up to 8 weeks have not detected changes in ECL cell histology, degree of gastritis, incidence of atrophic gastritis, intestinal metaplasia or distribution of
H. pylori infection. In over 250 patients followed for 36 months of continuous therapy, no significant change in findings present at baseline was observed.
Other Effects: Systemic effects of rabeprazole sodium in the CNS, cardiovascular and respiratory systems have not been found to date. Rabeprazole sodium, given in oral doses of 20 mg for 2 weeks, had no effect on thyroid function, carbohydrate metabolism, or circulating levels of parathyroid hormone, cortisol, estrogen, testosterone, prolactin, cholecystokinin, secretin, glucagon, follicle stimulating hormone (FSH), luteinizing hormone (LH), renin, aldosterone or somatotrophic hormone.
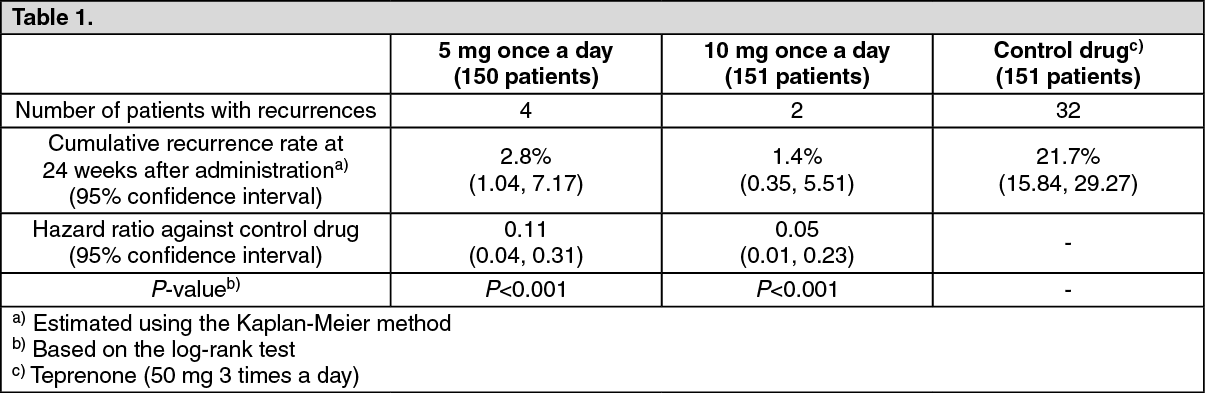
Clinical Efficacy: Prevention of gastric and duodenal ulcer recurrences associated with low-dose aspirin therapy (Study 308): The table as follows shows cumulative rates of recurrence for gastric and duodenal ulcer at 24 weeks after administration estimated using the Kaplan-Meier method in a double-blind comparative study involving patients requiring long-term treatment with low-dose aspirin (at 81 mg or 100 mg/day) with a past history of gastric ulcer or duodenal ulcer. (See Table 1 and figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Absorption:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Absorption: PARIET is an enteric-coated (gastro-resistant) tablet formulation of rabeprazole sodium. This presentation is necessary because rabeprazole is acid-labile. Absorption of rabeprazole therefore begins only after the tablet leaves the stomach. Absorption is rapid, with peak plasma levels of rabeprazole occurring approximately 3.5 hours after a 20 mg dose. Peak plasma concentrations (C
max) of rabeprazole and AUC are linear over the dose range of 10 mg to 40 mg. Absolute bioavailability of an oral 20 mg dose (compared to intravenous administration) is about 52% due in large part to pre-systemic metabolism. Additionally the bioavailability does not appear to increase with repeat administration. In healthy subjects the plasma half-life is approximately one hour (range 0.7 to 1.5 hours), and the total body clearance to be 283 ± 98 ml/min. Neither food nor the time of day of administration of the treatment affect the absorption of rabeprazole sodium.
The pharmacokinetic parameters of rabeprazole sodium (on day 5 of administration) administered repeatedly to healthy adult men in a fasting state at 5, 10 and 20 mg are shown as follows. (See Table 2.)
Click on icon to see table/diagram/image
Distribution: Rabeprazole is approximately 97% bound to human plasma proteins.
Metabolism and excretion: In humans the thioether (M1) and carboxylic acid (M6) are the main plasma metabolites with the sulphone (M2), desmethyl-thioether (M4) and mercapturic acid conjugate (M5) minor metabolites observed at lower levels. Only the desmethyl metabolite (M3) has a small amount of anti-secretory activity, but it is not present in plasma.
Following a single 20 mg
14C labeled oral dose of sodium rabeprazole, no unchanged drug was excreted in the urine. Approximately 90% of the dose was eliminated in urine mainly as the two metabolites: a mercapturic acid conjugate (M5) and a carboxylic acid (M6), plus two unknown metabolites. The remainder of the dose was recovered in feces.
Gender: Adjusted for body mass and height, there are no significant gender differences in pharmacokinetic parameters following a single 20 mg dose of rabeprazole.
Renal dysfunction: In patients with stable, end-stage, renal failure requiring maintenance hemodialysis (creatinine clearance ≤5 ml/min/1.73 m
2), the disposition of rabeprazole was very similar to that in healthy volunteers. The AUC and the C
max in these patients was about 35% lower than the corresponding parameters in healthy volunteers. The mean half-life of rabeprazole was 0.82 hours in healthy volunteers, 0.95 hours in patients during hemodialysis and 3.6 hours post dialysis. The clearance of the drug in patients with renal disease requiring maintenance hemodialysis was approximately twice that in healthy volunteers.
Hepatic dysfunction: Following a single 20 mg dose of rabeprazole to patients with chronic mild to moderate hepatic impairment the AUC doubled and there was 2-3 fold increase in half-life of rabeprazole compared to the healthy volunteers. However, following a 20 mg dose daily for 7 days the AUC had increased to only 1.5-fold and the C
max to only 1.2-fold. The half-life of rabeprazole in patients with hepatic impairment was 12.3 hours compared to 2.1 hours in healthy volunteers. The pharmacodynamic response (gastric pH control) in the two groups was clinically comparable.
Elderly: Elimination of rabeprazole was somewhat decreased in the elderly. Following 7 days of daily dosing with 20mg of rabeprazole sodium, the AUC approximately doubled, the C
max increased by 60% and t½ increased by approximately 30% as compared to young healthy volunteers. However there was no evidence of rabeprazole accumulation.
CYP2C19 Polymorphism: Following a 20mg daily dose of rabeprazole for 7 days. CYP2C19 slow metabolisers, had AUC and t½ which were approximately 1.9 and 1.6 times the corresponding parameters in extensive metabolisers whilst C
max had increased by only 40%.
Toxicology: Pre-clinical Safety Data: Pre-clinical effects were observed only at exposures sufficiently in excess of the maximum human exposure that make concerns for human safety negligible in respect of animal data.
Studies on mutagenicity gave equivocal results. Tests in mouse lymphoma cell line were positive, but
in vivo micronucleus and
in vivo and
in vitro DNA repair tests were negative. Carcinogenicity studies revealed no special hazard for humans.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image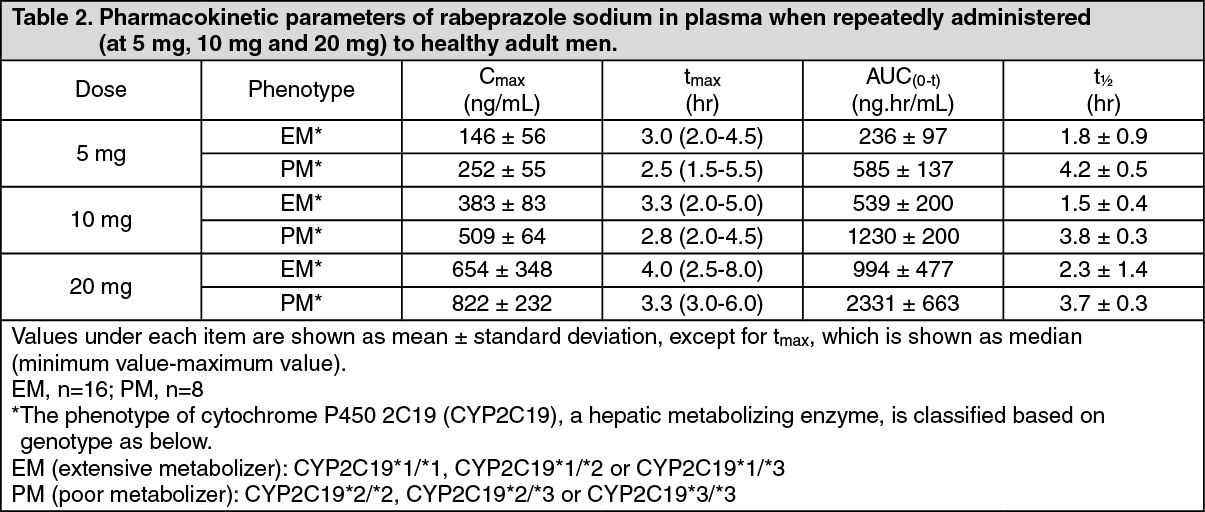 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
