


 Sign Out
Sign Out



Pharmacology: Pharmacodynamics: Mechanism of action and pharmacodynamic effects: The gadolinium chelate, gadobenate dimeglumine, shortens longitudinal (T1), and, to a lesser extent, transversal (T2) relaxation times of tissue water protons.
The relaxivities of gadobenate dimeglumine in aqueous solution are r1 = 4.39 and r2 = 5.56 mM-1s-1 at 20 MHz. Gadobenate dimeglumine experiences a strong increase in relaxivity on going from aqueous solution to solutions containing serum proteins, r1 and r2 values were 9.7 and 12.5 respectively in human plasma.
Clinical efficacy and safety: In liver imaging, MultiHance may detect lesions not visualised in pre-contrast enhanced MRI examination of patients with known or suspected hepatocellular cancer or metastatic disease. The nature of the lesions visualised after contrast enhancement with MultiHance has not been verified by pathological anatomical investigation. Furthermore, where the effect on patient management was assessed, the visualisation of post-contrast-enhanced lesions was not always associated with a change in the patient management.
In the liver MultiHance provides strong and persistent signal intensity enhancement of normal parenchyma on T1-weighted imaging. The signal intensity enhancement persists at high level for at least two hours after the administration of doses of either 0.05 or 0.10 mmol/kg. Contrast between focal liver lesions and normal parenchyma is observed almost immediately after bolus injection (up to 2-3 minutes) on T1-weighted dynamic imaging. Contrast tends to decrease at later time points because of non-specific lesion enhancement. However, progressive washout of MultiHance from the lesions and persistent signal intensity enhancement of normal parenchyma are considered to result in enhanced lesion detection and a lower detection threshold for lesion site between 40 and 120 minutes after MultiHance administration.
Data from pivotal Phase II and Phase III studies in patients with liver cancer indicate that, compared with other reference imaging modalities (e.g. intraoperative ultrasonography, computed tomographic angio-portography, CTAP, or computed tomography following intra-arterial injection of iodized oil), with MultiHance enhanced MRI scans there was a mean sensitivity of 95% and a mean specificity of 80% for detection of liver cancer or metastasis in patients with a high suspicion of these conditions.
In MRI of the brain and spine, MultiHance enhances normal tissues lacking a blood-brain barrier, extra axial tumours and regions in which the blood-brain-barrier has broken down. In the pivotal phase III clinical trials conducted in adults for this indication, designed as parallel-group comparisons, off-site readers reported an improvement in level of diagnostic information in 32-69% of images with MultiHance, and 35-69% of images with the active comparator.
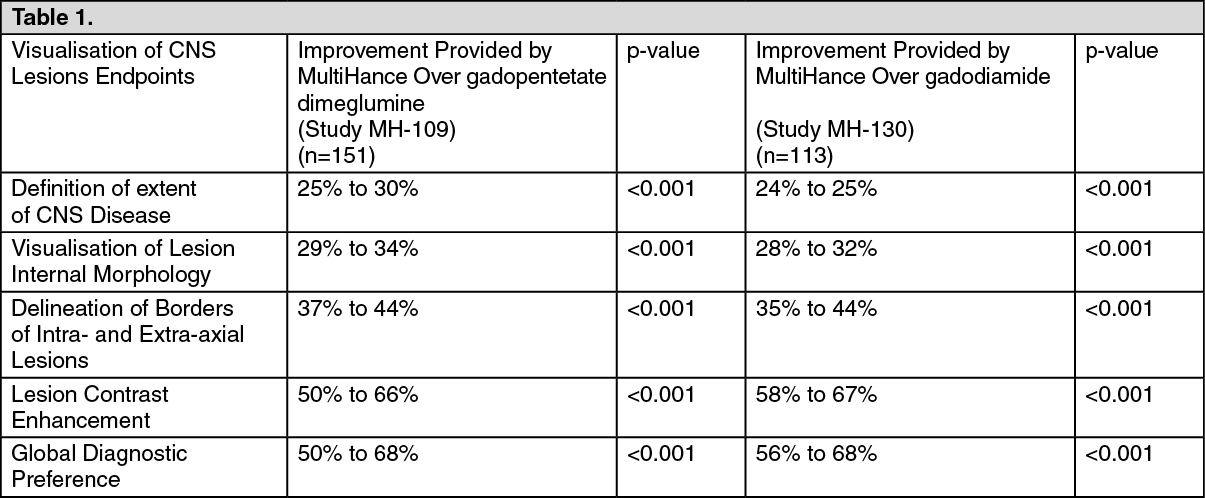
In two studies designed as intra-individual, crossover comparisons of 0.1 mmol/kg body weight MultiHance vs 0.1 mmol/kg body weight of two active comparators (gadopentetate dimeglumine or gadodiamide), conducted in patients with known or suspected brain or spine disease undergoing MRI of the central nervous system (CNS), MultiHance provided significantly (p<0.001) higher increase in lesion signal intensity, contrast-to-noise ratio, and lesion-to-brain ratio, as well as significantly (p<0.001) better visualisation of CNS lesions in images obtained with 1.5 Tesla scanners as tabulated as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the trials MH-109 and MH-130, the impact of improved visualization of CNS lesions with MultiHance versus gadodiamide or gadopentetate dimeglumine on diagnostic thinking and patient management was not studied.
In MRA, MultiHance improves image quality by increasing blood signal to noise ratio as a result of blood T1 shortening, reduces motion artifacts by shortening scan times and eliminates flow artifacts. In the phase III clinical trials in MRA of arteries extending from the supra-aortic territory to the pedal circulation, off-site readers reported an improvement in diagnostic accuracy ranging from 8% to 28% for the detection of clinically significant steno-occlusive disease (i.e. stenosis of >51% or >60% depending on the vascular territory) with MultiHance-enhanced images compared to time of flight (TOF) MRA, on the basis of conventional angiographic findings.
In MRI of female breast, MultiHance increases the contrast between neoplastic breast tissues and adjacent normal tissues, thus improving the conspicuity of breast tumors.
The pivotal, Phase III trial was an intra-individual, crossover comparison of 0.1 mmol/kg body weight MultiHance vs 0.1 mmol/kg body weight of an active, established comparator agent (gadopentetate dimeglumine) in MRI of patients with suspected or known breast cancer on the basis of previous ultrasound or mammography. The images were read off-site by three blinded readers with no affiliation to any of the study centres.
The sensitivity for the detection of benign and malignant lesions ranged from 91.7%-94.4% for MultiHance and 79.9% to 83.3% for the comparator (p<0.0003 for all readers).
The results for specificity in the detection of benign and malignant lesions were not statistically significant and ranged from 59.7%-66.7% for MultiHance and 30.6%-58.3% for the comparator (p<0.157 for all readers).
Statistically significant improvements were observed for both sensitivity and specificity in the region level analysis.
Pharmacokinetics: Modelling of the human pharmacokinetics was well described using a biexponential decay model. The apparent distribution and elimination half-times range from 0.085 to 0.117 h and from 1.17 to 1.68 respectively. The apparent total volume of distribution, ranging from 0.170 to 0.248 L/kg body weight, indicates that the compound is distributed in plasma and in the extracellular space.
Gadobenate ion is rapidly cleared from plasma and is eliminated mainly in urine and to a lesser extent in bile. Total plasma clearance, ranging from 0.098 to 0.133 L/h kg body weight, and renal clearance, ranging from 0.082 to 0.104 L/h kg body weight, indicate that the compound is predominantly eliminated by glomerular filtration. Plasma concentration and area under the curve (AUC) values show statistically significant linear dependence on the administered dose. Gadobenate ion is excreted unchanged in urine in amounts corresponding to 78%-94% of the injected dose within 24 hours. Between 2% and 4% of the dose is recovered in the faeces.
Disruption of the blood-brain barrier or abnormal vascularity allows gadobenate ion penetration into the lesion.
The current evidence suggests that gadolinium may accumulate in the brain after repeated administration of GBCAs although the exact mechanism of gadolinium passage into the brain has not been established. Population pharmacokinetic analysis was performed on systemic drug concentration-time data from 80 subjects (40 adult healthy volunteers and 40 paediatric patients) aged 2 to 47 years following intravenous administration of gadobenate dimeglumine. The kinetics of gadolinium down to the age of 2 years could be described by a two compartment model with standard allometric coefficients and a covariate effect of creatinine clearance (reflecting glomerular filtration rate) on gadolinium clearance. The pharmacokinetic parameter values (referenced to adult body weight) were consistent with previously reported values for MultiHance and consistent with the physiology presumed to underlie MultiHance distribution and elimination: distribution into extracellular fluid (approximately 15 L in an adult, or 0.21 L/kg) and elimination by glomerular filtration (approximately 130 mL plasma per minute in an adult, or 7.8 L/h and 0.11 L/h/kg). Clearance and volume of distribution decreased progressively for younger subjects due to their smaller body size. This effect could largely be accounted for by normalising pharmacokinetic parameters for body weight. Based on this analysis, weight based dosing for MultiHance in paediatric patients gives similar systemic exposure (AUC) and maximum concentration (Cmax) to those reported for adults, and confirms that no dose adjustment is necessary for the paediatric population over the proposed age range (2 years and above).
Toxicology: Preclinical safety data: Non clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential.
Indeed, preclinical effects were observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use.
Animal experiments revealed a poor local tolerance of MultiHance, especially in case of accidental paravenous application where severe local reaction, such as necrosis and eschars, could be observed. Local tolerance in case of accidental intra-arterial application has not been investigated, so that it is particularly important to ensure that the i.v. needle or cannula is correctly inserted into a vein (see Dosage & Administration).
Pregnancy and lactation: In animal studies no untoward effects on the embryonic or foetal development were exerted by daily intravenous administration of gadobenate dimeglumine in rats. Also, no adverse effects on physical and behavioural development were observed in the offspring of rats. However, after repeated daily dosing in rabbit, isolated cases of skeletal variations and two cases of visceral malformations were reported.