


 Sign Out
Sign Out



Pharmacology: Mecobalamin promotes the metabolism of nucleic acids, proteins and lipids:
In an experiment using brain-derived cell strains obtained from albino rats, mecobalamin acted as a co-enzyme in methionine synthesis. In particular, it was found to be involved in the synthesis of thymidine from deoxyuridine and to accelerate the synthesis of DNA and RNA. In another experiment using glia cells, mecobalamin was found to accelerate the synthesis of lecithin, a major component of the myelin sheath.
Mecobalamin is efficiently transferred to nervous tissues and improves metabolic disorders:
Mecobalamin is a CH3-vitamin B12 which is found in high concentrations in blood and cerebrospinal fluid. In an experiment in rats, it was transferred to nerve cell organelles more efficiently than CN-vitamin B12. It also accelerated the synthesis of the major structural component of the axon (protein) in sciatic nerve cells of rats with experimental diabetes and returned the protein transport rate close to normal, resulting in the maintenance of axonal function.
Mecobalamin repairs nerve tissues in experimental nerve injury models:
In experiments in rats and rabbits, mecobalamin was neuropathologically and electrophysiologically shown to inhibit the onset of nerve degeneration due to nerve disturbances caused by adriamycin and vincristine and experimental diabetes caused by streptozotocin. Mecobalamin was also compared with steroids in terms of their effects on the process of nerve regeneration in experimental facial paralysis models prepared by compressing the facial nerve of guinea pigs. Mecobalamin was found to be as effective as steroids for the recovery from paralysis when evaluated based on the winking reflex, induced electromyography and histological evaluation.
Mecobalamin inhibits abnormal excitation transmission by nerve tissues:
The anterior and posterior roots of the spinal nerve were separated from the spinal cord of frogs and connected to the sciatic nerve. Electrical stimulation was given to the end of the sciatic nerve in Ringer's solution and the action potentials of the anterior and posterior roots were recorded. 500 mcg/mL of DBCC, OH-vitamin B12, CH3-vitamin B12 were dissolved in the Ringer's solution and the inhibition of excitation transmission by these compounds was compared. The inhibition of nervous excitation transmission produced by CH3-vitamin B12 was the strongest.
Mecobalamin improves anemia by accelerating the maturation and division of erythroblasts:
Mecobalamin accelerates the synthesis of nucleic acids in bone marrow, as well as the maturation and division of erythroblasts, resulting in an increase in the production of erythrocytes. Treatment with mecobalamin was shown to promptly reverse the decrease in RBC hemoglobin and hematocrit numbers, in vitamin B12-deficient rats.
Pharmacokinetics: Tablet: Single-Dose Administration: After oral administration of single doses of 120 and 1500 mcg of Methycobal to healthy adult subjects, dose-related peak plasma concentrations were both achieved after 3 hrs. From 40-80% of the cumulative amount of total B12 recovered in the urine by 24 hrs after oral administration were excreted within the first 8 hrs.
Repeated-Dose Administration: The percentages of increase in the plasma concentration of total B12 were determined in healthy subjects given an oral daily dose of 1500 mcg of Methycobal for 12 consecutive weeks. The changes in the plasma level were also measured in the same patients for a period of the first 4 weeks after the last administration.
The plasma concentration increased for the first 4 weeks after administration, reaching twice as high as the initial concentration. Thereafter it was followed by a gradual increase up to about 280% of that before administration at 12th week of the dosing, and then declined. But it was maintained at approximately 180% of the level before dosing 4 weeks after the last administration.
Injection: Single-Dose Administraton: When a single IM or IV dose of 500 mcg of CH3-B12 was administered to healthy adults, the time required for the serum total vitamin B12 level to reach a peak (Tmax) was 0.9 ± 0.1 hr after IM administration and immediately to 3 min after IV administration, and the increment in peak serum total vitamin B12 level (Cmax) was 22.4 ± 1.1 ng/mL after IM administration and 85±8.9 ng/mL after IV administration.
The area under the blood concentration-time curve (AUC) was 204.1 ± 12.9 hr·ng/mL after IM administration and 358.6 ± 34.4 hr·ng/mL after IV administration.
On the other hand, the rate of binding saturation showed a similar increase in both groups of subjects for 144 hrs after administration.
Repeated-Dose Administration: 500 mcg/day of CH3-B12 was administered IV to healthy adults for 10 consecutive days. Serum total vitamin B12 levels measured before each administration (Cmin) increased from day to day. At 2 days of administration the serum level of total vitamin B12 was 5.5±1.8 ng/mL, about 1.4 times the 24-hr value (3.9±1.2 ng/mL). At 3 days of administration it was increased to 6.8 ± 1.5 ng/mL, about 1.7 times the 24-hr value, and this level was maintained until the last dosing.
Clinical Studies: Tablet: Clinical Effects: In clinical studies including double-blind trials, Methycobal tablets produced good relief of symptoms in 44.5% of patients (5503/12,373) with peripheral neuropathies. In double-blind controlled comparative trials of Methycobal tablets with cobalamin (DBCC) or mecobalamin in lower doses (120 mcg) in patients at chronic-fixed phase, the efficacy and usefulness of Methycobal tablets were confirmed.
Adverse Reactions: Out of 15,180 patients treated with Methycobal tablets, adverse reactions were reported in 146 patients (0.96%). The most common adverse reactions include gastrointestinal symptoms eg, anorexia in 52 patients (0.34%), gastrointestinal disorders in 38 patients (0.25%), nausea-vomiting in 18 patients (0.12%), soft stool-diarrhea in 17 patients (0.11%) and skin rash in 14 patients (0.09%).
Influences on Laboratory Values: No changes due to Methycobal treatment in laboratory values have been reported.
Injection: Clinical Efficacy: It has been shown in double-blind studies that CH3-B12 benefits peripheral neuropathies when the general improvement of symptoms is evaluated. Equivalency in effect between the IV and IM routes has been demonstrated in double-blind clinical studies.
Adverse Reactions and Influences on Laboratory Values: Adverse reactions to Methycobal have been reported in 3 (0.27%) of 1864 cases. The main adverse reactions were eruptions in 2 cases (0.11%). No changes in laboratory values have been associated with Methycobal treatment.
Others: Methycobal should not be used over a period of months if there is lack of satisfactory clinical response in patients with megaloblastic anemia probably due to vitamin B12 deficiency or with peripheral neuropathies.
Non-Clinical Studies: Distribution: At 24 hrs after IV administration of 87Co-CH3-B12 to rats in a dose of 10 mcg/kg, the radioactivity was detected in order of high concentration in the kidneys, adrenal, intestine, pancreas and pituitary, and the concentration of radioactivity was relatively lower in the eyes, spinal cord, brain and muscle.
Toxicology: Acute toxicity LD50 (mg/kg): See table.
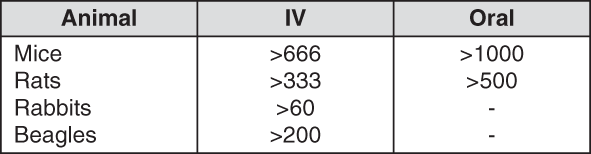 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSubacute Toxicity: Mecobalamin was administered IV to beagles in doses of 0.5, 5 and 50 mg/kg/day for 90 consecutive days. Changes in general conditions, body weight, blood and organ weights were unremarkable in all the dose groups of beagles. Histopathologically, increases in eosinophils and lysosomes were found in the observation with an optical microscope and an electron microscope, respectively, in the epithelial cells of proximal tubule in the animals of the 50 mg/kg/day dose group. No change, however, was noted in the other organs.
Chronic Toxicity: Mecobalamin was administered IV to beagles at doses of 0.3, 5 and 50 mg/kg/day for 12 consecutive months. Changes in general condition, body weight, blood and organ weights were unremarkable in all the dose groups of beagles. Histopathologically, increases in eosinophils and lysosomes were found in the observation with an optical microscope and an electron microscope, respectively, in the epithelial cells of proximal renal tubule in the 5 mg/kg/day or higher dose groups. In the 50 mg/kg/day dose groups lysosomes in the mesangial cells of the renal glomerulus and Kupffer cells in the liver were increased.
Teratogenicity: Reproduction Studies: Mecobalamin was administered IV in doses of 0.5, 5 and 50 mg/kg/day to rats before pregnancy, in the early stage of gestation, during the period of organogenesis and during the perinatal and lactating periods. No abnormal findings nor signs of teratogenicity were observed in the fetuses and newborns from these dams.