


 Sign Out
Sign Out


In clinical studies of up to 112 weeks duration, ezetimibe 10 mg daily was administered alone in 2396 patients, or with a statin in 11,308 patients or with fenofibrate in 185 patients. Adverse reactions were usually mild and transient. The overall incidence of side effects was similar between ezetimibe and placebo. Similarly, the discontinuation rate due to adverse experiences was comparable between ezetimibe and placebo.
According to available data 1200 patients took rosuvastatin and ezetimibe combination in clinical studies. As reported in the published literature, the most frequent common adverse events related to rosuvastatin-ezetimibe combination treatment in hypercholesterolemic patients are increased hepatic transaminases, gastrointestinal problems and muscle pain. These are known undesirable effects of the active substances. However, a pharmacodynamic interaction, in terms of adverse effects, between rosuvastatin and ezetimibe cannot be ruled out (see Pharmacology: Pharmacokinetics under Actions).
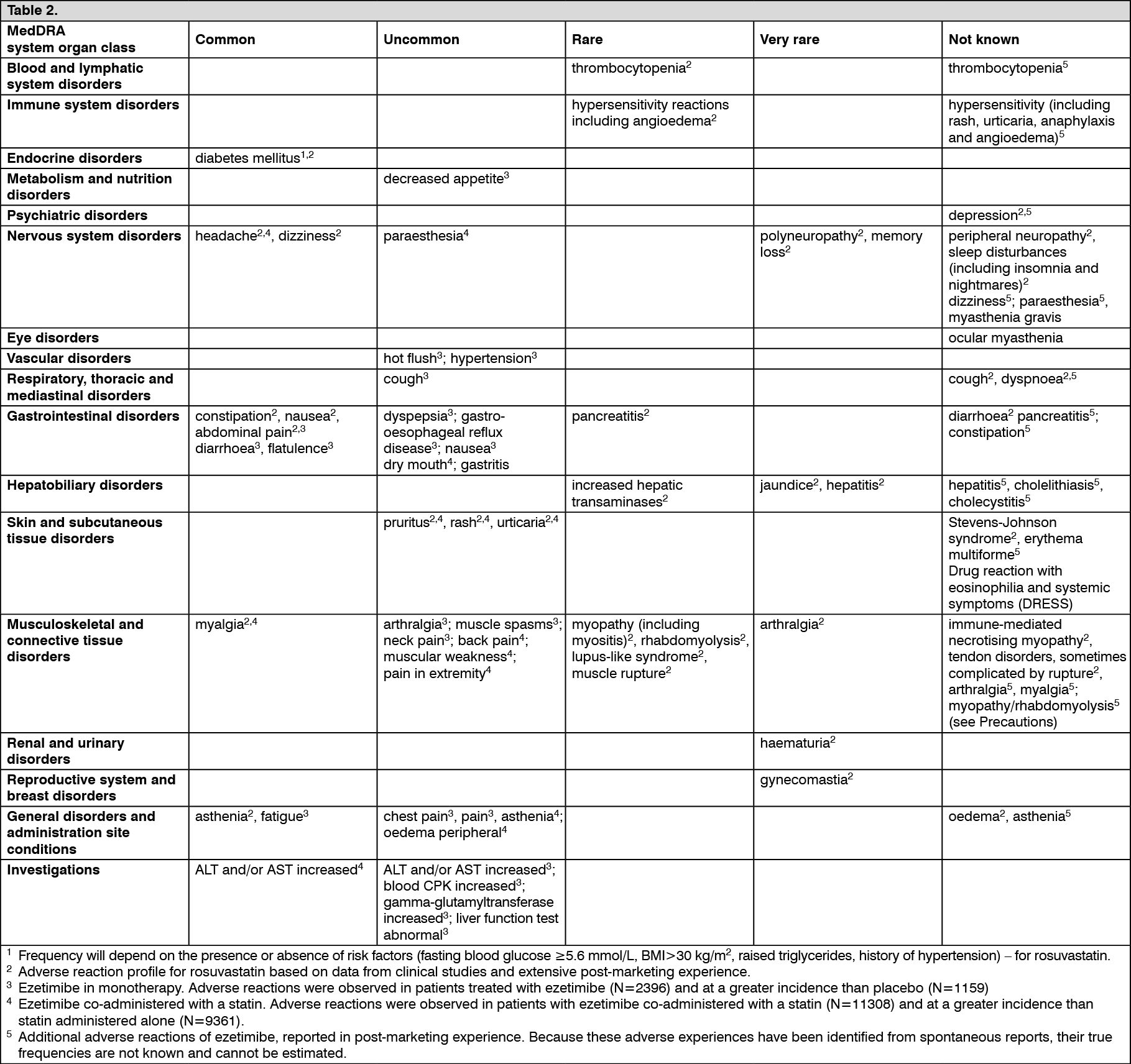
Tabulated list of adverse reactions: The frequencies of adverse events are ranked according to the following: Common (≥1/100 to <1/10); Uncommon (≥1/1,000 to <1/100); Rare (≥1/10,000 to <1/1,000); Very rare (<1/10,000); Not known (cannot be estimated from the available data). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAs with other HMG-CoA reductase inhibitors, the incidence of adverse drug reactions tends to be dose dependent.
Renal effects: Proteinuria, detected by dipstick testing and mostly tubular in origin, has been observed in patients treated with rosuvastatin. Shifts in urine protein from none or trace to ++ or more were seen in <1% of patients at some time during treatment with 10 and 20 mg, and in approximately 3% of patients treated with 40 mg. A minor increase in shift from none or trace to + was observed with the 20 mg dose. In most cases, proteinuria decreases or disappears spontaneously on continued therapy.
Review of data from clinical trials and post-marketing experience to date has not identified a causal association between proteinuria and acute or progressive renal disease.
Haematuria has been observed in patients treated with rosuvastatin and clinical trial data show that the occurrence is low.
Skeletal Muscle Effects: Effects on skeletal muscle e.g. myalgia, myopathy (including myositis), and, rarely, rhabdomyolysis with and without acute renal failure have been reported in rosuvastatin-treated patients with all doses and in particular with doses >20 mg.
A dose-related increase in CK levels has been observed in patients taking rosuvastatin; the majority of cases were mild, asymptomatic and transient. If CK-levels are elevated (>10xULN), the treatment should be discontinued (see Precautions).
Liver Effects: As with other HMG-CoA reductase inhibitors, a dose-related increase in transaminases has been observed in a small number of patients taking rosuvastatin; the majority of cases were mild, asymptomatic and transient.
The following adverse events have been reported with some statins: Sexual dysfunction; Exceptional cases of interstitial lung disease, especially with long term therapy (see Precautions).
The reporting rates for rhabdomyolysis, serious renal events and serious hepatic events (consisting mainly of increased hepatic transaminases) are higher at the 40 mg rosuvastatin dose.
Laboratory values: In controlled clinical monotherapy trials, the incidence of clinically important elevations in serum transaminases (ALT and/or AST ≥3X ULN, consecutive) was similar between ezetimibe (0.5%) and placebo (0.3%). In co-administration trials, the incidence was 1.3% for patients treated with ezetimibe co-administered with a statin and 0.4% for patients treated with a statin alone. These elevations were generally asymptomatic, not associated with cholestasis, and returned to baseline after discontinuation of therapy or with continued treatment (see Precautions).
In clinical trials, CPK >10X ULN was reported for 4 of 1,674 (0.2%) patients administered ezetimibe alone vs 1 of 786 (0.1%) patients administered placebo, and for 1 of 917 (0.1%) patients co-administered ezetimibe and a statin vs 4 of 929 (0.4%) patients administered a statin alone. There was no excess of myopathy or rhabdomyolysis associated with ezetimibe compared with the relevant control arm (placebo or statin alone) (see Precautions).
Paediatric population: The safety and efficacy of LYPSTAPLUS in children below the age of 18 years has not yet been established (see Pharmacology: Pharmacodynamics under Actions).
Rosuvastatin: Creatine kinase elevations >10xULN and muscle symptoms following exercise or increased physical activity were observed more frequently in a 52-week clinical trial of children and adolescents compared to adults. In other respects, the safety profile of rosuvastatin was similar in children and adolescents compared to adults.
Ezetimibe: Paediatric (6 to 17 years of age) patients: In a study involving paediatric (6 to 10 years of age) patients with heterozygous familial or non-familial hypercholesterolaemia (n=138), elevations of ALT and/or AST (≥3X ULN, consecutive) were observed in 1.1% (1 patient) of the ezetimibe patients compared to 0% in the placebo group.
There were no elevations of CPK (≥10X ULN). No cases of myopathy were reported.
In a separate study involving adolescent (10 to 17 years of age) patients with heterozygous familial hypercholesterolaemia (n=248), elevations of ALT and/or AST (≥3X ULN, consecutive) were observed in 3% (4 patients) of the ezetimibe/simvastatin patients compared to 2% (2 patients) in the simvastatin monotherapy group; these figures were respectively 2% (2 patients) and 0% for elevation of CPK (≥10X ULN). No cases of myopathy were reported. These trials were not suited for comparison of rare adverse drug reactions.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
View ADR Monitoring Form