


 Sign Out
Sign Out


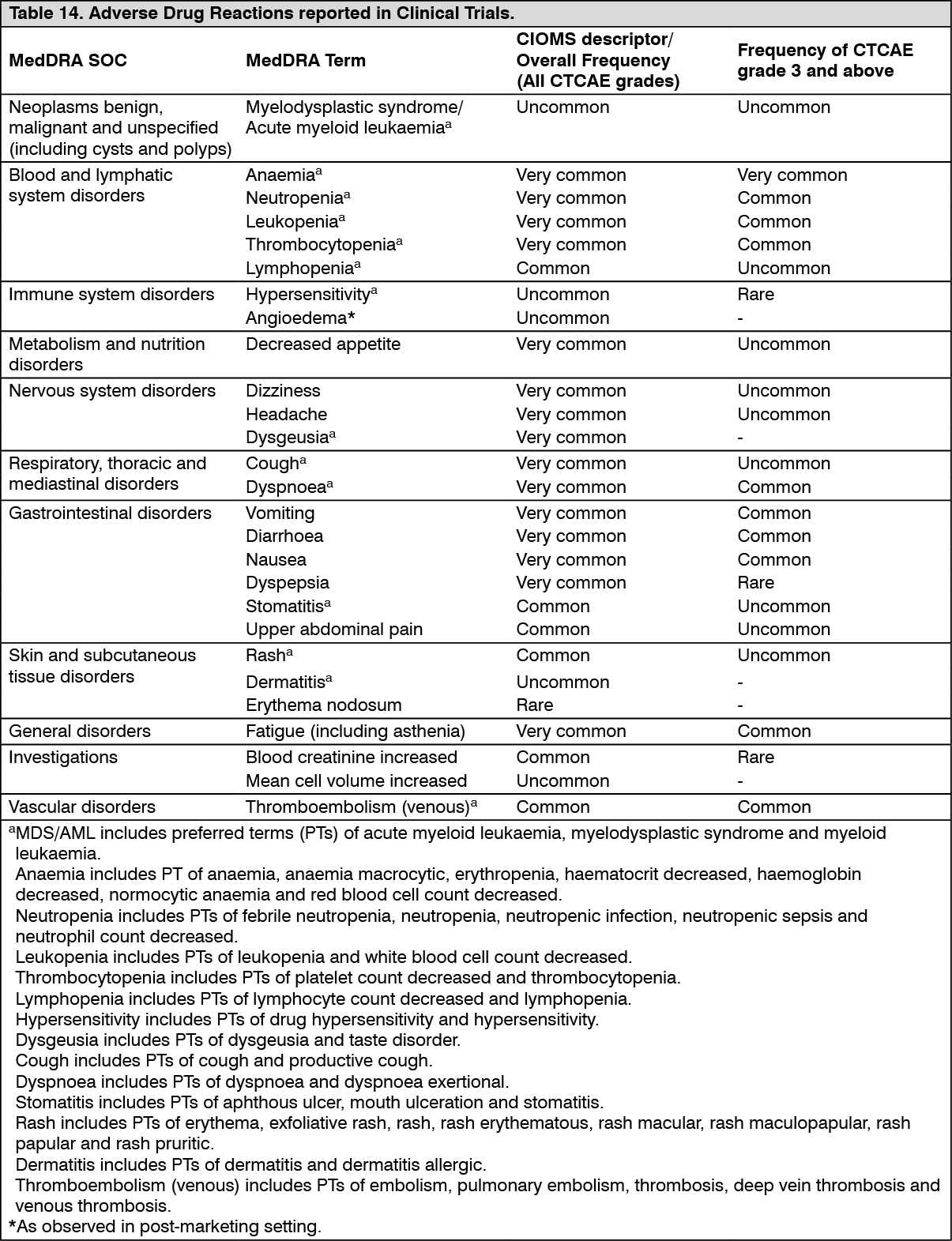
Tabulated list of adverse drug reactions from clinical trials: The following adverse reactions have been identified in completed clinical trials with patients receiving Lynparza monotherapy where patient exposure is known. Adverse Drug Reactions are organized by MedDRA System Organ Class (SOC) and then by MedDRA preferred term in Tables 14 and 15. Within each SOC, preferred terms are arranged by decreasing frequency and then by decreasing seriousness. Frequencies of occurrence of adverse reactions are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1000); and very rare (<1/10,000) including isolated reports.
Hard capsule: The safety profile is based on pooled data from 4098 patients with solid tumours treated with Lynparza monotherapy in clinical trials. (See Table 14.)
 Click on icon to see table/diagram/image
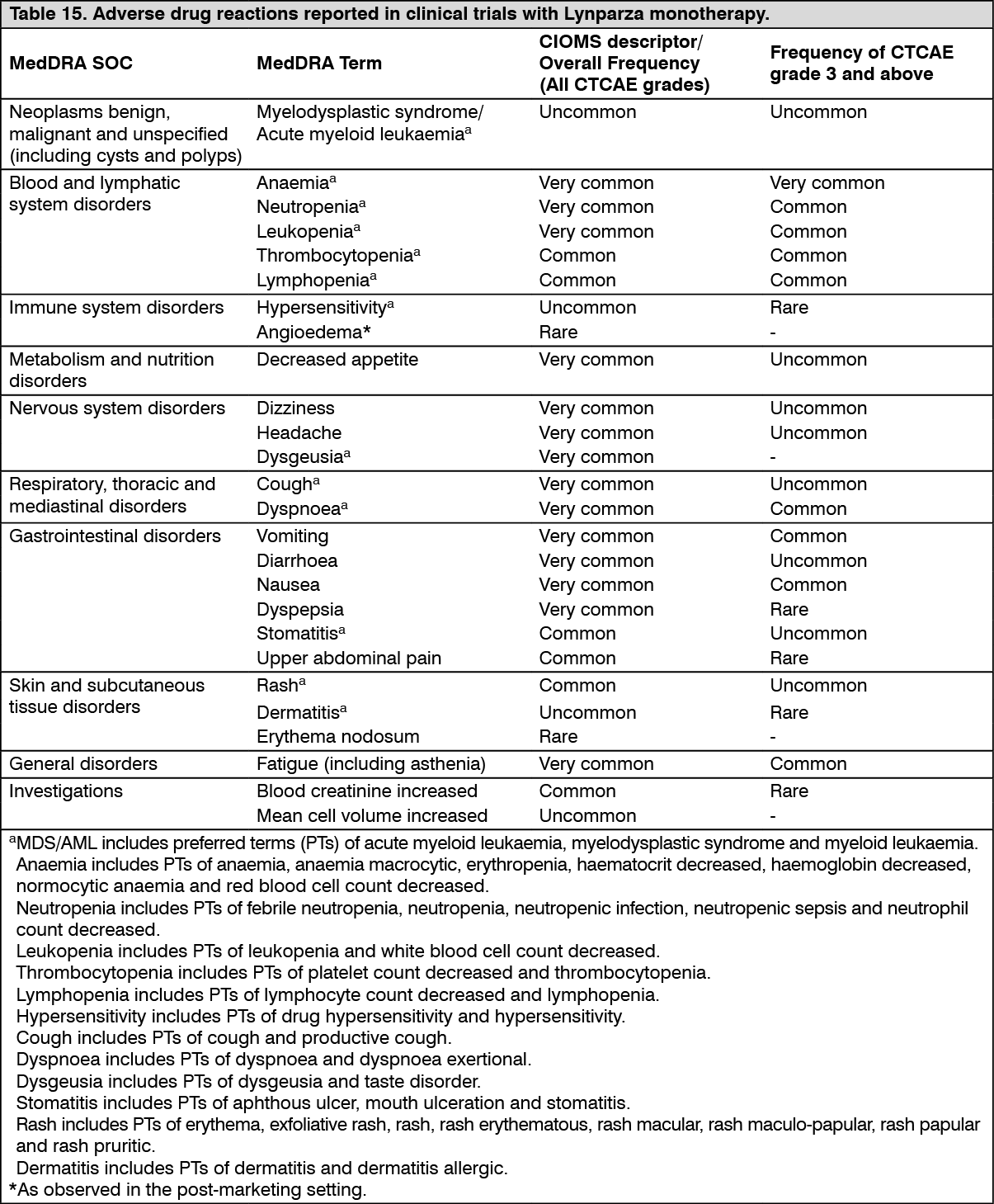
Click on icon to see table/diagram/imageFC tablet: The safety profile is based on pooled data from 3988 patients with solid tumours treated with Lynparza monotherapy and 535 patients treated with Lynparza in combination with bevacizumab in clinical trials at the recommended dose.
When Lynparza is used in combination with bevacizumab, the safety profile is generally consistent with that of the individual therapies. (See Table 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Myelodysplastic syndrome/Acute myeloid leukaemia: In clinical studies, across all indications and formulations, MDS/AML occurred uncommonly in patients on treatment and during the 30-day safety follow up, and < 1.5% at any time after starting olaparib, including cases actively solicited during the long term follow up for overall survival.
In patients with BRCAm platinum-sensitive relapsed ovarian cancer who had received at least two prior lines of platinum chemotherapy and received study treatment until disease progression (SOLO2 study, tablet formulation, with olaparib treatment ≥ 2 years in 45% of patients), the incidence of MDS/AML was 8% in patients receiving olaparib and 4% in patients receiving placebo at a follow-up of 5 years. In the olaparib arm, 9 out of 16 MDS/AML cases occurred after discontinuation of olaparib during the survival follow-up. The incidence of MDS/AML was observed in the context of extended overall survival in the olaparib arm and late onset of MDS/AML. The risk of MDS/AML remains < 1.5% at 5 year follow up in the first-line setting when olaparib maintenance treatment is given after one line of platinum chemotherapy for a duration of 2 years (SOLO1, tablet formulation).
Haematological toxicity: Anaemia and other haematological toxicities are generally low grade (CTCAE grade 1 or 2), however, there are reports of CTCAE grade 3 and higher events. Anaemia was the most common CTCAE grade ≥3 adverse reaction reported in clinical studies with first onset generally reported in the first 3 months of treatment. An exposure-response relationship between olaparib and decreases in haemoglobin has been demonstrated.
The incidence of elevations in mean corpuscular volume from low to normal at baseline to above the upper limit of normal was approximately 58% (Hard capsule) and 51% (FC tablet). Levels appeared to return to normal after treatment discontinuation and did not appear to have any clinical consequences.
Baseline testing, followed by monthly monitoring, of complete blood counts is recommended for the first 12 months of treatment, and periodically after this time, to monitor for clinically significant changes in any parameter during treatment which may require dose interruption or reduction and/or further treatment (see Dosage & Administration and Precautions).
Hard capsule: In clinical studies with Lynparza the incidence of CTCAE grade ≥2 shifts (decreases) from baseline in haemoglobin was 23%, absolute neutrophils 19%, platelets 6%, lymphocytes 29% and leucocytes 20% (all % approximate).
FC tablet: In clinical studies with Lynparza monotherapy the incidence of CTCAE grade ≥2 shifts (decreases) from baseline in haemoglobin was 21%, absolute neutrophils 17%, platelets 5%, lymphocytes 26% and leucocytes 19% (all % approximate).
Other laboratory findings: In clinical studies with Lynparza monotherapy the incidence of CTCAE grade ≥2 shifts (elevations) from baseline in blood creatinine was approximately 11%. Data from a double-blind placebo-controlled study showed median increase up to 23% from baseline remaining consistent over time and returning to baseline after treatment discontinuation, with no apparent clinical sequelae. 90% of patients had creatinine values of CTCAE grade 0 at baseline and 10% were CTCAE grade 1 at baseline.
Nausea and vomiting: Nausea was generally reported very early, with first onset within the first month of Lynparza treatment in the majority of patients. Vomiting was reported early, with first onset within the first two months of Lynparza treatment in the majority of patients. Both nausea and vomiting were reported to be intermittent for the majority of patients.
View ADR Monitoring Form