


 Sign Out
Sign Out


 Click on icon to see table/diagram/image
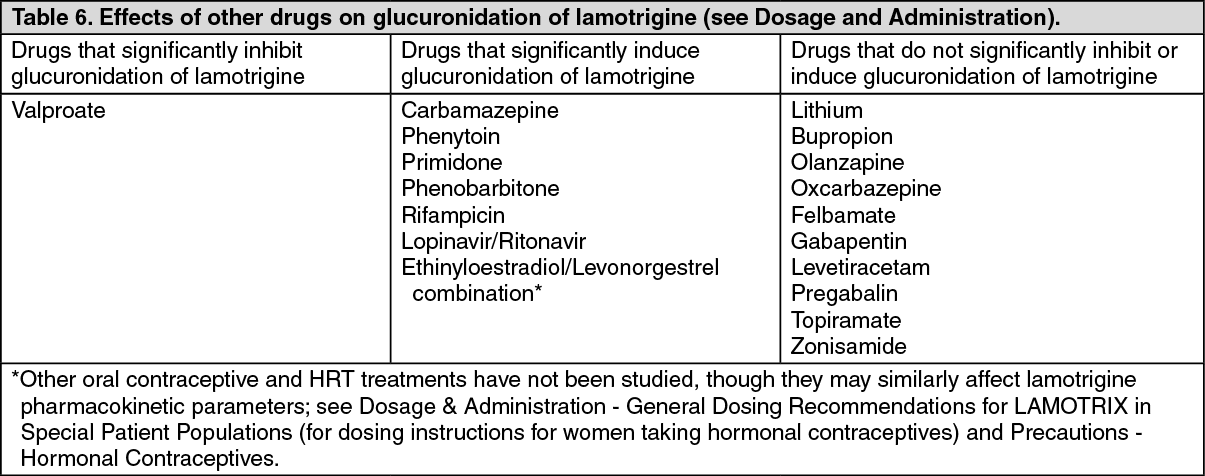
Click on icon to see table/diagram/imageInteractions involving AEDs (see Dosage & Administration):Valproate, which inhibits the glucuronidation of lamotrigine, reduces the metabolism of lamotrigine and increases the mean half life of lamotrigine nearly two fold. (See Precautions and Dosage & Administration.) Certain antiepileptic agents (such as phenytoin, carbamazepine, phenobarbitone and primidone) which induce cytochrome P450 enzymes also induce UGTs and therefore enhance the metabolism of lamotrigine. Other drug-classes which induce hepatic drug-metabolising enzymes may also enhance the metabolism of lamotrigine.
There have been reports of central nervous system events including dizziness, ataxia, diplopia, blurred vision and nausea in patients taking carbamazepine following the introduction of lamotrigine. These events usually resolve when the dose of carbamazepine is reduced. A similar effect was seen during a study of lamotrigine and oxcarbazepine in healthy adult volunteers, but dose reduction was not investigated.
In a study of healthy adult volunteers using doses of 200 mg lamotrigine and 1200 mg oxcarbazepine, oxcarbazepine did not alter the metabolism of lamotrigine and lamotrigine did not alter the metabolism of oxcarbazepine. The pharmacokinetic interaction between lamotrigine and oxcarbazepine in children has not been studied.
In a study in healthy volunteers, coadministration of felbamate (1,200 mg twice daily) with lamotrigine (100 mg twice daily for 10 days) appeared to have no clinically relevant effects on the pharmacokinetics of lamotrigine. Based on a retrospective analysis of plasma levels in patients who received lamotrigine both with and without gabapentin, gabapentin does not appear to change the apparent clearance of lamotrigine.
Potential drug interactions between levetiracetam and lamotrigine were assessed by evaluating serum concentrations of both agents during placebo-controlled clinical trials. These data indicate that lamotrigine does not influence the pharmacokinetics of levetiracetam and that levetiracetam does not influence the pharmacokinetics of lamotrigine. Steady-state trough plasma concentrations of lamotrigine were not affected by concomitant pregabalin (200 mg 3 times daily) administration. There are no pharmacokinetic interactions between lamotrigine and pregabalin. Topiramate resulted in no change in plasma concentrations of lamotrigine. Administration of lamotrigine resulted in a 15% increase in topiramate concentrations. In a study of patients with epilepsy, co-administration of zonisamide (200 to 400 mg/day) with lamotrigine (150 to 500 mg/day) for 35 days had no significant effect on the pharmacokinetics of lamotrigine. Plasma concentrations of lamotrigine were not affected by concomitant lacosamine (200, 400 or 600 mg/day) in placebo-controlled clinical trials in patients with partial-onset seizures.
In a pooled analysis of data from three placebo-controlled clinical trials investigating adjunctive perampanel in patients with partial-onset and primary generalised tonic-clonic seizures, the highest perampanel dose evaluated (12 mg/day) increased lamotrigine clearance by less than 10%. An effect of this magnitude is not considered to be clinical relevant. Although changes in the plasma concentrations of other antiepileptic drugs have been reported, controlled studies have shown no evidence that lamotrigine affects the plasma concentrations of concomitant antiepileptic drugs. Evidence from in-vitro studies indicates that lamotrigine does not displace other antiepileptic drugs from protein binding sites.
Interactions involving other psychoactive agents (see Dosage & Administration):The pharmacokinetic of lithium after 2g of anhydrous lithium gluconate given twice daily for six days to 20 healthy subjects were not altered by co-administration of 100 mg/day lamotrigine.
Multiple oral doses of bupropion had no statistically significant effects on the single dose pharmacokinetics of lamotrigine in 12 subjects and had only a slight increase in the AUC of lamotrigine glucuronide.
In a study in healthy adult volunteers, 15 mg olanzapine reduced the AUC and Cmax of lamotrigine by an average of 24% and 20%, respectively. An effect on this magnitude is not generally expected to be clinically relevant. Lamotrigine at 200 mg did not affect the pharmacokinetics of olanzapine.
Multiple oral doses of lamotrigine 400 mg daily had no clinically significant effect on the single dose pharmacokinetics of 2 mg risperidone in 14 healthy adult volunteers. Following the co-administration of risperidone 2 mg with lamotrigine, 12 out of the 14 volunteers reported somnolence compared to 1 out of 20 when risperidone was given alone, and none when lamotrigine was administered alone. In a study of 18 adult patients with bipolar I disorder, receiving an established regimen of lamotrigine (>/=100 mg/day), doses of aripiprazole were increased from 10 mg/day to a target of 30 mg/day over a 7 day period and continued once daily for a further 7 days. An average reduction of approximately 10% in Cmax and AUC of lamotrigine was observed. An effect of this magnitude is not expected to be of clinical consequence.
In vitro inhibition experiments indicated that the formation of lamotrigine's primary metabolite, the 2-N-glucuronide, was minimally affected by co-incubation with amitriptyline, bupropion, clonazepam, fluoxetine, haloperidol, or lorazepam. Bufuralol metabolism data from human liver microsome suggested that lamotrigine does not reduce the clearance of drugs eliminated predominantly by CYP2D6. Results of in vitro experiments also suggest that clearance of lamotrigine is unlikely to be affected by clozapine, phenelzine, risperidone, sertraline or trazodone.
Interactions involving hormonal contraceptives: Effect of hormonal contraceptives on lamotrigine pharmacokinetics: In a study of 16 female volunteers, 30 mcg ethinyloestradiol/150mcg levonorgestrel in a combined oral contraceptive pill caused an approximately two-fold increase in lamotrigine oral clearance, resulting in an average 52% and 39% reduction in lamotrigine AUC and Cmax, respectively. Serum lamotrigine concentrations gradually increased during the course of the week of inactive medication (e.g. "pill-free" week), with pre-dose concentrations at the end of the week of inactive medication being, on average, approximately two-fold higher than during co-therapy. (see Dosage & Administration, for dosing instructions for women taking hormonal contraceptives, and Hormonal Contraceptives under Precautions).
Effects of lamotrigine on hormonal contraceptive pharmacokinetics: In a study of 16 female volunteers, a steady state dose of 300mg lamotrigine had no effect on the pharmacokinetics of the ethinyloestradiol component of combined oral contraceptive pill. A modest increase in oral clearance of the levonorgestrel component was observed, resulting in an average 19% and 12% reduction in levonorgestrel AUC and Cmax, respectively. Measurement of serum FSH, LH, and oestradiol during the study indicated some loss of suppression of ovarian hormonal activity in some women, although measurement of serum progesterone indicated that there was no hormonal evidence of ovulation in any of the 16 subjects. The impact of the modest increase in the levonorgestrel clearance, and the change in the serum FSH and LH, on ovarian ovulatatory activity is unknown (see Precautions). The effects of doses of lamotrigine other than 300mg/day have not been studied and studies with other female hormonal preparations have not been conducted.
Interactions involving other medications: In a study in 10 male volunteers, rifampicin increased lamotrigine clearance and decrease lamotrigine half-life due to induction of the hepatic enzymes responsible for glucuronidation. In patients receiving concomitant therapy with rifampicin, the treatment regimen recommended for lamotrigine and concurrent glucuronidation inducers should be used (see Dosage & Administration).
In a study in healthy volunteers, lopinavir/ritonavir approximately halved the plasma concentrations of lamotrigine, probably by induction of glucuronidation. In patients receiving concomitant therapy with lopinavir/ritonavir, the treatment regimen recommended for lamotrigine and concurrent glucuronidation inducers should be used (see Dosage & Administration). Data from in vitro assessment of the effect of lamotrigine at OCT 2 demonstrate that lamotrigine, but not the N(2)-glucuronide metabolite, is an inhibitor of OCT 2 at potentially clinically relevant concentrations. These data demonstrate that lamotrigine is an inhibitor of OCT 2, with an IC 50 value of 53.8 μM (see Precautions).
Interactions involving laboratory tests: LAMOTRIX has been reported to interfere with the assay used in some rapid urine drug screens, which can result in false positive readings, particularly for phencyclidine (PCP). A more specific alternative chemical method should be used to confirm a positive result.