Pharmacotherapeutic Group: Antibacterial for systemic use, macrolide.
ATC Code: J01FA09.
Pharmacology: Pharmacodynamics: Clarithromycin is a semi-synthetic macrolide antibiotic obtained by substitution of a CH
3O group for the hydroxyl (OH) group at position 6 of the erythromycin lactonic ring. Specifically clarithromycin is 6-O-methyl erythromycin A. The white to off-white antibiotic powder is bitter, practically odorless, essentially insoluble in water and slightly soluble in ethanol, methanol, and acetonitrile. Its molecular weight is 747.96.
Clarithromycin exerts its antibacterial action by binding to the 50s ribosomal subunit of susceptible bacteria and suppresses protein synthesis.
Clinical Studies: Helicobacter pylori is strongly associated with peptic ulcer disease. Ninety (90) to 100% of patients with duodenal ulcers are infected with this pathogen. Eradication of
H. pylori has been shown to reduce the rate of duodenal ulcer recurrence, thereby reducing the need for maintenance anti-secretory therapy.
Triple Therapy in Duodenal Ulcer Disease: In a well-controlled double blind study,
H. pylori-infected duodenal ulcer patients received triple therapy with clarithromycin 500 mg twice daily, amoxicillin 1,000 mg twice daily and omeprazole 20 mg daily for 10 days or dual therapy with clarithromycin 500 mg 3 times daily and omeprazole 40 mg daily for 14 days.
Helicobacter pylori was eradicated in 90% of the patients receiving clarithromycin triple therapy and in 60% of the patients receiving dual therapy.
In an independent study,
H. pylori-infected patients received eradication therapy with clarithromycin 500 mg twice daily in conjunction with amoxicillin 1,000 mg twice daily and omeprazole 20 mg daily (Group A) or omeprazole 20 mg twice daily (Group B) for 7 days. In those patients not previously treated with anti-
H. pylori therapy,
H. pylori was eradicated in 86% (95% CI = 69-95) of patients in Group A and 75% (95% CI=62-85) of patients in Group B, the difference was not statistically significant.
In an open-label study
H. pylori-infected patients with duodenal ulcer or non-ulcer dyspepsia (NUD) received eradication therapy with clarithromycin 500 mg twice daily, lansoprazole 30 mg twice daily plus amoxicillin 1,000 mg twice daily for 10 days. In an all-patients-treated analysis,
H. pylori was eradicated from 91% of patients.
Dual Therapy in Duodenal Ulcer Disease: In well-controlled, double-blind studies,
H. pylori-infected duodenal ulcer patients received eradication therapy with clarithromycin 500 mg 3 times daily and omeprazole 40 mg daily for 14 days followed by omeprazole 40 mg (study A) or omeprazole 20 mg (studies B, C and D) daily for an additional 14 days; patients in each control group received omeprazole alone for 28 days. In study A,
H. pylori was eradicated in over 80% of patients who received clarithromycin and omeprazole and in only 1% of patients receiving omeprazole alone. In studies B, C and D, the combined eradication rate was over 70% (clinically evaluable analysis) in patients receiving clarithromycin and omeprazole and <1% in patients receiving omeprazole alone. In each study, the rate of ulcer recurrence at 6 months was statistically lower in the clarithromycin and omeprazole-treated patients when compared to patients receiving omeprazole alone.
In an investigator-blind study,
H. pylori-infected patients received eradication therapy with clarithromycin 500 mg three times daily in conjunction with lansoprazole 60 mg/day in single or divided doses for 14 days. The combined eradication rate was over 60%.
Pharmacokinetics: Absorption: The kinetics of orally administered clarithromycin has been studied extensively in a number of animal species and adult humans. These studies have shown clarithromycin is readily and rapidly absorbed with an absolute bioavailability of approximately 50%. Little or no unpredicted accumulation was found and the metabolic disposition did not change in any species following multiple dosing. Food intake immediately before dosing increases clarithromycin bioavailability by a mean of 25%. Overall, this increase is minor and should be of little clinical significance with the recommended dosing regimens. Clarithromycin may thus be administered in either the presence or absence of food.
Distribution, Biotransformation and Elimination: In vitro: In vitro studies showed that the protein-binding of clarithromycin in human plasma averaged about 70% at concentrations of 0.45-4.5 mcg/mL. A decrease in binding to 41-45% mcg/mL suggested the binding sites might become saturated, but this only occurred at concentrations far in excess of the therapeutic drug levels.
In vivo: Results of animal studies showed clarithromycin levels in all tissues, except the central nervous system (CNS), were several times higher than the circulating drug levels. The highest concentrations were usually found in the liver and lung where the tissue to plasma (T/P) ratios reached 10-20.
Normal Subjects: With twice daily dosing at 250 mg, the peak steady-state plasma concentration was attained in 2-3 days and averaged about 1 mcg/mL for clarithromycin and 0.6 mcg/mL for 14-OH-clarithromycin, while the elimination half-lives (t
½) of the parent drug and metabolite were 3-4 hrs and 5-6 hrs, respectively. With twice daily dosing at 500 mg, the steady-state peak plasma concentration (C
max) for clarithromycin and its hydroxylated metabolite was achieved by the 5th dose. After the 5th and 7th doses, the steady-state C
max for clarithromycin averaged 2.7 and 2.9 mcg/mL; its hydroxylated metabolite averaged 0.88 and 0.83 mcg/mL, respectively. The t
½ of the parent drug at the 500-mg dose level was 4.5-4.8 hrs, while that of the 14-OH-clarithromycin was 6.9-8.7 hrs. At steady-state, the 14-OH-clarithromycin levels did not increase proportionately with the clarithromycin dose, and the apparent t
½ of both clarithromycin and its hydroxylated metabolite tended to be longer at the higher doses. This non-linear pharmacokinetic behavior of clarithromycin, coupled with the overall decrease in the formation of 14-hydroxylation and N-demethylation products at the higher doses, indicates the non-linear metabolism of clarithromycin becomes more pronounced at high doses.
In human adults given single oral doses of clarithromycin 250 or 1,200 mg, urinary excretion accounted for 37.9% of the lower dose and 46% of the higher dose. Fecal elimination accounted for 40.2% and 29.1% (this included a subject with only 1 stool sample containing 14.1%) of these respective doses.
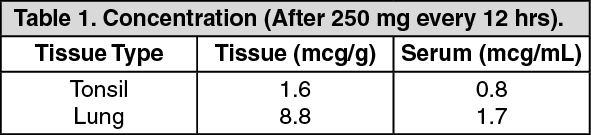
Patients: Clarithromycin and its 14-OH metabolite distribute readily into body tissues and fluids. Limited data from a small number of patients suggests clarithromycin does not achieve significant levels in cerebrospinal fluid (CSF) after oral doses (ie, only 1-2% of serum levels in CSF in patients with normal blood-CSF barriers). Concentrations in tissues are usually several fold higher than serum concentrations. Examples from tissue and serum concentrations are presented in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Hepatic Impairment:
Click on icon to see table/diagram/image
Hepatic Impairment: In a study comparing 1 group of healthy human subjects with a group of subjects with liver impairment who were given clarithromycin 250 mg twice daily for 2 days and a single 250-mg dose, the 3rd day, steady-state plasma levels and systemic clearing of clarithromycin were not significantly different between the 2 groups. In contrast, steady-state concentrations of the 14-OH metabolite were markedly lower in the group of hepatic-impaired subjects. This decreased metabolic clearance of the parent compound by 14-hydroxylation was partially offset by an increase in the renal clearance of parent drug, resulting in comparable steady-state levels of parent drug in the hepatic-impaired and healthy subjects. These results indicate no adjustment of dosage is necessary for subjects with moderate or severe hepatic impairment but with normal renal function.
Renal Impairment: A study was conducted to evaluate and compare the pharmacokinetic profile of multiple 500 mg oral doses of clarithromycin in subjects with normal and decreased renal function. The plasma levels, t
½, C
max and minimum plasma concentration (C
min) for both clarithromycin and its 14-OH metabolite were higher and area under the concentration-time curve (AUC) was larger in subjects with renal impairment.
K
elim and urinary excretion were lower. The extent to which these parameters differed was correlated with the degree of renal impairment; the more severe the renal impairment, the more significant the difference (see Dosage & Administration).
Elderly: A study was also conducted to evaluate and compare the safety and pharmacokinetic profiles of multiple 500-mg oral doses of clarithromycin in healthy elderly male and female subjects to those in healthy young adult male subjects. In the elderly group, circulating plasma levels were higher and elimination slower than in the younger group for both parent drug and 14-OH metabolite. However, there was no difference between the 2 groups when renal clearance was correlated with creatinine clearance. It is concluded from those results that any effect on the handling of clarithromycin is related to renal function and not to age
per se.
Mycobacterium avium Infections: Steady-state concentrations of clarithromycin and 14-OH-clarithromycin observed following administration of 500 mg doses of clarithromycin every 12 hrs to adult patients with human immunodeficiency virus (HIV) infection were similar to those observed in normal subjects. However, at the higher doses which may be required to treat
Mycobacterium avium infections, clarithromycin concentrations were much higher than those observed at the usual doses. In adult HIV-infected patients taking 1,000 and 2,000 mg/day in 2 divided doses, steady-state clarithromycin C
max values ranged from 2-4 mcg/mL and 5-10 mcg/mL, respectively. Elimination t
½ appeared to be lengthened at these higher doses as compared to that seen with usual doses in normal subjects. The higher plasma concentrations and longer elimination t
½ observed at these doses are consistent with the known nonlinearity in clarithromycin pharmacokinetics.
Concomitant Omeprazole Administration: A pharmacokinetic study was conducted with clarithromycin 500 mg 3 times daily and omeprazole 40 mg once-daily. When clarithromycin was given alone at 500 mg every 8 hrs, the mean steady-state C
max value was approximately 3.8 mcg/mL and the mean C
min value was approximately 1.8 mcg/mL. The mean AUC
0-8 for clarithromycin was 22.9 mcg/hr/mL. The time to reach maximum plasma concentration (T
max) and t
½ were 2.1 hr and 5.3 hr, respectively, when clarithromycin was dosed at 500 mg 3 times daily.
In the same study, when clarithromycin 500 mg 3 times daily was administered with omeprazole 40 mg once-daily, increases in omeprazole t
½ and AUC
0-24 were observed. For all subjects combined, the mean omeprazole AUC
0-24 was 89% greater and the harmonic mean for omeprazole t
½ was 34% greater when omeprazole was administered with clarithromycin than when omeprazole was administered alone. When clarithromycin was administered with omeprazole, the steady-state C
max, C
min, and AUC
0-8 of clarithromycin were increased by 10%, 27%, and 15%, respectively, over values achieved when clarithromycin was administered with placebo.
At steady-state, clarithromycin gastric mucous concentrations 6 hrs post-dosing were approximately 25-fold higher in the clarithromycin/omeprazole group compared with the clarithromycin alone group. Six (6) hrs post-dosing, mean clarithromycin gastric tissue concentrations were approximately 2-fold higher when clarithromycin was given with omeprazole than when clarithromycin was given with placebo.
Toxicology: Preclinical Safety Data: Acute, Subchronic and Chronic Toxicity: Studies were conducted in mice, rats, dogs and/or monkeys with clarithromycin administered orally. The duration of administration ranged from a single oral dose to repeated daily oral administration for 6 consecutive months. In acute mouse and rat studies, 1 rat, but no mice, died following a single gavage of 5 g/kg body weight. The median lethal dose, therefore, was >5 g/kg, the highest feasible dose for administration.
No adverse effects were attributed to clarithromycin in primates exposed to 100 mg/kg/day for 14 consecutive days or to 35 mg/kg/day for 1 month. Similarly, no adverse effects were seen in rats exposed to 75 mg/kg/day for 1 month, to 35 mg/kg/day for 3 months or to 8 mg/kg/day for 6 months. Dogs were more sensitive to clarithromycin, tolerating 50 mg/kg/day for 14 days, 10 mg/kg/day for 1 and 3 months, and 4 mg/kg/day for 6 months without adverse effects.
The major clinical signs at toxic doses in these studies described previously included emesis, weakness, reduced food consumption and reduced weight gain, salivation, dehydration and hyperactivity. Two (2) of 10 monkeys receiving 400 mg/kg/day died on treatment day 8; yellow discolored feces were passed on a few isolated occasions by some surviving monkeys given a dose of 400 mg/kg/day for 28 days.
The primary target organ at toxic dosages in all species was the liver. The development of hepatotoxicity in all species was detectable by early elevation of serum concentrations of alkaline phosphatase, alanine and aspartate aminotransferase, γ-glutamyl transferase and/or lactic dehydrogenase. Discontinuation of the drug generally resulted in a return to or toward normal concentrations of these specific parameters.
Additional tissues less commonly affected in the various studies included the stomach, thymus and other lymphoid tissues and the kidneys. Conjunctival injection and lacrimation, following near therapeutic dosages, occurred in dogs only. At a massive dosage of 400 mg/kg/day, some dogs and monkeys developed corneal opacities and/or edema.
Fertility, Reproduction and Teratogenicity: Fertility and reproduction studies have shown daily dosages of 150-160 mg/kg/day to male and female rats caused no adverse effects on the estrous cycle, fertility, parturition and number and viability of offspring. Two (2) teratogenicity studies in both Wistar (oral) and Sprague-Dawley (oral and IV) rats, 1 study in New Zealand White rabbits and 1 study in cynomolgus monkeys failed to demonstrate any teratogenicity from clarithromycin. Only in 1 additional study in Sprague-Dawley rats at similar doses and essentially similar conditions did a very low, statistically insignificant incidence (approximately 6%) of cardiovascular anomalies occur. These anomalies appeared to be due to spontaneous expression of genetic changes within the colony. Two (2) studies in mice also revealed a variable incidence of cleft palate (3-30%) following doses of 70 times the upper range of the usual daily human clinical dose (500 mg twice daily), but not at 35 times the maximal daily human clinical dose, suggesting maternal and fetal toxicity but not teratogenicity.
Clarithromycin has been shown to produce embryonic loss in monkeys when administered at approximately 10x the upper range of the usual daily human dose (500 mg twice daily), starting at gestation day 20. This effect has been attributed to maternal toxicity of the drug at very high doses. An additional study in pregnant monkeys at dosages of approximately 2.5-5 times the maximal intended daily dosage produced no unique hazard to the conceptus.
A dominant lethal test in mice given 1,000 mg/kg/day (approximately 70 times the maximal human daily clinical dose) was clearly negative for any mutagenic activity and in a segment I study of rats treated with up to 500 mg/kg/day (approximately 35 times the maximal daily human clinical dose) for 80 days, no evidence of functional impairment of male fertility due to this long-term exposure to these very high doses of clarithromycin was exhibited.
Mutagenicity: Studies to evaluate the mutagenic potential of clarithromycin were performed using both non-activated and rat liver-microsome-activated test systems (Ames Test). Results of these studies provided no evidence of mutagenic potential at drug concentrations of ≤25 mcg/Petri plate. At a concentration of 50 mcg the drug was toxic for all strains tested.
Microbiology: Clarithromycin has demonstrated excellent
in vitro activity against both standard strains of bacteria and clinical isolates. It is highly potent against a wide variety of aerobic and anaerobic gram-positive and gram-negative organisms. The minimum inhibitory concentrations (MICs) of clarithromycin are generally one log2 dilution more potent than the MICs of erythromycin.
In vitro data also indicate clarithromycin has excellent activity against
Legionella pneumophila and
Mycoplasma pneumonia. It is bactericidal to
Helicobacter pylori; this activity of clarithromycin is greater at neutral pH than at acid pH.
In vitro and
in vivo data show this antibiotic has activity against clinical significant mycobacterial species.
The
in vitro data indicate
Enterobacteriaceae, pseudomonas species and other non-lactose fermenting gram-negative bacilli are not susceptible to clarithromycin.
Clarithromycin has been shown to be active against most strains of the following organisms both
in vitro and in clinical infections as described in Indications.
Aerobic Gram-Positive Microorganisms: Staphylococcus aureus,
Streptococcus pneumoniae,
Streptococcus pyogenes,
Listeria monocytogenes.
Aerobic Gram-Negative Microorganisms: Haemophilus influenzae,
Haemophilus parainfluenzae,
Moraxella catarrhalis,
Neisseria gonorrhoeae,
Legionella pneumophila.
Other Microorganisms: Mycoplasma pneumonia,
Chlamydiapneumoniae (TWAR).
Mycobacteria: Mycobacterium leprae,
Mycobacterium kansasii,
Mycobacterium chelonae,
Mycobacterium avium complex (MAC) consisting of;
Mycobacterium avium,
Mycobacterium intracellulare.
β-lactamase production should have no effect on clarithromycin activity.
Note: Most strains of methicillin-resistant and oxacillin-resistant staphylococci are resistant to clarithromycin.
Helicobacter: Helicobacter pylori: In cultures performed prior to therapy,
H. pylori was isolated and clarithromycin MIC's were determined pretreatment in 104 patients. Of these, 4 patients had resistant strains, 2 patients had strains with intermediate susceptibility and 98 patients had susceptible strains.
The following
in vitro data are available, but their clinical significance is unknown. Clarithromycin exhibits
in vitro activity against most strains of the following microorganisms; however, the safety and effectiveness of clarithromycin in treating clinical infections due to these microorganisms have not been established in adequate and well-controlled clinical trials.
Aerobic Gram-Positive Microorganisms: Streptococcus agalactiae,
Streptococci (Group C,F,G),
Viridans group streptococci.
Aerobic Gram-Negative Microorganisms: Bordetella pertussis,
Pasteurella multocida.
Anaerobic Gram-Positive Microorganisms: Clostridium perfringens,
Peptococcus niger,
Propionibacterium acnes.
Anaerobic Gram-Negative Microorganisms: Bacteroides melaninogenicus.
Spirochetes: Borrelia burgdorferi, Treponema pallidum.
Campylobacter: Campylobacter jejuni.
The principal metabolite of clarithromycin in man and other primates is a microbiologically-active metabolite, 14-(OH)-clarithromycin. This metabolite is as active or 1- to 2-fold less active than the parent compound for most organisms, except for
H. influenzae against which it is twice as active. The parent compound and the 14-OH metabolite exert either an additive or synergistic effect on
H. influenzae in vitro and
in vivo, depending on bacterial strains.
Clarithromycin was found to be 2-10 times more active than erythromycin in several experimental animal infection models. It was shown, for example, to be more effective than erythromycin in mouse systemic infection, mouse SC abscess and mouse respiratory tract infections caused by
S. pneumoniae, S. aureus,
S. pyogenes and
H. influenzae. In guinea pigs with Legionella infection this effect was more pronounced; an intraperitoneal dose of 1.6 mg/kg/day of clarithromycin was more effective than 50 mg/kg/day of erythromycin.
Susceptibility Tests: Quantitative methods that require measurement of zone diameters give the most precise estimates of susceptibility of bacteria to antimicrobial agents. One recommended procedure uses discs impregnated with 15 mcg of clarithromycin for testing susceptibility (Kirby-Bauer diffusion test); interpretations correlate inhibition zone diameters of this disc test with MIC values for clarithromycin. The MIC's are determined by the broth or agar dilution method.
With these procedures, a report from the laboratory of "susceptible" indicates the infecting organism is likely to respond to therapy. A report of "resistant" indicates the infective organism is not likely to respond to therapy. A report of "Intermediate Susceptibility" suggests the therapeutic effect of the drug may be equivocal or the organism would be susceptible if higher doses were used. (Intermediate susceptibility is also referred to as moderately susceptible.)




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
