Pharmacology: Pharmacodynamics: Mechanism of action: Cytotoxic T lymphocyte-associated antigen (CTLA-4) is primarily expressed on the surface of T lymphocytes. Interaction of CTLA-4 with its ligands, CD80 and CD86, limits effector T-cell activation, through a number of potential mechanisms, but primarily by limiting co-stimulatory signalling through CD28.
Tremelimumab is a selective, fully human IgG2 antibody that blocks CTLA-4 interaction with CD80 and CD86, thus enhancing T-cell activation and proliferation, resulting in increased T-cell diversity and enhanced antitumour immune activity.
The combination of durvalumab, a PD-L1 inhibitor, and tremelimumab functions to enhance anti-tumour T-cell activation and function at multiple stages of the immune response, enhancing anti-tumour immunity.
The effect of STRIDE on the quantities of proliferative cytotoxic CD8+ T cells was evaluated in Study 22 in patients with uHCC using a CD8+Ki67+ assay. At Day 15 a marked increase of proliferating CD8+ T cell populations was observed in the STRIDE arm compared to the durvalumab monotherapy arm. Patients receiving STRIDE also experienced a higher Objective Response Rate (ORR) compared to other treatment arms and responders across all arms exhibited higher median proliferative cytotoxic CD8+ T cell when compared to non-responding patients.
Clinical efficacy and safety: HCC - HIMALAYA Study: The efficacy of STRIDE was evaluated in the HIMALAYA study, a randomised, open-label, multicenter study in patients with confirmed uHCC who did not receive prior systemic treatment for HCC. The study included patients with BCLC Stage C or B (not eligible for locoregional therapy) and Child-Pugh Score Class A.
The study excluded patients with brain metastases or a history of brain metastases, co-infection of viral hepatitis B and hepatitis C; active or prior documented GI bleeding within 12 months; ascites requiring non-pharmacologic intervention within 6 months; hepatic encephalopathy within 12 months before the start of treatment; active or prior documented autoimmune or inflammatory disorders. Patients with esophageal varices were included except those with active or prior documented GI bleeding within 12 months prior to study entry.
Randomisation was stratified by macrovascular invasion (MVI) (yes vs. no), etiology of liver disease (confirmed hepatitis B virus vs. confirmed hepatitis C virus vs. others) and ECOG performance status (0 vs. 1).
The HIMALAYA study randomized 1171 patients 1:1:1 to receive: D: durvalumab 1500 mg every 4 weeks; STRIDE: IMJUDO 300 mg as a single priming dose + durvalumab 1500 mg; followed by durvalumab 1500 mg every 4 weeks; S: Sorafenib 400 mg twice daily.
Tumour assessments were conducted every 8 weeks for the first 12 months and then every 12 weeks thereafter. Survival assessments were conducted every month for the first 3 months following treatment discontinuation and then every 2 months.
The primary endpoint was OS. Key secondary endpoints were PFS, Investigator assessed ORR and DoR according to RECIST v1.1. Patient-Reported Outcomes (PROs) were also assessed.
The demographics and baseline disease characteristics were generally representative for patients with uHCC. The baseline demographics of the overall study population were as follows: male (83.7%), age <65 years (50.4%), white (44.6%), Asian (50.7%), black or African American (1.7%), other (2.3%), ECOG PS 0 (62.6%); Child-Pugh Class score A (99.5%), macrovascular invasion (25.2%), extrahepatic spread (53.4%), viral etiology; hepatitis B (30.6%), hepatitis C (27.2%), uninfected (42.2%), baseline AFP < 400 ng/ml (63.7%), baseline AFP ≥ 400 ng/ml (34.5%), viral aetiology; hepatitis B (30.6%), hepatitis C (27.2%), uninfected (42.2%), evaluable PD-L1 data (86.3%), PD-L1 Tumour area positivity (TAP) ≥ 1% (38.9%), PD-L1 TAP < 1% (48.3%) [Ventana PD-L1 (SP263) assay].
The study demonstrated a statistically significant and clinically meaningful improvement in OS with STRIDE vs. S [HR=0.78 [95% CI 0.66, 0.92]; p=0.0035].
See Table 1 and figure.
 Click on icon to see table/diagram/image
Pharmacokinetics:
Click on icon to see table/diagram/image
Pharmacokinetics: The pharmacokinetics (PK) of tremelimumab was assessed for IMJUDO in combination with durvalumab.
The pharmacokinetics of tremelimumab was studied in patients with solid tumours at a single priming dose of 300 mg.
There was no clinically meaningful difference between the PK of tremelimumab as monotherapy or in combination with durvalumab.
Special populations: Age (18-87 years), body weight (34-149 kg), gender, positive anti-drug antibody (ADA) status, albumin levels, LDH levels, creatinine levels, tumour type, race, mild renal impairment (creatinine clearance (CRCL) 60 to 89 mL/min), moderate renal impairment (creatinine clearance (CRCL) 30 to 59 mL/min), mild hepatic impairment (bilirubin ≤ ULN and AST > ULN or bilirubin > 1.0 to 1.5 × ULN and any AST), moderate hepatic impairment (bilirubin > 1.5 to 3 x ULN and any AST) or ECOG/WHO status had no clinically significant effect on the PK of tremelimumab.
The effect of severe renal impairment (CRCL 15 to 29 mL/min) or severe hepatic impairment (bilirubin > 3.0 x ULN and any AST) on the PK of tremelimumab is unknown.
Elderly: No dose adjustment is required for elderly patients (≥ 65 years of age). Of the 462 patients with uHCC treated with STRIDE, 173 (37.4%) patients were 65 years or older and 63 (13.6%) patients were 75 years or older. No overall clinically meaningful differences in safety or efficacy were reported between patients ≥ 65 years of age and younger patients.
Immunogenicity: As with all therapeutic proteins, there is a potential for immunogenicity. Immunogenicity of tremelimumab is based on pooled data in 2075 patients who were treated with IMJUDO 75 mg or 1 mg/kg and evaluable for the presence of anti-drug antibodies (ADAs). Two-hundred fifty-two patients (12.1%) tested positive for treatment-emergent ADAs. Neutralizing antibodies against tremelimumab were detected in 10.0% (208/2075) patients. The presence of ADAs did not impact tremelimumab pharmacokinetics, and there was no apparent effect on efficacy and safety.
In the HIMALAYA study, of the 182 patients who were treated with STRIDE and evaluable for the presence of ADAs against tremelimumab, 20 (11.0%) patients tested positive for treatment-emergent ADAs. Neutralizing antibodies against tremelimumab were detected in 4.4% (8/182) patients. The presence of ADAs did not have an apparent effect on pharmacokinetics or safety.
Immunogenicity assay results are highly dependent on several factors, including assay sensitivity and specificity, assay methodology, sample handling, timing of sample collection, concomitant medications and underlying disease.
For these reasons, comparison of incidence of antibodies to tremelimumab with the incidence of antibodies to other products may be misleading.
Toxicology: Preclinical safety data: Carcinogenicity and mutagenicity: The carcinogenic and genotoxic potential of tremelimumab has not been evaluated.
Reproductive toxicology: Animal fertility studies have not been conducted with tremelimumab. In reproduction studies, administration of tremelimumab to pregnant cynomolgus monkeys during the period of organogenesis was not associated with maternal toxicity or effects on pregnancy losses, foetal weights, or external, visceral, skeletal abnormalities or weights of selected foetal organs at exposure levels approximately 4 to 31-times higher than those observed at a recommended dose range of 75 mg to 300 mg based on area under the curve (AUC).
Animal toxicology and/or pharmacology: In the chronic six-month toxicity study in cynomolgus monkeys, weekly intravenous administration of tremelimumab was associated with dose-related incidence in persistent diarrhoea and skin rash, scabs and open sores, which were dose-limiting. These clinical signs were also associated with decreased appetite and body weight and swollen peripheral lymph nodes. Histopathological findings correlating with the observed clinical signs included reversible chronic inflammation in the cecum and colon, and mononuclear cell infiltration in a wide variety of tissues including the skin and lymphoid tissues, with dose-related incidence and severity.
A dose-dependent increase in the incidence and severity of mononuclear cell infiltration with or without mononuclear cell inflammation was observed in the salivary gland, pancreas (acinar), thyroid, parathyroid, adrenal, heart, esophagus, tongue, periportal liver area, skeletal muscle, prostate, uterus, pituitary, eye (conjunctiva, extra ocular muscles), and choroid plexus of the brain. No observed adverse effect level (NOAEL) was found in this study with animals treated with the lowest dose of 5 mg/kg/week, however the intermediate dose of 15 mg/kg week was considered the highest non-severely toxic dose (HNSTD). This dose provided an exposure-based safety margin of 1.77 to clinical relevant exposure.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image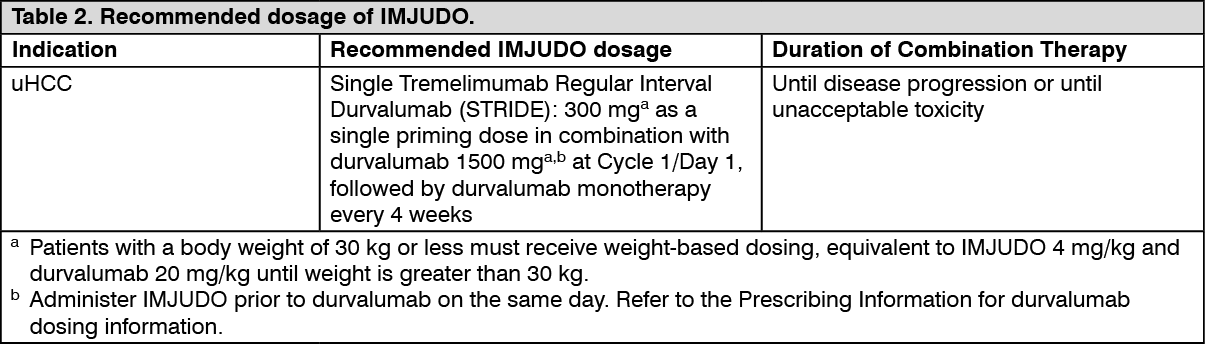 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
