In the two-chamber cartridge, there is a white powder in the front compartment and a clear solution in the rear compartment. After reconstitution, one cartridge contains 5.3 mg (16 IU) somatropin in 1 mL. The two-chamber cartridge is supplied for use sealed in a disposable multidose pre-filled pen (GoQuick).
Excipients/Inactive Ingredients: Powder: Front compartment: Glycine, Sodium dihydrogen phosphate anhydrous, Disodium phosphate anhydrous, Mannitol.
Solvent: Rear compartment: Water for injections, m-Cresol, Mannitol.
Pharmacology: Pharmacodynamics: Somatropin is a potent metabolic hormone of importance for the metabolism of lipids, carbohydrates and proteins. In children with inadequate endogenous growth hormone, somatropin stimulates linear growth and increases growth rate. In adults, as well as in children, somatropin maintains a normal body composition by increasing nitrogen retention and stimulation of skeletal muscle growth, and by mobilization of body fat. Visceral adipose tissue is particularly responsive to somatropin. In addition to enhanced lipolysis, somatropin decreases the uptake of triglycerides into body fat stores. Serum concentrations of IGF-I (Insulin-like Growth Factor-I) and IGFBP3 (Insulin-like Growth Factor Binding Protein 3) are increased by somatropin. In addition, the following actions have been demonstrated: Lipid metabolism: Somatropin induces hepatic LDL cholesterol receptors, and affects the profile of serum lipids and lipoproteins. In general, administration of somatropin to growth hormone deficient patients results in reductions in serum LDL and apolipoprotein B. A reduction in serum total cholesterol may also be observed.
Carbohydrate metabolism: Somatropin increases insulin but fasting blood glucose is commonly unchanged. Children with hypopituitarism may experience fasting hypoglycemia. This condition is reversed by somatropin.
Water and mineral metabolism: Growth hormone deficiency is associated with decreased plasma and extracellular volumes. Both are rapidly increased after treatment with somatropin. Somatropin induces the retention of sodium, potassium and phosphorus.
Bone metabolism:
Somatropin stimulates the turnover of skeletal bone. Long-term administration of somatropin to growth hormone deficient patients with osteopenia results in an increase in bone mineral content and density at weight-bearing sites.
Physical capacity: Muscle strength and physical exercise capacity are improved after long-term treatment with somatropin. Somatropin also increases cardiac output, but the mechanism has yet to be clarified. A decrease in peripheral vascular resistance may contribute to this effect.
Pharmacokinetics: Absorption: The bioavailability of subcutaneously administered somatropin is approximately 80% in both healthy subjects and growth hormone deficient patients. Results were comparable in both male and female patients. A subcutaneous dose of 0.035 mg/kg of somatropin results in plasma Cmax and tmax values in the range of 13-35 ng/mL and 3-6 hours, respectively.
In healthy adult males, following an SC injection in the thigh of 0.03 mg/kg, the extent of absorption (AUC) of a concentration of 5.3 mg/mL somatropin was 35% greater than that for 1.3 mg/mL somatropin. The mean (± standard deviation) peak (Cmax) serum levels were 23.0 (± 9.4) ng/mL and 17.4 (± 9.2) ng/mL, respectively.
In a similar study involving pediatric GHD patients, 5.3 mg/mL somatropin yielded a mean AUC that was 17% greater than that for 1.3 mg/mL somatropin. The mean Cmax levels were 21.0 ng/mL and 16.3 ng/mL, respectively.
Adult GHD patients received two single SC doses of 0.03 mg/kg of somatropin at a concentration of 1.3 mg/mL, with a one- to four-week washout period between injections. Mean Cmax levels were 12.4 ng/mL (first injection) and 12.2 ng/mL (second injection), achieved at approximately six hours after dosing.
There are no data on the bioequivalence between the 12-mg/mL formulation and either the 1.3-mg/mL or the 5.3-mg/mL formulations.
Distribution: The mean volume of distribution of somatropin following administration to GHD adults was estimated to be 1.3 (± 0.8) L/kg.
Metabolism: The metabolic fate of somatropin involves classical protein catabolism in both the liver and kidneys. In renal cells, at least a portion of the breakdown products are returned to the systemic circulation. The mean terminal half-life of intravenous somatropin in normal adults is 0.4 hours, whereas subcutaneously administered somatropin has a half-life of 3.0 hours in GHD adults. The observed difference is due to slow absorption from the subcutaneous injection site.
Excretion: The mean clearance of subcutaneously administered somatropin in 16 GHD adult patients was 0.3 (± 0.11) L/h/kg.
Special Populations: Pediatric: The pharmacokinetics of somatropin are similar in GHD pediatric and adult patients.
Gender: No gender studies have been performed in pediatric patients; however, in GHD adults, the absolute bioavailability of somatropin was similar in males and females.
Race: No studies have been conducted with somatropin to assess pharmacokinetic differences among races.
Renal, hepatic, or cardiac insufficiency: Information about the pharmacokinetics of somatropin in patients with renal, hepatic, or cardiac insufficiency is either lacking or incomplete.
Toxicology: Preclinical safety data: In studies regarding general toxicity, local tolerance and reproduction toxicity, no clinically relevant effects have been observed.
In vitro and in vivo genotoxicity studies on gene mutations and induction of chromosome aberrations have been negative.
An increased chromosome fragility has been observed in one in-vitro study on lymphocytes taken from patients after long-term treatment with somatropin and following the addition of the radiomimetic drug bleomycin. The clinical significance of this finding is unclear.
In another study, no increase in chromosomal abnormalities was found in the lymphocytes of patients who had received long-term somatropin therapy.
Children: Growth disturbance due to insufficient secretion of growth hormone and growth disturbance associated with Turner syndrome.
Adults: Replacement therapy in adults with pronounced growth hormone deficiency.
The dosage and administration schedule should be individualized. Somatropin should be given subcutaneously and the injection site varied to prevent lipoatrophy.
Growth disturbance due to insufficient secretion of growth hormone in children: Generally, a dose of 0.07-0.10 IU/kg (0.025-0.035 mg/kg) body weight per day or 2.1-3.0 IU/m
2 (0.7-1.0 mg/m
2) body surface area per day is recommended. Even higher doses have been used.
Growth disturbance due to Turner syndrome: A dose of 0.14 IU/kg (0.045-0.050 mg/kg) body weight per day or 4.3 IU/m
2 (1.4 mg/m
2) body surface area per day is recommended. (See Table 1).
 Click on icon to see table/diagram/image
Growth hormone deficient adult patients:
Click on icon to see table/diagram/image
Growth hormone deficient adult patients: The recommended starting dose is 0.45 - 0.90 IU (0.15 - 0.30 mg) per day. The final dose should be individually titrated as needed with respect to age and gender. The daily maintenance dose seldom exceeds 4 IU (1.33 mg) per day. Women may require higher doses than men. This means that there is a risk that women, especially those on oral oestrogen replacement may be under-treated. As normal physiological growth hormone production decreases with age, dose requirements may be reduced. Clinical response, side effects, and determination of IGF-I in serum may be used as guidance for dose titration. (See Table 2).
Click on icon to see table/diagram/image
Acute overdosage could lead initially to hypoglycemia and subsequently to hyperglycemia. Long-term overdosage could result in signs and symptoms consistent with the effects of human growth hormone excess.
Somatropin is contraindicated in patients who have evidence of neoplastic activity and in patients with uncontrolled growth of benign intracranial tumors. Anti-tumor therapy must be completed prior to starting somatropin.
Somatropin is contraindicated in patients with acute critical illness due to complications following open heart or abdominal surgery, multiple accidental trauma, or acute respiratory failure. Two placebo-controlled clinical trials (N=522), conducted in adult patients to evaluate the effects of somatropin 5.3 or 8 mg (16 or 24 IU) on length of stay in intensive care units, showed significantly higher mortality (41.9% vs. 19.3%) in patients treated with somatropin compared with those who received placebo (see Precautions in patients who are receiving somatropin for growth hormone replacement).
Hypersensitivity to the active substance or to any of the excipients.
Diagnosis and therapy with somatropin should be initiated and monitored by physicians who are appropriately qualified and experienced in the diagnosis and management of patients with the therapeutic indication of use.
Myositis is a very rare adverse event that may be related to the preservative m-cresol. If myalgia or disproportionate pain at injection site develops, myositis should be considered and, if confirmed, a presentation of somatropin without m-cresol should be used.
Somatropin may induce a state of insulin resistance and, in some patients, hyperglycemia. Therefore, patients should be observed for evidence of glucose intolerance. In rare cases, therapy with somatropin may produce sufficient glucose intolerance to meet the diagnostic criteria for Type 2 diabetes mellitus. The risk of developing diabetes during treatment with somatropin is greatest in those patients with other risk factors for Type 2 diabetes mellitus, such as obesity, family history of diabetes, treatment with steroids, or prior impaired glucose tolerance. In patients with pre-existing diabetes mellitus, the dose of anti-diabetic therapy might require adjustment when somatropin is instituted.
In general, peripheral thyroid hormone levels remain within the normal reference range during treatment with somatropin. However, there is an enhanced conversion of T4 to T3 that may result in a reduction in serum T4 and an increase in serum T3 concentrations. This effect may be of clinical relevance for patients with central subclinical hypothyroidism in whom hypothyroidism may theoretically develop. Conversely, mild hyperthyroidism may occur in patients receiving replacement therapy with thyroxin. It is therefore, advisable to test thyroid function shortly after the start of treatment with somatropin, and after dose adjustments.
Introduction of somatropin treatment may result in inhibition of 11β-hydroxysteroid dehydrogenase type 1 (11β-HSD-1) and reduced serum cortisol concentrations. In patients treated with somatropin, previously undiagnosed central (secondary) hypoadrenalism may be unmasked and glucocorticoid replacement may be required. In addition, patients treated with glucocorticoid replacement therapy for previously diagnosed hypoadrenalism may require an increase in their maintenance or stress doses, following initiation of somatropin treatment (see Interactions).
If a woman taking somatropin begins oral oestrogen therapy, the dose of somatropin may need to be increased to maintain the serum insulin-like growth factor-I (IGF-I) levels within the normal age-appropriate range. Conversely, if a woman on somatropin discontinues oral oestrogen therapy, the dose of somatropin may need to be reduced to avoid excess of growth hormone and/or side effects (see Interactions).
In patients with growth hormone deficiency secondary to treatment of malignant disease, it is recommended to monitor for signs of relapse of the malignancy.
In patients with endocrine disorders, including growth hormone deficiency, slipped epiphyses of the hip may occur more frequently than in the general population. Children who develop a limp during treatment with somatropin should be evaluated (see Adverse Reactions).
In case of severe or recurrent headache, visual problems, nausea, or vomiting, a funduscopy for papilledema is recommended. If papilledema is confirmed, a diagnosis of benign intracranial hypertension should be considered and, if appropriate, growth hormone treatment should be discontinued. At present, there is insufficient evidence to guide the decision of whether or not to reintroduce growth hormone therapy in patients with resolved intracranial hypertension. If growth hormone treatment is restarted, careful monitoring for symptoms of intracranial hypertension is necessary.
Progression of scoliosis can occur in patients who experience rapid growth. Because growth hormone increases growth rate, physicians should be alert to this abnormality, which may manifest during growth hormone therapy.
Experience in patients above 60 years is limited.
In patients with chronic renal insufficiency, renal function should be below 50% of normal before institution of therapy with somatropin. To verify growth disturbance, growth should be followed for a year preceding institution of therapy. Conservative treatment for renal insufficiency should have been established and should be maintained during therapy with growth hormone. Somatropin should be discontinued at renal transplantation.
If patients who are receiving growth hormone replacement therapy become acutely critically ill, the potential benefit of continued treatment with somatropin should be weighed against the potential risk (see Contraindications).
Somatropin is ineffective for growth promotion in children with closed epiphyses.
Effects on ability to drive and use machines: No effects on the ability to drive and use machines have been observed.
Animal reproduction studies have not shown evidence of harmful effects on the fetus. There are, however, no studies in pregnant women. Treatment with Genotropin should be interrupted if pregnancy occurs.
During normal pregnancy, the levels of pituitary growth hormone markedly fall after Week 20 of gestation, being replaced almost entirely by placental growth hormone by Week 30. Therefore, it is unlikely that continued replacement therapy with somatropin would be necessary in growth hormone deficient women during the third trimester of pregnancy.
It is not known if somatropin is excreted into breast milk, but absorption of intact protein from the gastrointestinal tract of the infant is extremely unlikely.
Patients with growth hormone deficiency are characterized by extracellular volume deficit. When treatment with somatropin is started, this deficit is rapidly corrected. In general, in adult patients, adverse effects related to fluid retention, such as edema peripheral, face edema, musculoskeletal stiffness, arthralgia, myalgia and paresthesia are mild to moderate, arise within the first months of treatment, and subside spontaneously or with dose-reduction.
The incidence of these adverse effects is related to the administered dose, the age of the patients, and possibly inversely related to the age of the patients at the onset of growth hormone deficiency.
Tabulated list of adverse reactions: Tables 3-5 show the adverse reactions ranked under headings of System Organ Class and frequency using the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data) for each of the indicated conditions. (See Tables 3, 4 and 5).
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Transient injection site reactions in children have been reported.
Somatropin has been reported to reduce serum cortisol levels, possibly by affecting carrier proteins or by increased hepatic clearance. The clinical relevance of these findings may be limited. Nevertheless, corticosteroid replacement therapy should be optimized before initiation of Genotropin therapy.
Rare cases of leukemia have been reported in growth hormone deficient children treated with somatropin, but the incidence appears to be similar to that in children without growth hormone deficiency.
Slipped capital femoral epiphysis and Legg-Calve-Perthes disease have been reported in children treated with growth hormone. But, it is unknown if these 2 pathologies are more frequent or not while treated with somatropin.
Concomitant treatment with glucocorticoids inhibits the growth-promoting effects of somatropin containing products. Patients with adrenocorticotropic hormone (ACTH) deficiency should have their glucocorticoid replacement therapy carefully adjusted to avoid any inhibitory effect on growth. Therefore, patients treated with glucocorticoids should have their growth monitored carefully to assess the potential impact of glucocorticoid treatment on growth.
Growth hormone decreases the conversion of cortisone to cortisol and may unmask previously undiscovered central hypoadrenalism or render low glucocorticoid replacement doses ineffective (see Precautions).
Administration of somatropin may increase the clearance of compounds metabolized by cytochrome P4503A4 (e.g. sex steroids, corticosteroids, anticonvulsants, and cyclosporin). The clinical significance of this potential interaction is unknown.
In women on oral oestrogen replacement, a higher dose of growth hormone may be required to achieve the treatment goal (see Precautions).
Incompatibilities: This medical product must not be mixed with other medical products and should only be reconstituted in the supplied solvent.
Special precautions for disposal and other handling: Two-chamber cartridge: The solution is prepared by screwing the GoQuick pre-filled pen sections together so that the solvent will be mixed with the powder in the two-chamber cartridge. Gently dissolve the powder with a slow, swirling motion. Do not shake vigorously; this might cause denaturation of the active ingredient. The reconstituted solution is almost colorless or slightly opalescent. The reconstituted solution for injection is to be inspected prior to use and only clear solutions without particles should be used.
Empty GoQuick pre-filled pens should never be refilled and must be properly discarded.
Before reconstitution: Store in a refrigerator (2°C - 8°C), with up to 1 month at or below 25°C allowed. Keep container in the outer carton in order to protect from light.
After reconstitution: Store in a refrigerator (2°C - 8°C). Do not freeze. Keep container in the outer carton in order to protect from light.
Shelf-life: After reconstitution, chemical and physical in-use stability at 2°C - 8°C has been demonstrated for 4 weeks.
From a microbiological point of view, once reconstituted, the product may be stored at 2°C - 8°C for 4 weeks.
Other in-use storage times and conditions are the responsibility of the user.
H01AC01 - somatropin ; Belongs to the class of somatropin and somatropin agonists. Used in anterior pituitary lobe hormone and analogue preparations.
Genotropin powd for soln for inj 16 IU (5.3 mg)
([GoQuick pre-filled pen (2-chamber cartridge)] + solvent 1.15 mL x 1's) 1's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image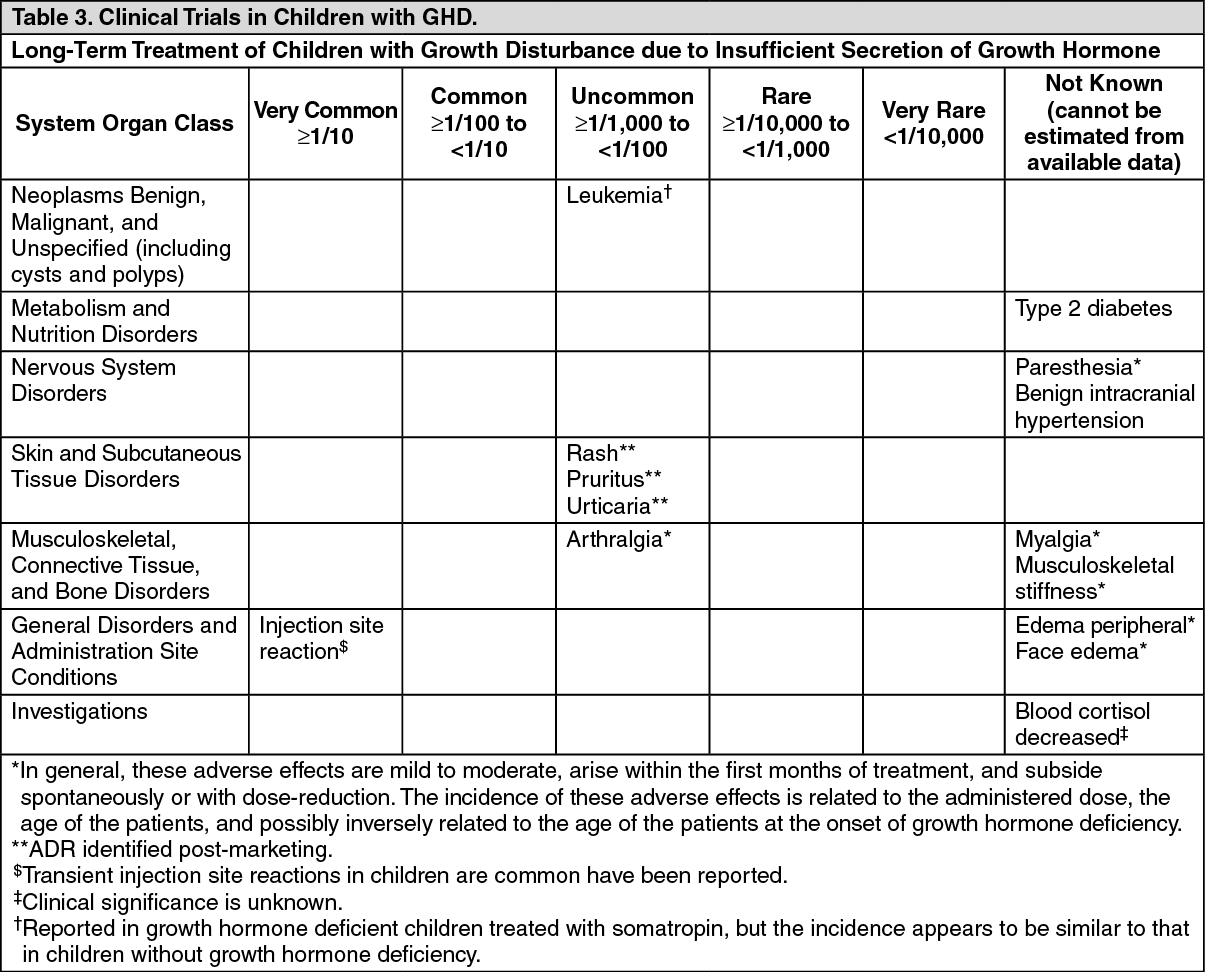 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image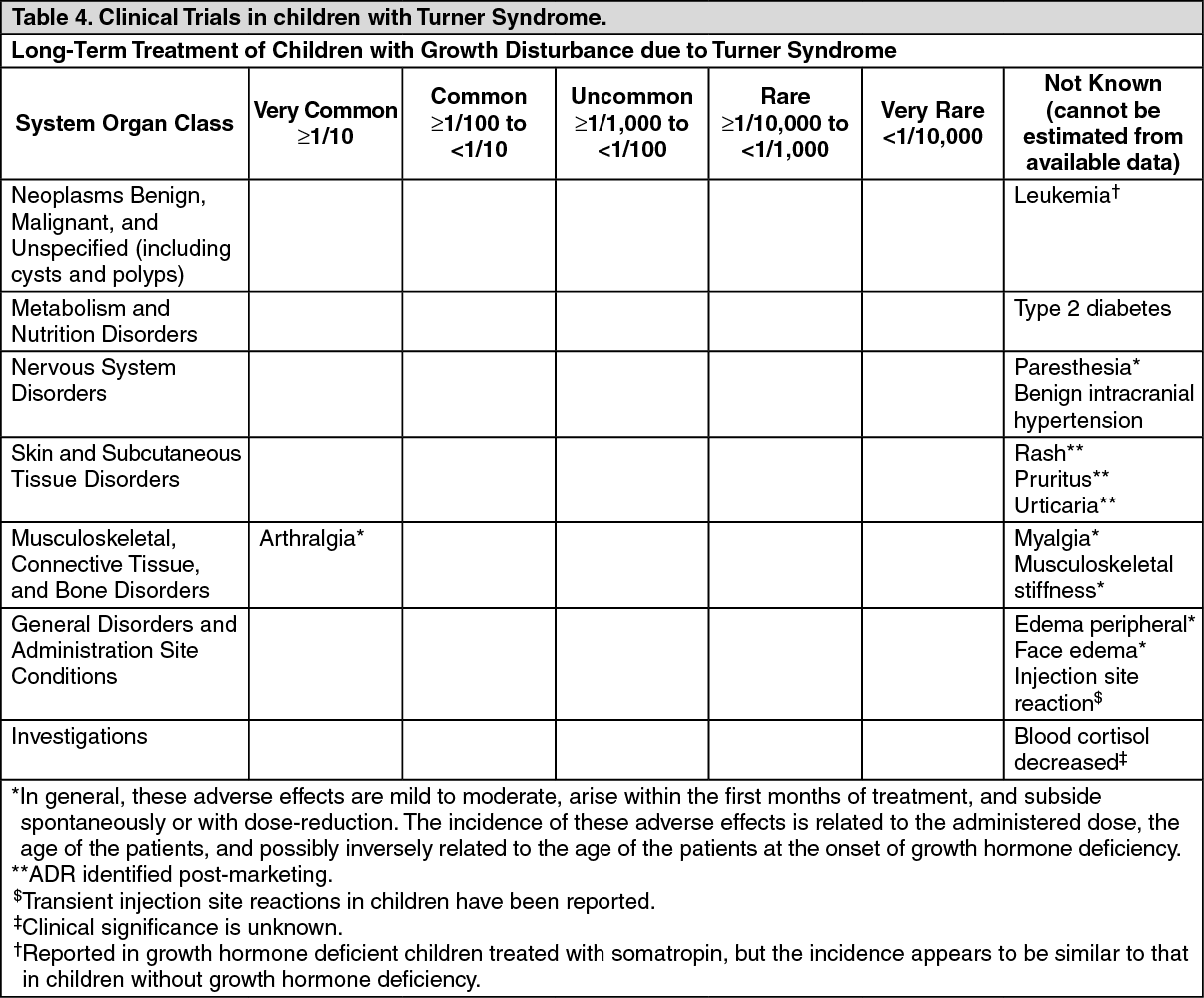 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image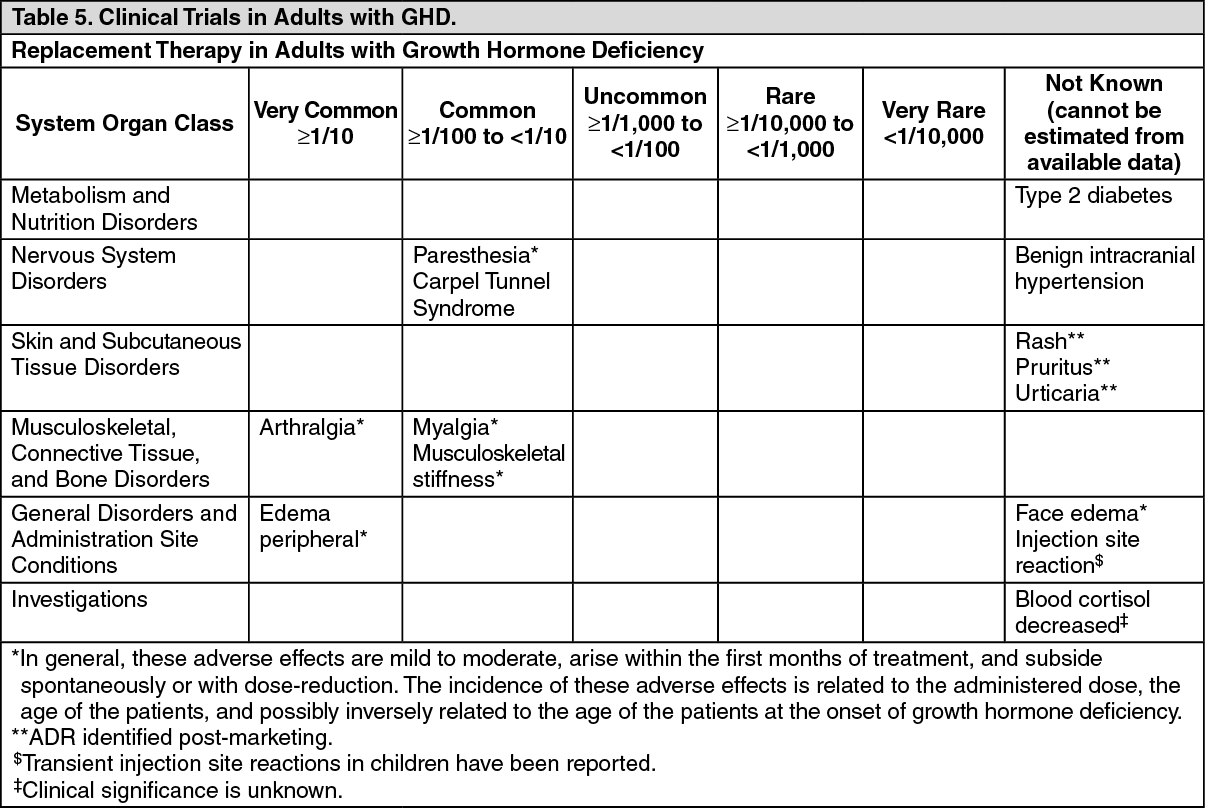 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image43b0c190-b452-4872-a11a-9faa0140dd14.GIF)

 Sign Out
Sign Out
